
記住我

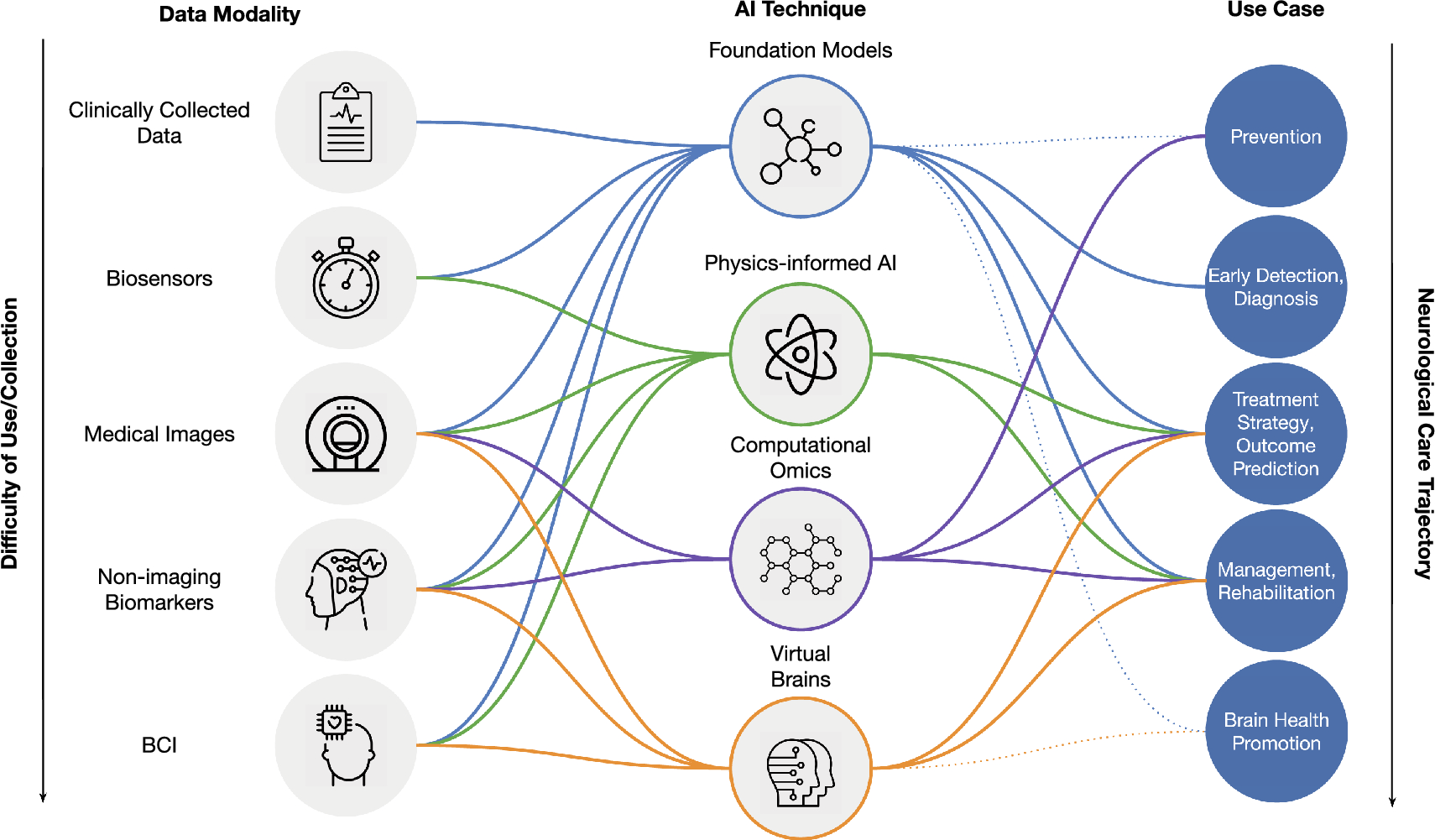
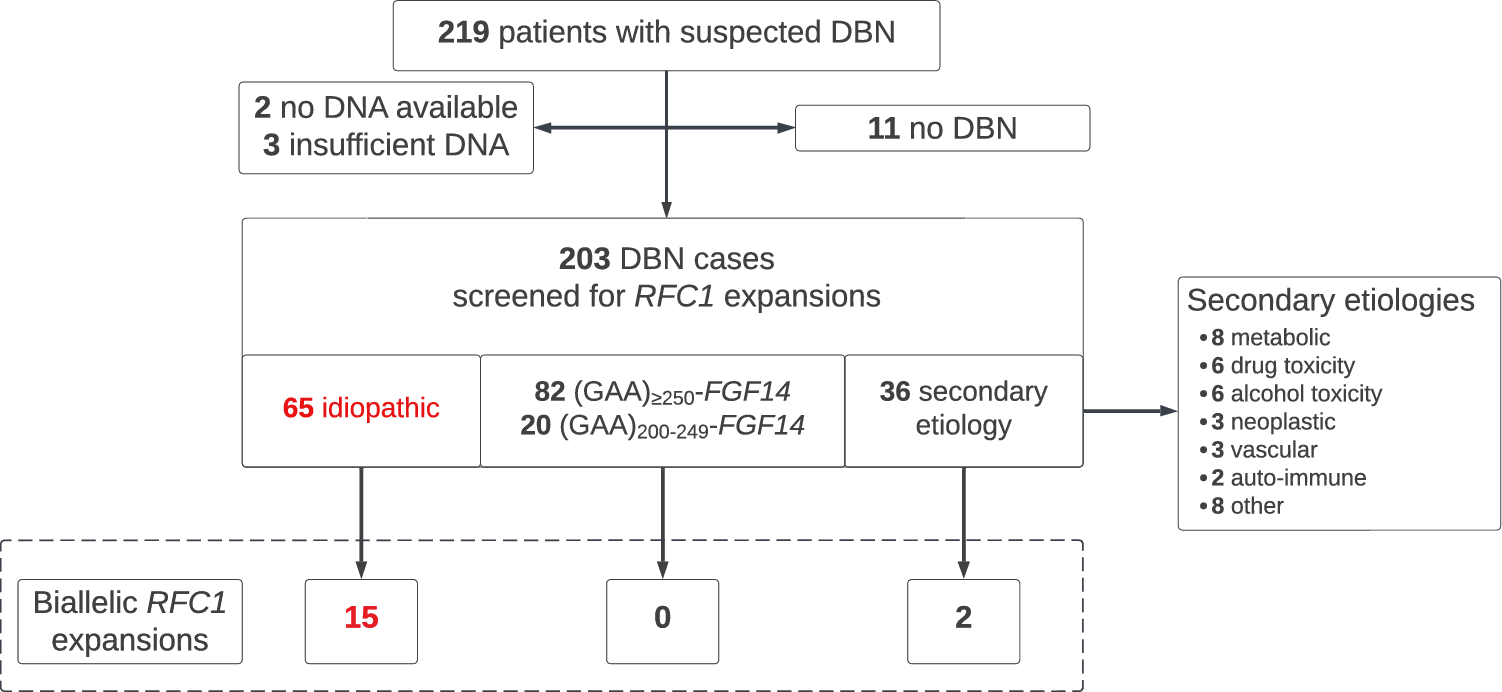
Biallelic RFC1 AAGGG repeat expansions were identified in 15 of 65 (23%) patients with “idiopathic” DBN (Figs.1 and 2A). Moreover, a high frequency of heterozygous RFC1 repeat expansion carriers was observed in the “idiopathic” DBN cohort (12%, 8/65 patients / 6.2%, 8/130 allele frequency; compared to 0.7–6.5% carrier frequency in the general population [13]). A total of 50 patients remained unsolved after RFC1 screening, and will be referred to onward as “genetically unexplained”. In addition, 2 of the 36 (6%) patients with presumed secondary DBN were found to carry biallelic RFC1 AAGGG repeat expansions, while none of the 102 (GAA)≥200-FGF14-positive patients did (Fig. 1).
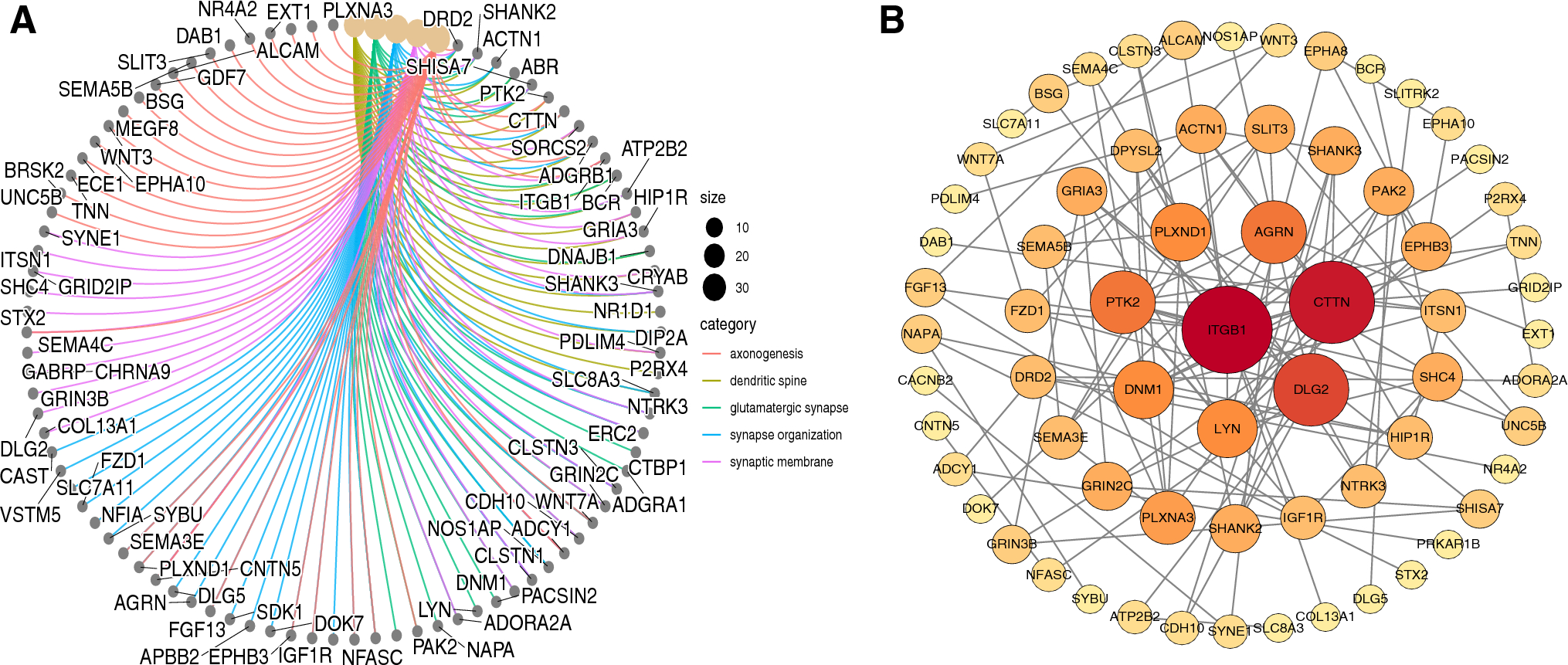
Fig. 2
Frequency of RFC1 repeat expansions in DBN syndromes and progression of functional disability in the RFC1-related DBN syndrome. A Percentage of patients carrying biallelic RFC1 AAGGG repeat expansions in a cohort of 65 patients with idiopathic downbeat nystagmus (DBN). B Percentage of patients carrying biallelic RFC1 AAGGG repeat expansions in the phenotypic subgroups with (1) pure DBN, (2) DBN plus cerebellar impairment (DBN + C), (3) DBN plus cerebellar impairment and bilateral vestibulopathy (DBN + C + BVP), (4) DBN plus cerebellar impairment and polyneuropathy (DBN + C + N), and (5) DBN plus cerebellar impairment, BVP, and polyneuropathy (DBN + C + BVP + N). No patient with DBN plus isolated BVP or isolated neuropathy was identified among the idiopathic DBN cohort. C Disease duration at time of onset of regular use of walking aid and regular falls in the RFC1-positive patients with DBN. D Longitudinal intra-individual progression of functional impairment as assessed by the FARS functional disability stage relative to disease duration (35 observations from 11 patients with DBN carrying biallelic RFC1 repeat expansions). Observations from the same patient are connected by a dotted line. The FARS functional stage assesses disability through a 7-point ordinal scale: 0 = normal; 1 = minimal signs on examination; 2 = minimal disability; 3 = mild disability; 4 = moderate disability, requires a walker; 5 = severe disability, confined but can navigate a wheelchair; 6 = total disability
Phenotypic characterization of the RFC1-related DBN syndromeThe frequency of biallelic RFC1 repeat expansions stratified by DBN subgroups was 50% (3/6) for DBN plus cerebellar impairment and BVP, and 86% (12/14) for DBN plus cerebellar impairment, BVP, and polyneuropathy (Fig. 2B). None of the patients in the other DBN subgroups carried biallelic RFC1 repeat expansions (Fig. 2B). Table 1 presents the clinical features of the RFC1-positive, (GAA)≥200-FGF14-positive, and genetically unexplained DBN cohorts.
Table 1 Characteristics and discriminative features of the RFC1-related downbeat nystagmus syndromeDBN occurred with cerebellar impairment in all 15 RFC1-positive patients, which was limited to the ocular motor system with typical cerebellar ocular motor signs (i.e., saccadic pursuit, dysmetric saccades, gaze-evoked nystagmus) in 5 patients (33%). Additional cerebellar ocular motor signs were observed in all RFC1-positive patients. Brain MRI showed global cerebellar atrophy in 27% (3/11) and isolated vermis atrophy in 9% (1/11) of patients. BVP was documented in all RFC1-positive patients by vHIT (n = 10) or caloric stimulation (n = 5). Polyneuropathy was identified in 12 of 15 (80%) RFC1-positive patients, and was diagnosed on NCS in six patients and clinically in six patients. Three patients had no evidence of neuropathic features on examination, though NCS were not available for these patients. The presence of chronic cough could not be reliably extracted from medical records, although it was documented in two patients in whom it developed more than 10 years before the onset of gait impairment.
Progression of functional disability in the RFC1-related DBN syndromeA substantial proportion of RFC1-positive patients experienced regular falls (89%, 8/9), some of them as early as 2.5 years after disease onset (median disease duration at onset of regular falls, 4 years; range, 2.5–7.5). Furthermore, walking aids were used by 50% of patients (7/14) after a median disease duration of 6.5 years (range, 2.5–18) (Fig. 2C). At time of last examination, the median Friedreich Ataxia Rating Scale (FARS) functional stage was 3.25 (range, 1.5–4), indicating a mild-to-moderate disability (Fig. 2D).
Discriminative features of the RFC1-related DBN syndromeCompared to (GAA)≥200-FGF14-positive and genetically unexplained patients with DBN, RFC1-positive patients with DBN appeared more functionally impaired, as assessed by the FARS functional stage, history of regular falls and use of walking aids, and gait impairment on examination (Table 1). However, the RFC1-positive DBN group also had a significantly longer disease duration compared to the genetically unexplained group (median, 7 vs 4 years; p = 0.007) and a trend toward longer disease duration compared to the (GAA)≥200-FGF14-positive group (median, 7 vs 6 years; p = 0.070), which may account in part for the higher degree of functional impairment in the RFC1-positive group. Neuropathic features and proprioceptive dysfunction on examination were significantly more common in the RFC1-positive group (Table 1), in keeping with early and preferential involvement of dorsal root ganglia in that disease [14]. Vestibular impairment was also significantly more common and severe, as measured by VOR gains on vHIT, in RFC1-positive patients (n = 9) compared to (GAA)≥200-FGF14-positive (n = 9) and genetically unexplained patients (n = 2) (Table 1).
留言 (0)