
記住我

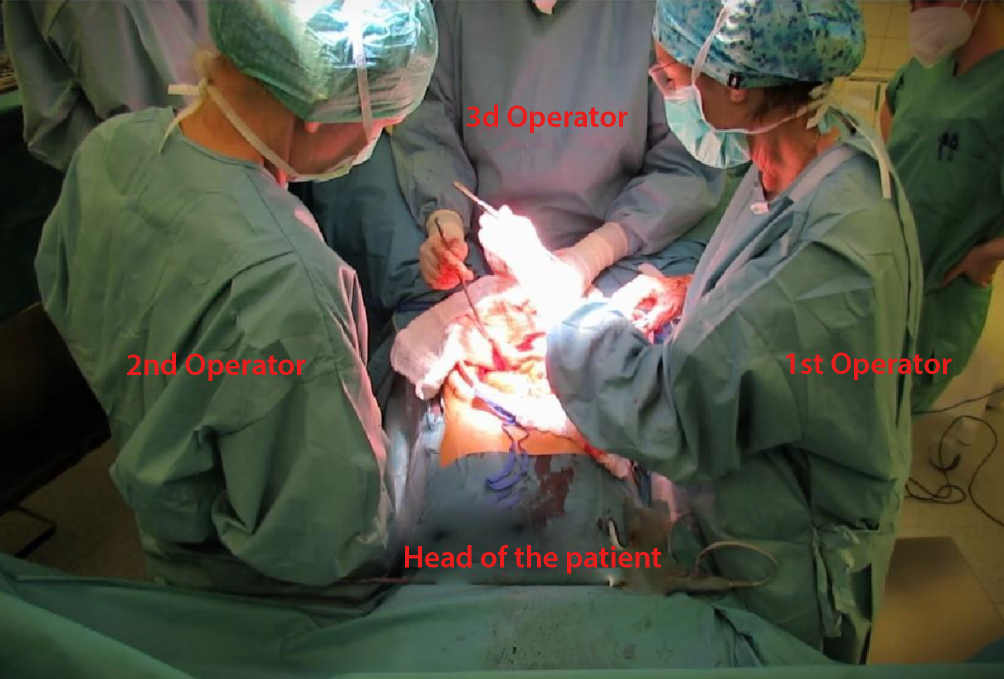
The patient is positioned on the operating table in a lithotomy position. In cases where the patient is undergoing resection of a previous ileoanal pouch, the legs should be abducted and supported by leg stirrups to provide access to the anorectal plane (Lloyd–Davies position, Fig. 1).
Fig. 1
Lloyd–Davies position, with abducted legs supported by leg stirrups
Step 1.Bowel measurement and incision for pouch creation. The initial stage involves precise measurement of the small intestine segment required to construct the pouch, typically 60 cm in length. Distinct marking sutures are placed at 15-cm intervals along this segment (Fig. 2). Subsequently, a longitudinal antimesenteric incision is performed on the bowel, sparing the proximal 15-cm segment. This intact portion is preserved for the subsequent construction of the valve and outlet mechanism of the pouch.
Fig. 2
Marking sutures at 15-cm intervals along the small intestine segment
Step 2.Repetition of measurements and S‑shaped pouch formation. This step involves repetition of the 60-cm small bowel measurement four times, integral to formation of the S‑shaped continent ileostomy (CI). At our center, we prefer this method due to its enhanced postoperative outcomes and the facilitation of endoscopic evaluation of the afferent loop. For creating precise antimesenteric incisions, it is often beneficial to employ suction or a rectal probe within the bowel lumen, ensuring the straightness and accuracy of these incisions (Fig. 3). This careful technique is crucial for successful formation of the S‑shaped structure of the pouch.
Fig. 3
Antimesenteric incisions; a rectal probe is employed within the bowel lumen
Step 3.In the subsequent stage of the procedure, we meticulously suture the posterior wall of the pouch, addressing each limb sequentially (Fig. 4). This critical step is executed using dual continuous full-thickness sutures composed of absorbable material, typically Polydioxanone (PDS; Johnson & Johnson, New Brunswick, NJ, USA). This technique effectively unites the three loops of the bowel, ensuring a robust and secure construction of the pouch’s posterior aspect.
Fig. 4
Full-thickness suture of the posterior wall of the pouch
Step 4.At this juncture, with particular emphasis on patients with a higher body mass index, the peritoneal layer covering the valve’s mesentery is meticulously excised in a triangular fashion on both sides (Fig. 5). This step is critical for ensuring optimal surgical outcomes in these patients.
Fig. 5
The visceral peritoneum of the valve mesentery is excised in a triangular fashion
Step 5.The nipple valve is meticulously constructed by intussuscepting the efferent limb into the developing reservoir (Fig. 6, Video 1). This is achieved using two to three Babcock clamps, which facilitate precise manipulation and alignment during the intussusception process.
Fig. 6
Intussusception of the efferent limb into the developing reservoir
Exercising meticulous care to avoid the mesentery, we employ a 60-mm knifeless linear cutter (Fig. 7) to secure the nipple valve, which measures approximately 4–5 cm in length. This process involves three precise applications of the cutter, ensuring durable and stable fixation of the bowel for the nipple valve (Fig. 8a.b).
Fig. 7
Cautious removal of the blade from the linear cutter
Fig. 8
a Fixation of the bowel for the nipple valve using the 60-mm linear cutter and avoiding the mesentery. b Final macroscopic result after application of the knifeless linear cutter
Following the valve’s construction, the final phase of pouch assembly involves the closure of its anterior wall. This critical step is executed using a continuous full-thickness absorbable suture (Fig. 9). Prior to finalizing the suture, an additional step is undertaken to secure the valve to the anterior wall of the pouch. In recent procedures, we have consistently utilized the closing suture line for this purpose. Subsequently, a seromuscular oversewing technique is meticulously performed to reinforce the structural integrity of the pouch.
Fig. 9
Full-thickness suture of the anterior wall of the pouch
At this stage, an assessment of continence is conducted (Fig. 10). This involves the introduction of a catheter through the nipple valve into the pouch, followed by cautious instillation of physiological saline solution. Subsequently, while maintaining the catheter in a clamped state, it is extracted to evaluate for complete continence (Video 2). In instances of any leakage, the affected areas must be meticulously oversewn to secure full continence of the reservoir. After this corrective step, the catheter is reinserted for the purpose of evacuating the instilled fluid.
Fig. 10
Continence test of the newly fashioned reservoir
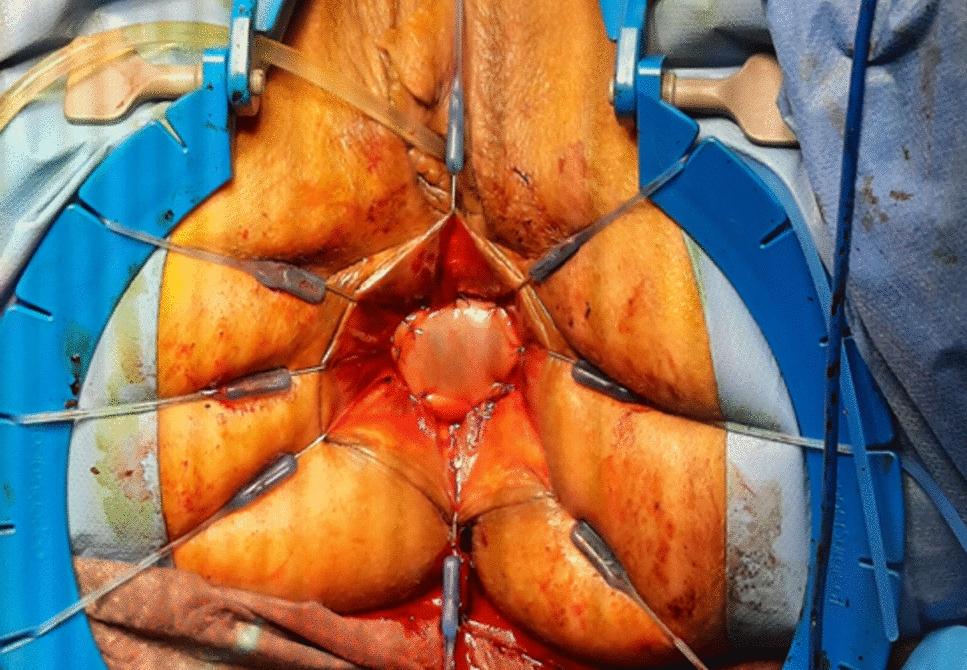
Following preparation of the stoma opening, attention is directed towards meticulous preparation of the outlet. A critical step involves securely affixing the collar of the pouch to the abdominal wall using non-absorbable sutures, specifically Prolene (Ethicon, Inc., Johnson & Johnson; Fig. 11). These sutures are strategically positioned between the collar of the pouch, in proximity to the mesentery, and the posterior sheath of the rectus muscle. Once all sutures have been precisely placed, they are individually tied. Subsequent to this procedure, a second continence evaluation is performed.
Fig. 11
The pouch’s collar is secured to the posterior sheath of the rectus muscle using a Prolene (Ethicon, Inc., Johnson & Johnson, New Brunswick, NJ, USA) suture
In the final stage of the procedure, an intraabdominal drainage is placed and the catheter is repositioned in the pouch. After final closure of the abdominal wall, the catheter is secured to the skin with three braided absorbable stitches; these will be removed in the early postoperative days (Fig. 12).
Fig. 12
The abdominal wall at the end of the procedure
留言 (0)