
記住我

This study retrospectively evaluated a consecutive series of multidisciplinary robotic resections for bowel DIE performed between January 2021 (opening of the Robotic Endometriosis Centre at The Princess Grace Hospital) and December 2022. Data were extracted from a prospectively maintained endometriosis database in a BSGE-accredited endometriosis centre.
Patients provided informed consent for prospective anonymized data collection for the BSGE national registry for research purpose (accreditation requirement).
The primary aim was to report perioperative outcomes of patients undergoing multidisciplinary resections. The secondary aim was to report dyschezia and QoL pre- and postoperatively (6 months).
Inclusion criteria were (1) robotic approach; (2) pararectal space dissection; (3) multidisciplinary approach involving colorectal surgeons with/without urologist; (4) endometriosis on histology; (5) age ≥ 18 years.
The was one exclusion criterion: no specialized colorectal surgeon.
MDT discussion and planningPreoperative staging workup included (Fig. 1) collection of symptoms, medical history, gynaecological examination (speculum/bimanual), and BSGE pelvic pain questionnaire completion. Faecal occult blood test, pelvic and transvaginal ultrasound, abdominopelvic magnetic resonance imaging, and colonoscopy were performed if indicated.
Fig. 1
Perioperative endometriosis management pathway. MDT*: includes gynaecologists, colorectal surgeons, urological robotic surgeons, anaesthetists, radiologists, nurse specialist (gynaecological and pain management), and database administrators. MDT§: includes general robotic surgeons, cardiothoracic surgeons, gastroenterologists, haematologists, psychologists, psychiatrists, psychosexual therapists, stoma nurses, pain consultants, fertility specialists, women’s health physiotherapy team, and dieticians. BSGE British Society for Gynaecological Endoscopy, CNS clinical nurse specialist, GnRH gonadotropin-releasing hormone, GP general practitioner, MDT multidisciplinary team
Surgery was offered when symptoms were unresponsive to medical treatment and was carefully discussed at an MDT meeting and with the patient. The MDT (including gynaecologists, colorectal surgeons, urologists, cardiothoracic surgeons, radiologists, gastroenterologists, psychologists, psychiatrists, psychosexual therapists, stoma nurses, women’s health physiotherapy team, nurse specialist (gynaecological and pain management), dieticians, database administrators and any other extended MDT members, if required) prepared a patient-tailored surgical plan. Fertility referral, GnRH analogues, and pain management were recommended if needed.
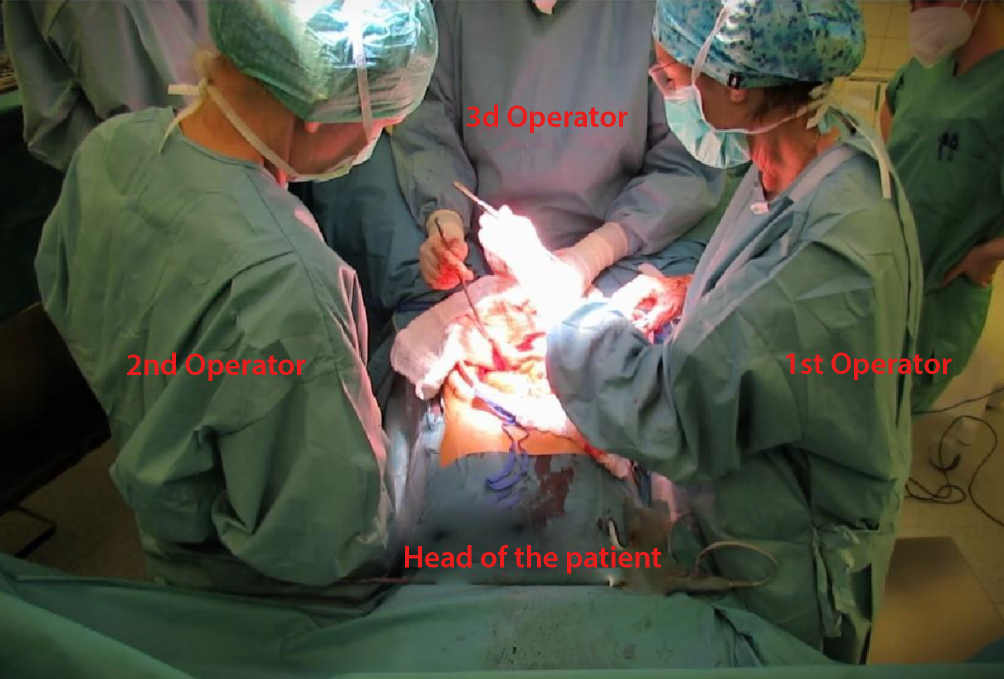
Surgical techniqueSurgeries were performed with the da Vinci Xi® platform with dual console by an MDT including gynaecologist, colorectal surgeon, and urologist with extensive expertise in minimally invasive surgery.
Mechanical bowel preparation and deep vein thrombosis prophylaxis were performed.
Lloyd-Davies position (22° head-down) was adopted. Pneumoperitoneum (10 mmHg) was obtained through Veress needle technique.
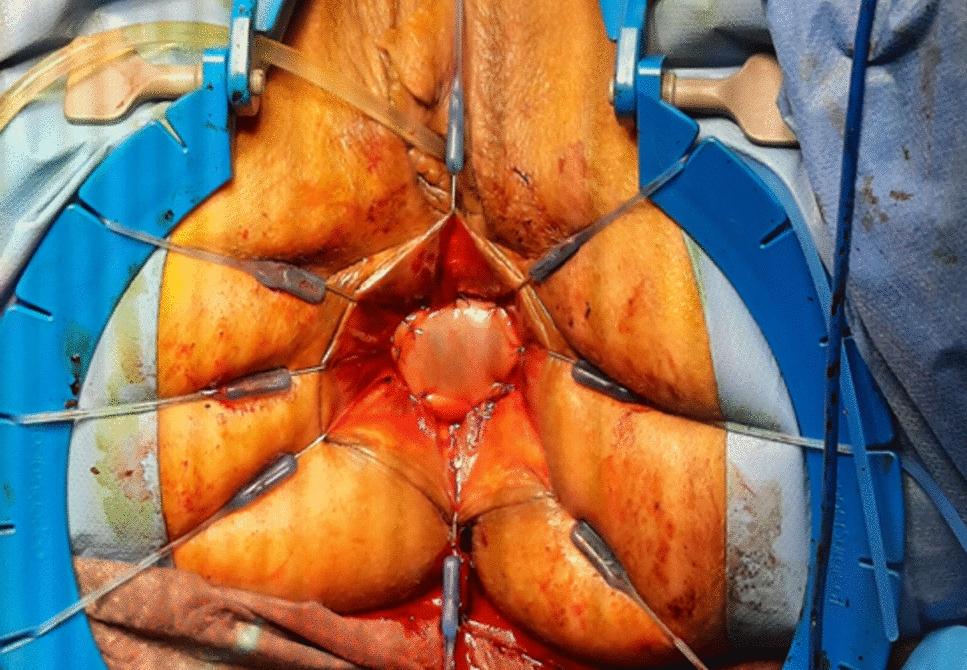
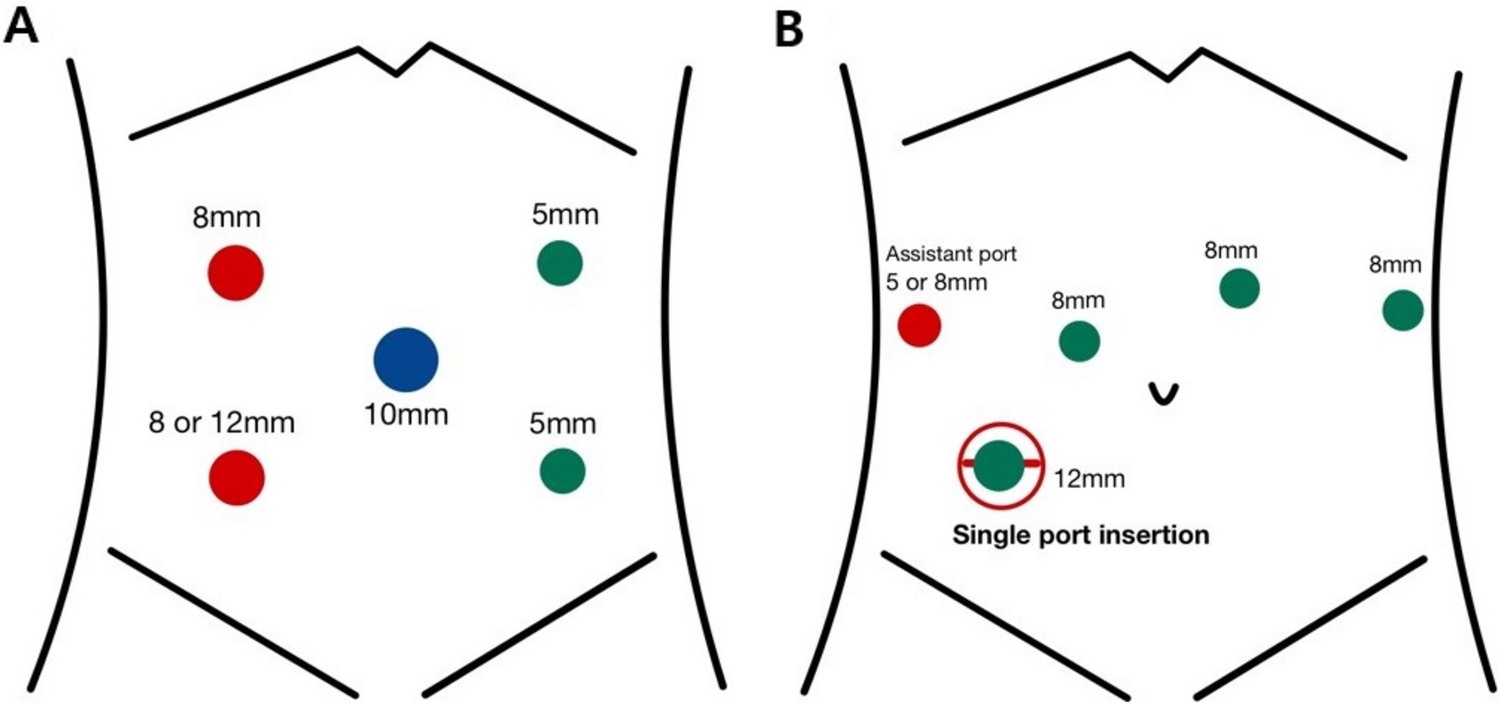
A five-port transverse approach (Fig. 2) was adopted with four robotic 8-mm trocars and one 8-mm AirSeal® access port (ConMed, Utica, NY, USA; used by the assistant for suction or traction). A single-docking fully robotic approach with a two right-hand setting was used: arm 1 (bipolar forceps), arm 2 (30° endoscope), arm 3 (monopolar scissors), arm 4 (Cadiere forceps). Second assistant used VCare® Plus (ConMed, Utica, NY, USA) intrauterine manipulator.
Fig. 2
Port and patient cart placement asset. As assistant port, ASIS anterior superior iliac spine, CM costal margin, PS pubic symphysis
dV3 monopolar and dV1 bipolar system (Intuitive Surgical, Inc., Sunnyvale, CA, USA) were used for energy devices. Monopolar setting was 3, cut auto (180 W max); 3, coag swift (150 W max). Bipolar setting was 3, auto (80 W max).
A gynaecologist performed adhesiolysis, drainage, and stripping of endometriomas. Resection varied according to disease location, extension, and patient’s fertility desire. Then, gynaecologists and colorectal surgeon together performed nodules resection with shaving, disc excision, or segmental resection according to number of lesions, location, contiguity, size, depth of infiltration, distance from the anal verge, and circumferential involvement. All dissections were performed with nerve-sparing technique. Shavings were performed with monopolar cut function and grouped in superficial shaving (serosa and outer third muscularis layer excision) and deep shaving (serosa with middle third muscularis layer excision with interrupted suture repair in single layer). For disc excision, the bowel wall including the nodule was resected with a transanal circular stapler. Segmental resection was performed with low ligation of the superior rectal artery at the level of DIE. All colorectal anastomoses were evaluated with a triple assessment using fluorescence (3 ml indocyanine green infusion), air leak, and endoscopic evaluation (“Portsmouth protocol”) [29].
Conversion was defined as unintended extension of the suprapubic extraction site incision.
Postoperative follow-upAll specimens underwent pathological evaluation. Complications were assessed according to Clavien-Dindo’s classification [30].
Postoperative continuous hormone therapy was recommended to patients with no pregnancy intention to reduce postoperative recurrences.
Figure 1 reports the postoperative follow-up. Referral to the appropriate MDT expert (colorectal, urologist, HPB surgeon, pain management, gastroenterologist, dietician, other) was made when clinically indicated.
STROBE statement for cohort studies was followed [31].
Pain questionnairesThe BSGE Pelvic Pain Questionnaire (Supplementary file 1) was completed in person at baseline (preoperatively) and through email at 6 months’ follow-up. Menstrual dyschezia was calculated from responses to question “pain opening bowels during period”, while non-cyclical dyschezia was calculated from responses to question “pain opening bowels at other times”. QoL scores were evaluated through Likert scale (Q7).
Statistical analysisPatient characteristics were summarized using basic descriptive statistics. Continuous variables were presented as median (interquartile range, IQR) and compared using Mann–Whitney U test. Categorical variables were expressed as proportions and analyzed using chi-squared or Fisher’s exact test. Statistical analysis was performed using IBM SPSS Statistics for Macintosh, version 28 (IBM Corp., Armonk, NY, USA). Confidence intervals were estimated at 95%, and significance level set at p = 0.05.
留言 (0)