
記住我
We collected data of 400 consecutive patients (age ≥ 18 yr) scheduled for major cardiac (n = 200; n = 100 with a cardiopulmonary bypass and n = 100 without a cardiopulmonary bypass) or vascular (n = 200) surgery between January 2019 and February 2020 at the University Hospital Frankfurt, retrospectively. Major surgery was defined as any cases with increased probability of an RBC transfusion.5,6 We manually extracted patient data and the number and types of performed laboratory tests from the hospital’s electronic database. Based on laboratory diagnostics, we identified the number of blood tests and the blood collection tubes used. We then used the data to quantify the amount of blood loss and to calculate the amount of reduced blood volume when using small-volume tubes. It is noteworthy to mention that small-volume tubes are used for the most part at the University Hospital Frankfurt. Standard-volume tubes are used for specific analyses or analyses performed at external laboratories. Briefly, use of small-volume tubes was part of the implementation of a Patient Blood Management program at the University Hospital Frankfurt.5 The exchange of the tubes was repeatedly announced to all employees by the head of the laboratory department through email, newsletters, and internal training. Small-volume sodium citrate coagulation [SCC] tubes were validated before implementation.3 Standard-volume tubes were replaced stepwise for each collection tube (serum, ethylenediaminetetraacetic acid [EDTA], SCC, and ABG) and for every hospital ward in close collaboration with medical staff. Handling and analyses of collected blood using small-volume tubes were closely controlled and analyzed.
The study protocol was approved by the ethics committee of the University Hospital Frankfurt (Ref. 318/17) and the requirement for written informed consent by patients was waived.
SamplingThe number of diagnostic samplings was evaluated for serum chemistry (serum), EDTA, SCC, ABG, blood culture (10.0 mL), thin capillary tubes (0.5 mL), point-of-care testing (POCT) (2.8 mL), and activated clotting time (ACT) (1.0 mL). The volume for standard and small-volume tubes were: 4.7 mL and 2.6 mL for serum, 2.7 mL and 1.8 mL for EDTA, 3.0 mL and 1.8 mL for SCC, and 2.0 mL and 1.0 mL for ABG, respectively. In addition, the placement of central venous catheter (CVCs) and arterial lines was noted.
Total blood loss for patients with ICU stays was calculated for both standard- and small-volume tubes based on the number of serum, EDTA, SCC, ABG, blood culture, thin capillary tubes, and POCT laboratory tests that were conducted. In the presence of a CVC or arterial line, 5 mL of blood was routinely discarded before blood was drawn for laboratory analysis and was included in the estimation of total blood loss. Closed blood conservation devices were used in the ICU only. In these patients, no blood was discarded during blood collection. Anemia was defined according to the World Health Organization criteria7 as Hb < 12.0 g·dL–1 for women and Hb < 13.0 g·dL–1 for men.
Statistical analysisTo investigate the volume of blood drawn for laboratory diagnostics, we estimated the number of blood tests taken and the number of collection tubes used. Based on laboratory profiles, the used collection tube was identified as 1) EDTA: small blood count including blood cells and Hb; 2) serum: creatinine, liver function, kidney function, and electrolyte; and 3) SCC: coagulation. Blood analyses performed with tubes for ABG were identified in the laboratory profiles. Next, the drawn blood volume was calculated using standard- and small-volume tubes for serum, EDTA, SCC, and ABG. Then, the total volume of blood drawn during a hospital stay was calculated for three conditions: 1) standard-volume tubes (serum [4.7 mL], EDTA [2.7 mL], SCC [3.0 mL], ABG [2.0 mL], blood culture [10.0 mL], thin capillary tubes [0.5 mL], POCT [2.8 mL], and amount of discarded blood [5.0 mL]); 2) small-volume tubes (serum [2.6 mL], EDTA [1.8 mL], SCC [1.8 mL], ABG [1.0 mL], blood culture [10 mL], thin capillary tubes [0.5 mL], POCT [2.8 mL], and amount of discarded blood [5.0 mL]); and 3) small-volume tubes and closed blood conservation devices (serum [2.6 mL], EDTA [1.8 mL], SCC [1.8 mL], ABG [1.0 mL], blood culture [10 mL], thin capillary tubes [0.5 mL], POCT [2.8 mL]).
We analyzed descriptive variables using means and standard deviations (SDs). Statistical significance was set at P < 0.05 and was determined using the Mann–Whitney U test, Student’s t test, or Fisher’s exact test. We used Spearman’s rank correlation rho to assess correlations between length of stay (LOS) and the number of laboratory tests performed. To assess the standardized mean difference, we calculated the absolute difference between saved blood volumes using small-volume tubes compared with standard-volume tubes. The number of performed laboratory tests with serum, EDTA, SCC, and ABG was used to calculate the saved blood volume. We performed a univariate linear regression model on the hospital stay and the volume of drawn blood volume for laboratory diagnostics. Prediction bands have been analyzed to take the variability of the data around the fitted curve into account. All analyses were conducted using R version 3.1 (R Foundation for Statistical Computing, Vienna, Austria) and Microsoft® Excel (Microsoft Corporation, Redmond, WA, USA).
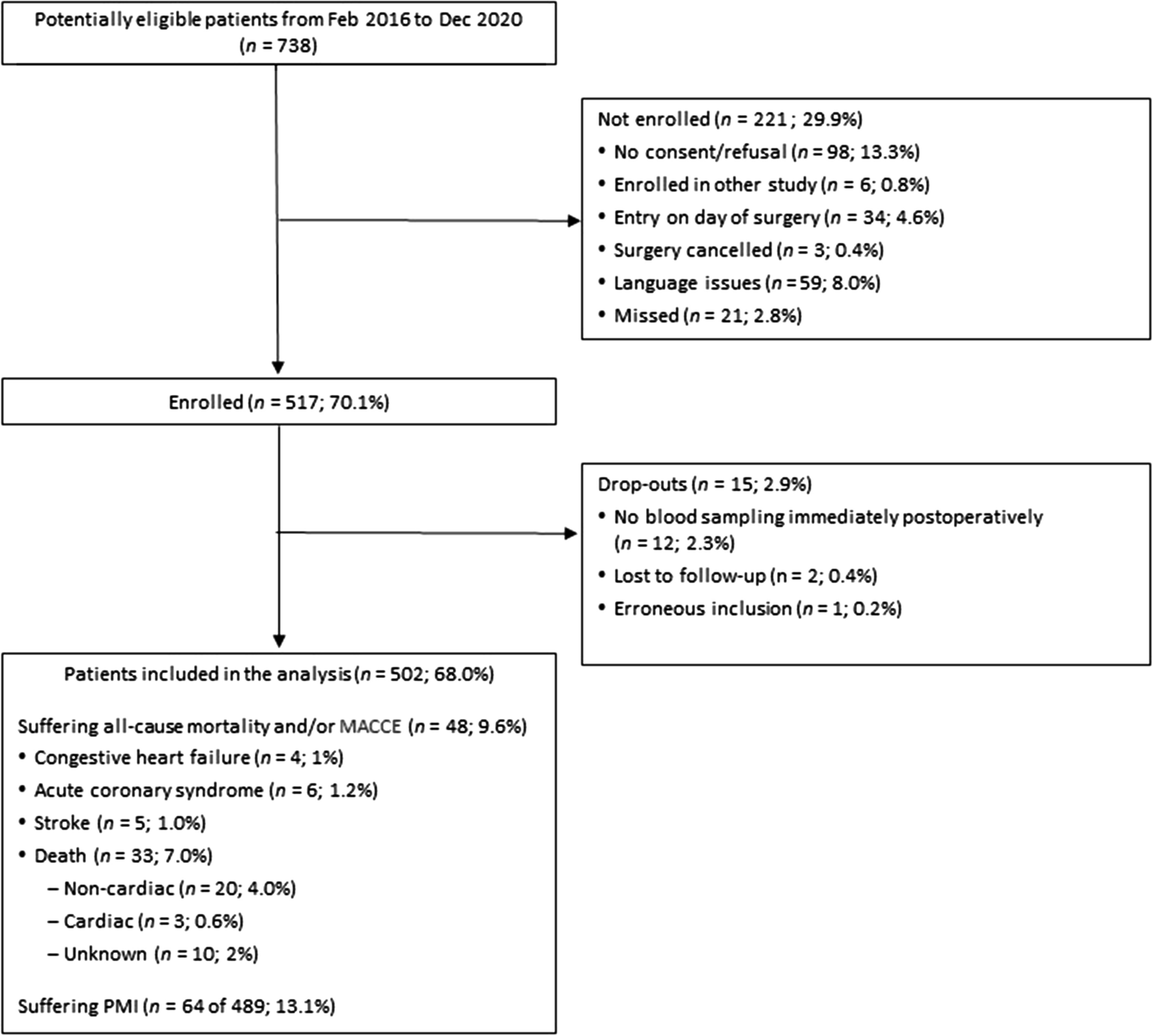
ResultsIn total, 200 patients undergoing cardiac surgery and 200 patients undergoing vascular surgery were included in the analysis (Electronic Supplementary Material [ESM] eTable 1). Table 1 lists the patient characteristics including age, sex, Hb level at admission, and presence or absence of anemia. The mean (SD) total hospital LOS was 14.7 (10.7) days for patients undergoing cardiac surgery and 16.3 (16.9) days for patients undergoing vascular surgery. For cardiac surgery patients, the mean (SD) Hb level at discharge was 10.3 (1.6) g·dL–1, and 93.5% of patients had anemia. For vascular surgery patients, the Hb level at discharge was 10.4 (2.0) g·dL–1 and 86.5% were anemic (Table 2). In total, 85 (42.5%) cardiac surgery patients had a LOS of 0–10 days, 80 (40%) had a LOS of 10–20 days, and 35 (17.5%) had a LOS of > 21 days. Of the vascular surgery patients, 116 (58%) had a LOS of 0–10 days, 31 (15.5%) had a LOS of 10–20 days, and 53 (25.6%) had a LOS of > 21 days. Electronic Supplementary Material eTables 2 and 3 show Hb levels and hospital LOS for patients undergoing peripheral major vascular surgery, aortic surgery, vascular surgery, and cardiac surgery with or without cardiopulmonary bypass.
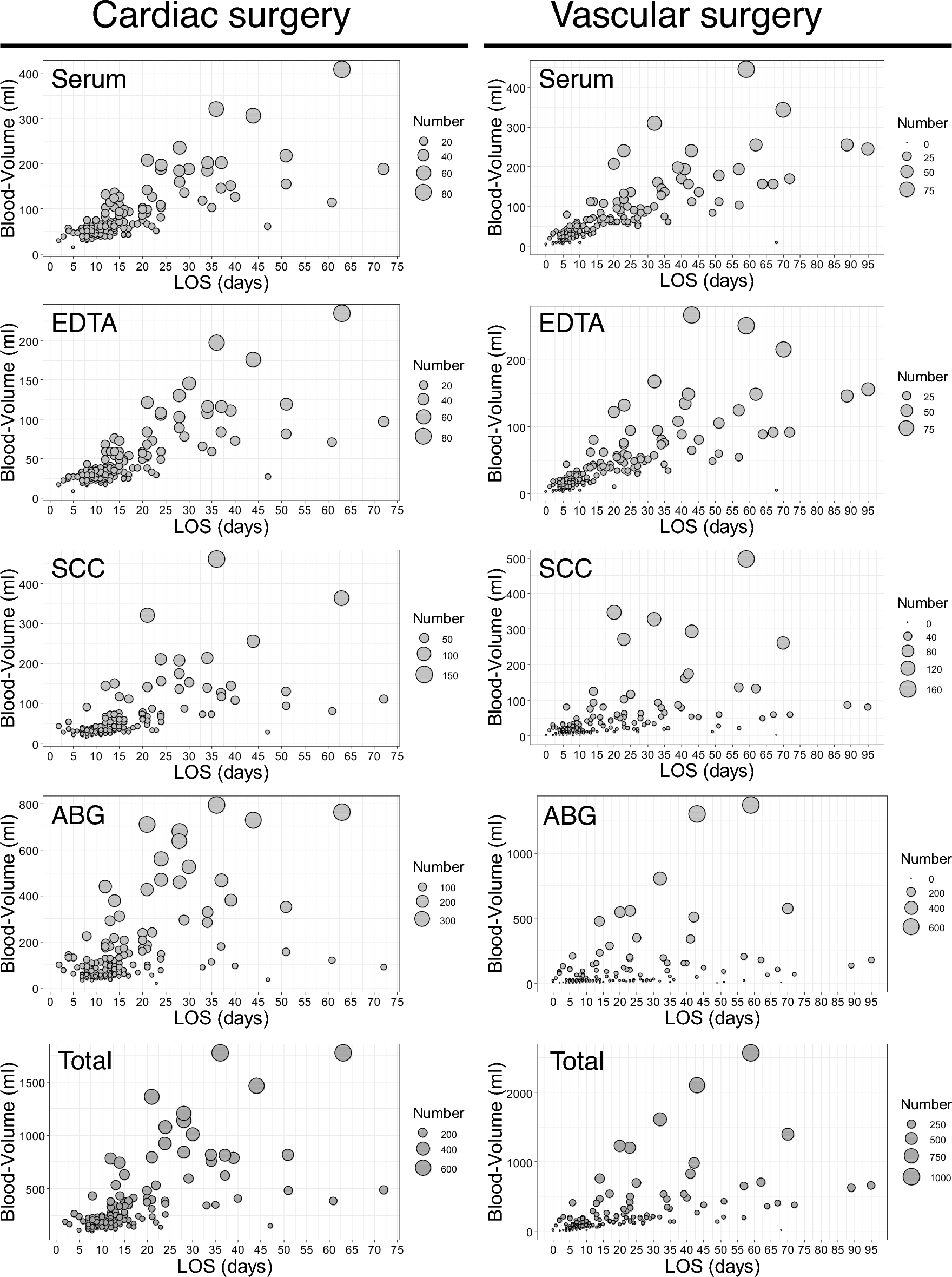
Table 1 Patient characteristicsTable 2 Length of hospital stay and hemoglobin level at dischargeBlood volumes and the frequency of laboratory testingThe most commonly performed laboratory tests in patients undergoing cardiac surgery were ABG (n = 12,678; 56%) followed by SCC (n = 3,606; 16%), serum (n = 3,151; 14%), and EDTA (n = 3,106; 14%). For patients undergoing vascular surgery, the most common tests were ABG (n = 7,177; 48%) followed by EDTA (n = 2,725; 18%), serum (n = 2,635; 17%), and SCC (n = 2,444; 16%) (ESM eTable 4). In cardiac surgery patients, hospital LOS and the number of laboratory tests using serum, EDTA, and SCC were strongly correlated (ESM eTable 5). Similarly, in patients undergoing vascular surgery, LOS and the number of laboratory tests using serum and EDTA were strongly correlated (ESM eTable 5). Increasing hospital LOS during the postoperative period was associated with increased overall phlebotomy volumes (Fig. 1). For patients undergoing cardiac surgery, the mean total blood loss due to phlebotomy was 167.9 mL (95% confidence interval [CI], 158.0 to 177.8), 255.6 mL (95% CI, 226.5 to 284.6) and 695.3 mL (95% CI, 544.1 to 846.4) with a hospital LOS of 0–10, 11–20, and > 21 days, respectively. The mean total blood loss due to phlebotomy was 80.5 mL (95% CI, 70.5 to 90.6), 225.0 mL (95% CI, 135.1 to 314.8) and 470.3 mL (95% CI, 333.5 to 607.1) for vascular surgery patients with a hospital LOS of 0–10, 11–20, and > 21 days, respectively (Fig. 2, ESM eFig. 1). The linear regression analysis revealed that LOS was a significant predictor for drawn blood volume using serum, EDTA, SCC, and ABG blood collection tubes. The analysis also showed that most of the analyzed data reside within the margins of the predictive bands (ESM eFig. 2).
Fig. 1
Number and volume of blood analysis per collection tube. The bubble plot shows for each collection tube the number and drawn blood volume per day. Bubble size represents the number of performed blood analyses.
ABG = arterial blood gas; EDTA = ethylenediaminetetraacetic acid; LOS = length of hospital stay; SCC = sodium citrate coagulation
Fig. 2
Total drawn blood volume during hospital stay. *P < 0.05. The number and volume of blood analyses are shown for patients undergoing cardiac or vascular surgery. Mean values with 95% confidence intervals are shown for hospital stays of 0–10 days, 11–20 days, and ≥ 21 days.
Amount of potential blood saving using small-volume tubesThe absolute difference between saved blood volumes using small-volume tubes compared with standard-volume tubes increased with a longer hospital LOS (ESM eTables 6 and 7).
The mean amount of blood drawn can be significantly reduced using small-volume tubes compared with standard-volume tubes both in cardiac and vascular surgery patients (ESM eTables 6 and 7): 50% reduction using ABG, 45% reduction using serum, 33.4% reduction using EDTA, and 40% reduction using SCC.
Total blood loss during the intensive care unit stayThe total blood loss was highest for patients during their ICU stay and increased the longer they spent in the ICU. Patients with a two-day stay in the ICU had a mean blood loss of 146.6 mL (95% CI, 134.6 to 158.6) and with ≥ 11 days, this increased to a mean blood loss of 1,428 mL (95% CI, 1,117.8 to 1,739.2) (Table 3). By using small-volume tubes, the amount of blood loss could have been reduced by 51.3 mL for patients with an ICU stay of two days and up to 465.3 mL for patients with an ICU stay of ≥ 11 days. The combined use of small-volume tubes and closed blood conservation devices was associated with a blood loss reduction of 82.8 mL for patients with an ICU stay of two days and 824.0 mL for patients with an ICU stay of ≥ 11 days (Fig. 3 and ESM eTable 8).
Fig. 3
Total drawn blood volume during intensive care stay. Mean values with 95% confidence intervals are shown for standard-volume tubes (standard VT), small-volume tubes (small VT) and small-volume tubes + blood conservation devices (small VT + BCD).
BCD = blood collection device; VT = volume tubes
留言 (0)