
記住我
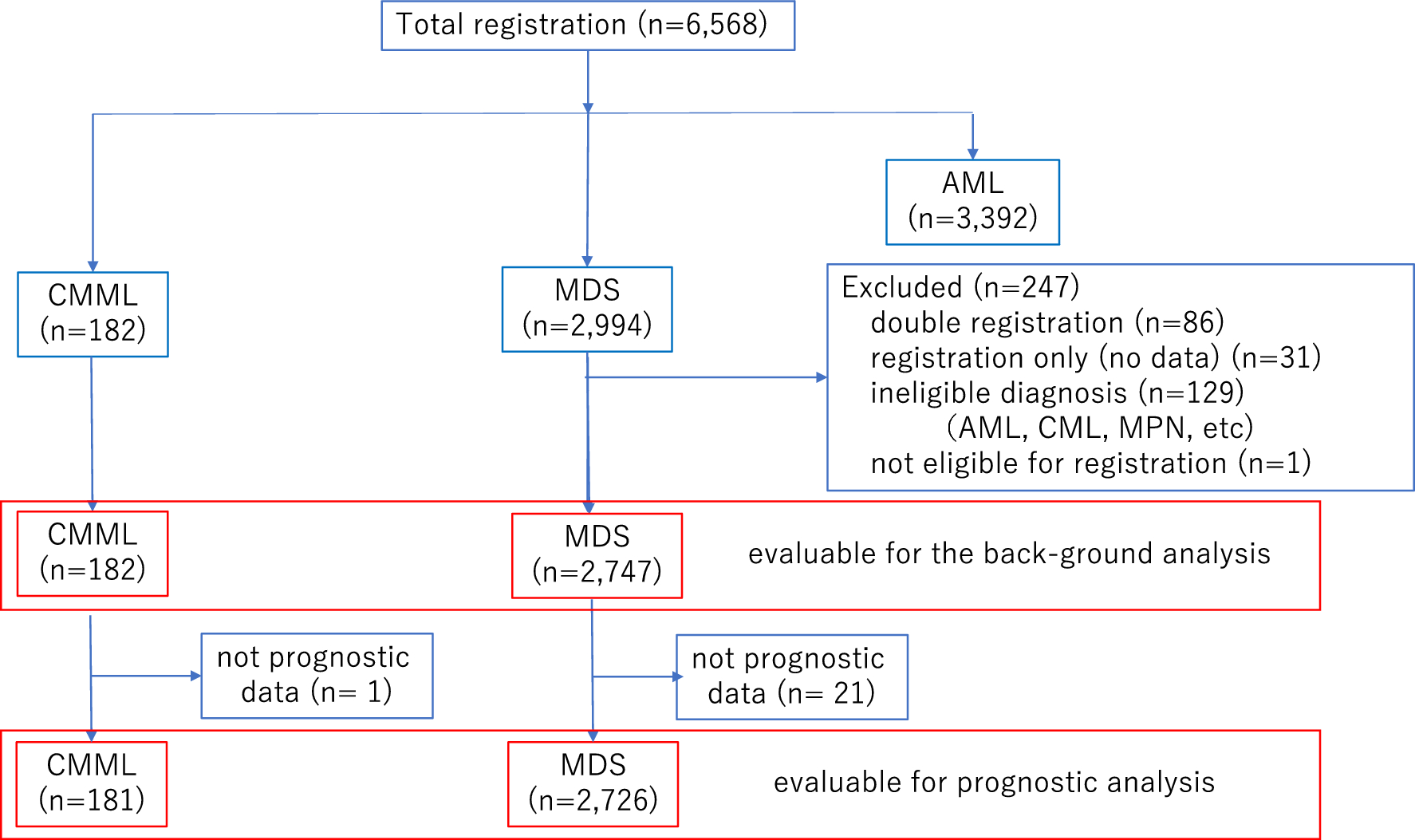
Data for 367 patients from 68 facilities were included in our analysis. Our subsequent survey revealed that 150 unenrolled patients had a confirmed prognosis of 2 months after the diagnosis of COVID-19. Among these patients, the number of reported HDs was 25. The capture rate for COVID-19 cases within the registration period was 71.0%.
The baseline patient characteristics and comorbidities are illustrated in Table 1. The median age at the time of COVID-19 diagnosis was 69 years (range 18–95 years); 215 patients (58.6%) were male, and 152 patients (41.4%) were female, one of whom was pregnant. Current or previous smokers comprised 34.3% of the patients, but no patients reported any experience with vaping (or no information was available). The number of patients who had been vaccinated against COVID-19 was 110 (30.0%). The diagnosis of COVID-19 was verified by PCR-based testing in 325 (88.6%) reported cases and by antigen testing in 54 (14.7%) reported cases. Most cases of SARS-CoV-2 infection were community-acquired (n = 227; 61.9%) or nosocomial (n = 88; 23.9%); the infection route in the remaining patients was unclear. A total of 106 patients (28.9%) reported more than one comorbidity, among which hypertension was most frequent (28.9%) and was followed by diabetes (19.4%). Twenty-four patients (6.5%) participated in other registries, all of whom were enrolled in COVIREGI-JP. Details of laboratory and imaging tests at the time of COVID-19 diagnosis are described in Supplemental Table S1. The most prevalent finding on chest X-ray or CT images of the lungs was ground-glass opacity or ground-glass attenuation (81.9%), and unilateral and bilateral findings were observed in 14.5% and 85.5% of cases, respectively.
Table 1 Patient characteristics and comorbiditiesBackground HDs and treatmentThe HDs at the time of COVID-19 diagnosis included seven benign (n = 43; 11.7%) and 25 malignant diseases (n = 324; 88.3%; Table 2). The median time between HD and COVID-19 diagnoses was 710 days (benign disease 1,046 days; malignant disease 670 days). The most common benign HD was immune thrombocytopenia (ITP), which accounted for 5.5% (n = 20) of the total population. The most common malignant HD was aggressive B-cell lymphoma, which was followed by multiple myeloma and myelodysplastic syndromes. Malignant lymphoma, including aggressive B-cell lymphoma, affected 145 people, accounting for approximately 40% of the entire population. The composition of each HD and the details of the treatments for each disease in the last year before the COVID-19 diagnosis and at the time of the COVID-19 diagnosis are shown in Supplemental Fig. S1 and Table S2 (1)–(33). Allogeneic and autologous transplantation were conducted in 36 (9.8%) and 16 (4.4%) patients, respectively, and none of the patients were treated with CAR-T (CD19 CAR-T). Table 3 provides information on HD status at the time of COVID-19 diagnosis, and the time between final treatment and diagnosis. At the time of COVID-19 diagnosis, 14.7% of patients were in initial diagnosis/on induction therapy; 18.8% were in remission on consolidation or maintenance therapy; 24.8% were in remission and not on therapy; 20.4% had stable disease but were not in remission; and 16.4% had a status of relapsed and refractory. Regarding the time from the last treatment for HDs to COVID-19 diagnosis, most patients (n = 211; 57.5%) were currently undergoing treatment; times within 3 months, within 3–6 months, within 6 months to 1 year, and within 1–2 years accounted for less than 10% each, and times after 2 years accounted for 14.7%.
Table 2 Background hematological diseases and history of cellular therapiesTable 3 Hematologic disease status at the time of diagnosis of COVID-19 and time since treatment for hematologic diseasePresenting symptoms and severity at the time of COVID-19 diagnosisWe examined the presenting symptoms of patients with COVID-19 (Table 4). The most prevalent presenting symptoms were fever (85.0%), cough (50.6%), shortness of breath (31.0%), and fatigue (29.4%). We also examined the severity COVID-19 diagnosis according to the ASH [4] and Ministry of Health, Labour and Welfare (MHLW) [15] criteria. According to the ASH criteria, 127 (34.6%), 220 (60.0%), and 20 (5.4%) patients had mild, moderate, and severe disease, respectively. According to the MHLW criteria, 182 (49.6%), 87 (23.7%), 80 (21.8%), and 18 (4.9%) were classified as having mild, moderate-I, moderate-II, and severe disease, respectively.
Table 4 Symptoms and severity at the time of COVID-19 diagnosisTreatment and supportive care for COVID-19COVID-19-specific therapies for all patients are shown in Supplemental Table S3. The most common COVID-19-specific medications were remdesivir (40.3%) and dexamethasone including alternate glucocorticoids (37.3%), followed by favipiravir (15.5%) and tocilizumab (6.3%). However, approximately 20% of all patients received no treatment or observation.
We also explored the use of supportive care for COVID-19. Approximately 60% of patients did not receive oxygen at the time of COVID-19 diagnosis, and approximately 40% of patients required low-flow oxygen (1–5 L). Less than 10% of patients required invasive mechanical ventilation, and only 3% required ECMO. Approximately one-quarter (24.3%) of patients were given anticoagulant medication at the time of COVID-19 diagnosis, most commonly unfractionated heparin (n = 53; 14.4%).
Laboratory data predicting OSBoxplots of the laboratory test results at the time of COVID-19 diagnosis are shown in Supplemental Fig. S2, stratified by survival status in all patients. Laboratory indicators at the time of COVID-19 diagnosis, including hemoglobin, albumin, lactate dehydrogenase, and C-reactive protein (CRP), showed substantial differences between the patients who survived and those who died. We then used ROC curve analysis to assess the abilities of these four factors to predict OS outcomes (Fig. 1). Albumin and CRP had a relatively high predictive value compared to other factors for all patients (threshold 3.3, AUC 0.743, 95% CI 0.660–0.825; threshold 6.96, AUC 0.722, 95% CI 0.645–0.800).
Fig. 1
Receiver operating characteristic curve analysis of laboratory data at the time of COVID-19 diagnosis for overall survival in all patients. ROC receiver operating characteristic, AUC area under the curve, Hb hemoglobin, LDH lactate dehydrogenase, Alb albumin, CRP C-reactive protein
Outcomes of SARS-CoV-2 infectionThe median follow-up duration for the survivors was 73 days (range 1–639). At the data cutoff, 49 (13.3%) patients had died. Among the entire patient population, the 60-day OS rate was 86.6% (95% CI 82.6–89.7%), and the median OS was not reached (Fig. 2a). In the ASH classification, the 60-day OS rates were 92.1% (95% CI 85.9–95.7%), 85.4% (95% CI 79.9–89.4%), and 65.0% (95% CI 40.3–81.5%) for the mild, moderate, and severe groups, respectively (Fig. 2b). For the MHLW classification, the 60-day OS rates were 92.8% (95% CI 88.0–95.8%), 86.2% (95% CI 76.9–91.9%), 78.8% (95% CI 68.1–86.2%), and 61.1% (95% CI 35.3–79.2%) for the mild, moderate-I, moderate-II, and severe groups, respectively (Fig. 2c). Furthermore, univariate analysis indicated that several factors were associated with OS, including age > 60, Alb ≤ 3.3 g/dl, severity according to ASH classification, severity according to MHLW classification, benign disease, PS > 2, relapsed/refractory status, oxygen requirement at diagnosis, and CRP > 7.0 mg/dl (P = 0.006, P < 0.001, P = 0.003, P < 0.001, P = 0.028, P < 0.001, P < 0.001, P < 0.001, and P < 0.001, respectively; Table 5). In the multivariate analysis considering these variables, Alb ≤ 3.3 g/dl (hazard ratio (HR) 4.026, 95% CI 1.954–8.294, P < 0.001) and requiring oxygen (HR 14.55, 95% CI 3.378–62.64, P < 0.001) were independently associated with shorter OS, whereas benign disease (HR 0.095, 95% CI 0.012–0.750, P = 0.026) was associated with longer OS. The multivariate analysis in the patients with malignant HDs, excluding benign HDs, also indicated that Alb ≤ 3.3 g/dl (hazard ratio (HR) 4.165, 95% CI 2.002–8.666, P < 0.001) and requiring oxygen (HR 14.72, 95% CI 3.421–63.33, P < 0.001) were independently associated with shorter OS (Supplemental Table S4). The presence of HDs, such as lymphoma, was not in itself a significant factor associated with OS in either cohort.
Fig. 2

Kaplan–Meier estimates of overall survival. Kaplan–Meier estimates of overall survival for a all patients and with stratification by b ASH severity, c JMHW severity, d albumin at diagnosis, e oxygen required, f benign or malignant hematological diseases, g vaccination status, and h route of infection. ASH The American Society of Hematology, MHLW The Ministry of Health, Labour and Welfare in Japan
Table 5 Univariate and multivariate analyses of 60-day OSThe 60-day OS rates for patients with Alb ≤ 3.3 g/dl and oxygen required (65.6%; 95% CI 55.0–74.3% and 70.6%; 95% CI 62.8–77.1%) were inferior to those of other patients (92.6%; 95% CI 87.8–95.5%; P < 0.001 and 98.6%; 95% CI 95.6–99.5%; P < 0.001) (Fig. 2d, e). In contrast, patients with benign disease had a longer OS than patients with malignant disease (60-day OS; 97.6%; 95% CI 84.3–99.7% vs. 85.1%; 95% CI 80.8–88.6%, P = 0.028; Fig. 2f). We also compared OS between vaccinated and non-vaccinated patients, as well as between patients with community-acquired and nosocomial infections. As expected, the OS was longer in vaccinated patients and those with community-acquired infection than in the other patients (60-day OS; 95.4% vs. 82.8%, P = 0.001 and 92.9% vs. 68.1%, P < 0.001, respectively; Fig. 2g, h). The 60-day OS rates for patients diagnosed during the first to sixth waves of COVID-19 were as follows: 38.9% (95% CI 17.5–60.0%; n = 18), 73.1% (95% CI 51.7–86.2%; n = 26), 86.7% (95% CI 77.3–92.4%; N = 83), 81.8% (95% CI 68.8–89.8%; n = 55), 95.7% (84.0–98.9; n = 47), and 94.1% (95% CI 88.6–97.0%; n = 138), respectively. Notably, the OS rates varied across the different epidemic waves, and higher mortality was observed during the early waves (details in Supplemental Fig. S3).
Outcomes of complications during hospitalizationWe also investigated several complications (thrombosis, hemorrhage, and new infections) associated with COVID-19 during hospitalization. The most common complications were additional infections, which occurred in 48 of 367 patients (13.1%), which were followed by thrombosis and bleeding (four and seven patients, respectively). The proportion of non-survivors was higher (35.4%) among patients who developed new infections during their hospital stays than among those who contracted new thrombosis (25.0%; 1/4) or hemorrhage (28.6%; 2/7; Supplemental Fig. S4a–c). Among all patients, the mortality rate was higher among patients with than without new infections (35.4% vs. 10.0%; P < 0.001).
留言 (0)