Ureteropelvic junction obstruction (UPJO) is one of the most common obstructive malformations in pediatric urology [5]. The incidence of this condition ranges from 1 per 500 births [2]. This pathology is most commonly observed in boys (60–75%). According to the literature, the left side is the most frequently affected (60%). It can also be bilateral in 10–20% of cases [8,9,10]. These data are consistent with our results.
Antenatal diagnosis has been made in over 50% of cases [9, 10]. In our study, antenatal diagnosis was made in 15 out of 40 patients (37.5%) in group A and 8 out of 25 in group B. This percentage difference can be explained by several factors. First, the small sample size of our study may have contributed to the variation. In addition, inadequate prenatal care in developing countries, the operator-dependent nature of ultrasound scans, and low socio-economic level, can all hinder the thorough monitoring of pregnancies.
The management of patients with UPJO has evolved considerably over the past few decades [11, 12]. Laparoscopy is one of the preferred methods for managing many urological diseases. While open surgical procedures are still considered the gold standard, they are being replaced by techniques that offer equivalent success rates, reduced post-operative pain, and shorter hospital stays [13].
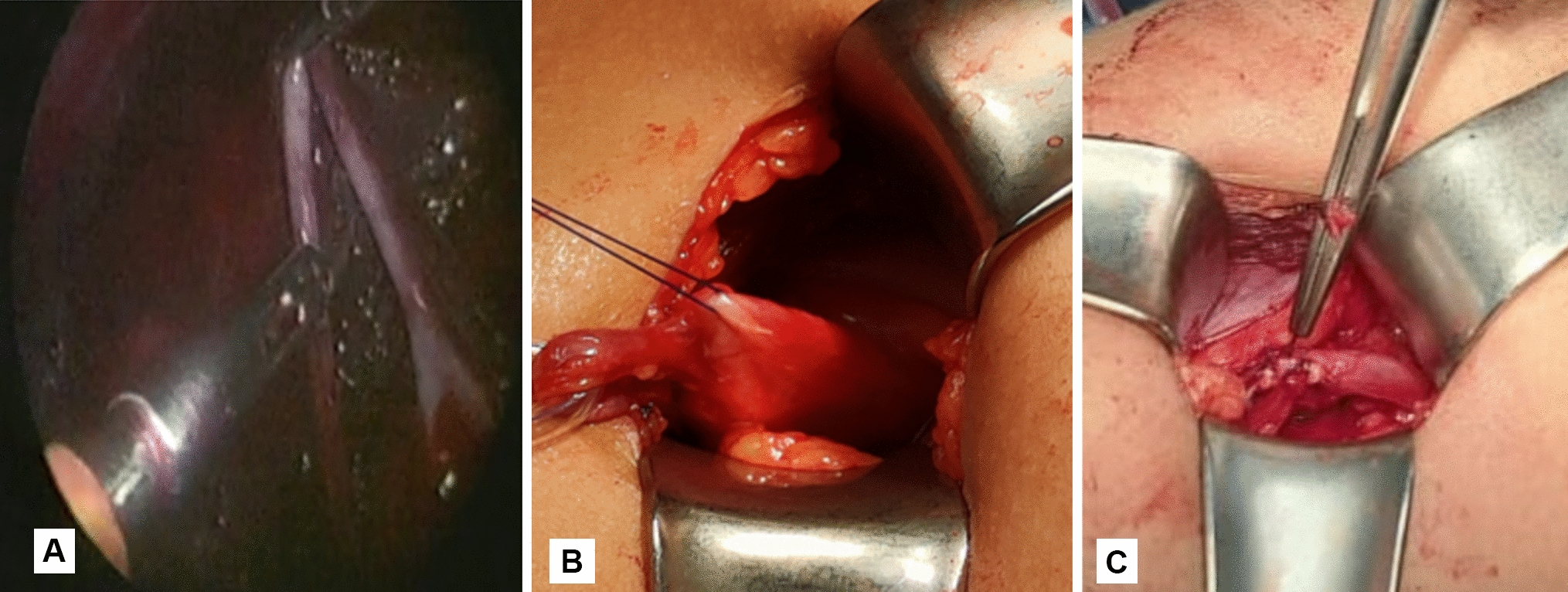
Laparoscopic pyeloplasty in children is still controversial due to the challenges of intracorporeal suturing and the limited space within the intraperitoneal cavity. This procedure is difficult to learn and time-consuming [14]. After an initial experience, it was suggested that the laparoscopic approach should not be performed in children younger than 6 months of age, while in our study, laparoscopic procedures have been performed on patients who were more than 3 months. Consequently, the patients who undergo laparoscopic procedures tend to be older than open [15]. Moreover, handling fine suture materials with current laparoscopic instruments remains cumbersome. As originally described by Lee et al. [16], exteriorizing the anastomosis in laparoscopic assisted dismembered pyeloplasty (LADP) overcomes these challenges. The technique is similar to the exteriorization of the loop of the intestine used in gastrointestinal anastomosis [17]. LADP provided less mobilization that has been required to bring the UPJ out of the flank. The duration of the surgery was much shorter than that of a contemporary series of pediatric laparoscopic pyeloplasty. As this procedure does not involve intracorporeal suturing, the learning curve is much shorter compared to that of a complete laparoscopic pyeloplasty [18, 19].
Helal and Daboos [20] utilized laparoscopic assisted pyeloplasty in approximately 20 out of 40 patients. They concluded that this minimally invasive method had a shorter operative time and less post-operative pain. However, the functional results showed no significant difference when compared to the open method. In our study, we adopted the same approach in group A, as the previous researchers and found that this method eliminates the requirement for a large lumbar incision. The mean operative time in the group of LADP was shorter; in our study, it was 90 ± 12 min, while Helal and Daboos [20] series had a longer operative time and it was 120 min. Therefore, we adapted the technique of laparoscopic assisted pyeloplasty in cases of group A because of the benefits of a minimally invasive approach, in addition to easy, safe exploration fewer wound complications, and short hospital stay.
Numerous studies have focused on impaired renal function to establish an algorithm for its evaluation and treatment [2, 7, 21]. However, the management of poorly functioning kidneys, which are associated with less than 10% of UPJO cases, is still debatable [2, 21]. Defining whether these patients would benefit from pyeloplasty and avoid undergoing total nephrectomy. We have reviewed the series in which the authors have defined, in their results, the group of patients considered to have UPJO with impaired renal function. In their series of 142 renal units, Hashim [22] considered renal function to be impaired if it was less than 20%. Bowen [23], Nayyar [24], Nishi [25], Dhillon [26], and Salem [27] also utilized this criterion. UPJO with severely impaired renal function was reported in studies by Lone [28], Ulman [29], and Csaicsich [30]. In their series, the renal function value was found to be less than 15%. Similarly, Abdelaziz [31], Gupta [2], Aziz [7], Bassiouny [32], and Wagner [33] reported a renal function value of less than 10% in their series.
In our series, a cutoff value of 10% was used to define UPJO with impaired function in scintigraphy. Previously therapeutic options included conservative treatment (pyeloplasty), nephrostomy followed by pyeloplasty, and radical treatment (nephrectomy) [28, 32]. However, recent studies with long-term follow-up have shown an improvement in renal function after pyeloplasty in these cases. Thus, nephrectomy is no longer justified [31, 34].
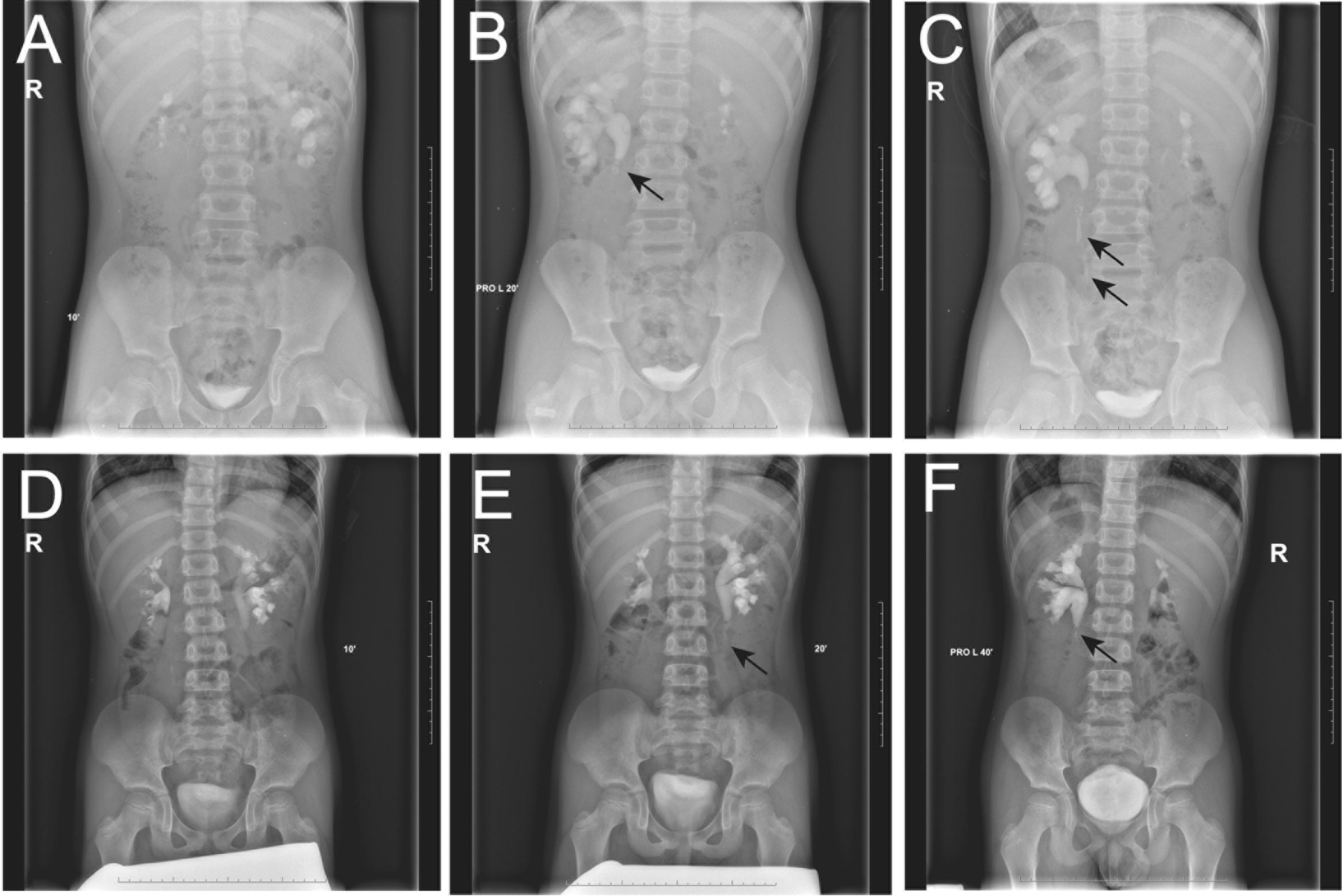
The diameter of the renal pelvis was reduced in all cases in the current study. Specifically, the mean antero-posterior (AP) diameter decreased from 38 ± 7.2 mm and 40 ± 7.2 mm in both groups to 16 ± 3.1 mm and 14 ± 2.1 mm post-operatively. Regarding renal function, our results showed improvement with a mean increase from 7.9 ± 1.3% and 8.1 ± 1.1% pre-operatively to 22.22 ± 6.3% and 24.20 ± 5.1% post-operatively. Other studies have shown an improvement in RF following pyeloplasty. Wagner [33] conducted a study on the outcomes of pyeloplasty in 32 patients who were divided into 3 groups: group I (RF > 40%), group II (10% < RF < 40%), and group III (RF < 10%). A significant improvement in RF was observed in patients who underwent pyeloplasty 12 months after the procedure. Specifically, patients with an initial RF level < 10% experienced a mean post-operative RF of 36%. Abdelaziz [31] conducted a prospective study on 25 patients with UPJO and a split renal function (SRF) of less than 10% who underwent pyeloplasty. The study observed an improvement in FR, with an average increase from 5% pre-operatively to 21% post-operatively after 6 months of surgery, and 20% after 12 months (Table 6).
Table 6 The various studies have emphasized the impact of pyeloplasty on a kidney with UPJO and renal function ≤ 10%Although our work provides an answer to the choice of surgical treatment for renal units with UPJO and impaired renal function ≤ 10% of overall function, it is primarily limited by the short follow-up period. This limitation can affect the perception of late complications and the necessity of nephrectomy after a prolonged period of progression.


留言 (0)