CRYAB encodes the alpha-crystallin B chain that belongs to a small heat-shock protein that contributes to the structural integrity of the protein and cellular structures, preventing aberrant protein aggregation [12]. Since this protein is mainly expressed in the tissues of the eye lens, cardiac, or skeletal muscles [13], mutant in CRYAB may cause clinical symptoms in these organs. Disorders associated with CRYAB variants are difficult to diagnose accurately due to the divergent phenotypes, but missense type variants and the isolated cataract phenotype are most commonly reported. On the other hand, patients with CRYAB truncating variants showed more severe manifestations including infantile onset myopathy and ventilator insufficiency [14,15,16,17]. We show that a stop-loss variant, a gain-of-function mutation, can reduce protein stability and lead to syndromic clinical presentation, such as adult-onset DCM with congenital cataracts as reported in the current study. This corresponds with a previous case reported by van der Smagt et al., involving a stop-loss variant that also had a complex phenotype [10]. The affected family members in that study presented with a combination of congenital cataracts and the adult-onset DCM without skeletal myopathy, and their cardiomyocytes showed protein aggregation on immunohistochemical staining [10]. Other reports of CRYAB-related cardiomyopathy showed heterogeneity in mutant type (missense, frameshift, stop-loss etc.) and clinical manifestations (cardiomyopathy with or without syndromic features), making generalization difficult.
To date, only two stop-loss variants in CRYAB were reported; c.527A>G [p.(Ter176TrpextTer19)] detected in the current study and c.528G>T [p.(Ter176TyrextTer19)] in another study [11]. Both mutants were predicted to have new alpha-helixes and random coils (Fig. 2A) and increased instability and hydrophobicity (Fig. 2B). However, it is of note that there would be a possibility of genotype-phenotype correlation in the two stop-loss variants. The c.527A>G case found in the current study showed syndromic features of ocular and cardiac problems, whereas the previously reported c.528G>T case showed no other systemic abnormalities except congenital cataract [11]. The phenotypic differences might be related to differences in hydrophobicity between tryptophan (Trp) and tyrosine (Tyr) at the 176th codon, which is the first amino acid residue of the extended strand resulting from each variant. The GRAVY score of -0.509 in c.527A>G was higher than -0.511 in c.528G>T, and in particular, the difference between the hydrophobicity score of −0.222 and -0.178 at the 176th codon of each variant was even larger. Additionally, differences in oxidation between Trp and Tyr residues could be another explanation. It is well known that these two residues are vulnerable to protein oxidation caused by endogenous and exogenous stimuli, leading to several diseases such as cancers, cardiovascular diseases, and asthma [18, 19]. Previous experimental study showed that Trp residue is more readily oxidized than Tyr [19], suggesting that c.527A>G may cause a more complex phenotype than c.528G>T.
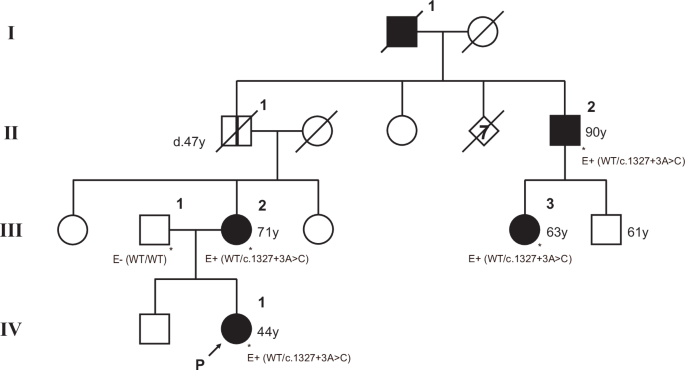
It is extremely rare for CRYAB variants to be detected as the cause of DCM. A prior report of 766 patients with DCM from various ethnic origins reported that none of the subjects had pathogenic, likely pathogenic, or uncertain significant variants in CRYAB [8]. Moreover, since most DCM develops in adulthood, it can be difficult to diagnose based on the history of the patient and the current medical complaints. The cardiomyopathies involve families in a Mendelian pattern and usually affect younger patients, highlighting the importance of cardiomyopathy as an important cause of heart failure and sudden cardiac death in young individuals who may be asymptomatic [5, 6, 20]. The proband in our study had a 10-year-old son (III:1, Fig. 1A) who had the same CRYAB variant. He was diagnosed congenital cataract at his age of 4, but has not diagnosed with or suffered from DCM. Early diagnosis and risk recognition of DCM are very important as clinical implications and outcomes may vary depending on the identified causative gene and variant, so genetic counseling and prevention and management of future high-risk diseases are necessary for the proband’s young child.
In conclusion, our study expands the genotype of CRYAB-related disease and illustrates the emerging complex phenotype. It also highlights the importance of comprehensive molecular workup such as WGS for syndromic DCM accompanied by cataracts, considering the possibility that it is a CRYAB-related disease.



Comments (0)