
記住我


Between 11 February 2020 and 2 January 2023, 65 patients were screened, of which 59 were enrolled. Of those, two did not receive study medication owing to death (one patient) and withdrawal of consent (one patient) and nine discontinued study treatment within the first two cycles owing to primary progressive disease (three patients), death (one patient), adverse events (four patients) and non-compliance (one patient). According to the study protocol, 48 patients who received at least two cycles of study treatment, including at least one administered dose in cycle three, comprised the analysis population (Fig. 1). The primary end point was ORR at interim staging and the secondary end points included ORR after consolidation therapy, duration of response (DOR), progression-free survival (PFS), overall survival, time to next treatment (TTNT) and safety. Post hoc analyses included ORR and time-to-event parameters in the intention-to-treat (ITT) population, ORR and PFS according to previous RT-directed therapy and according to previous BTK inhibitor exposure.
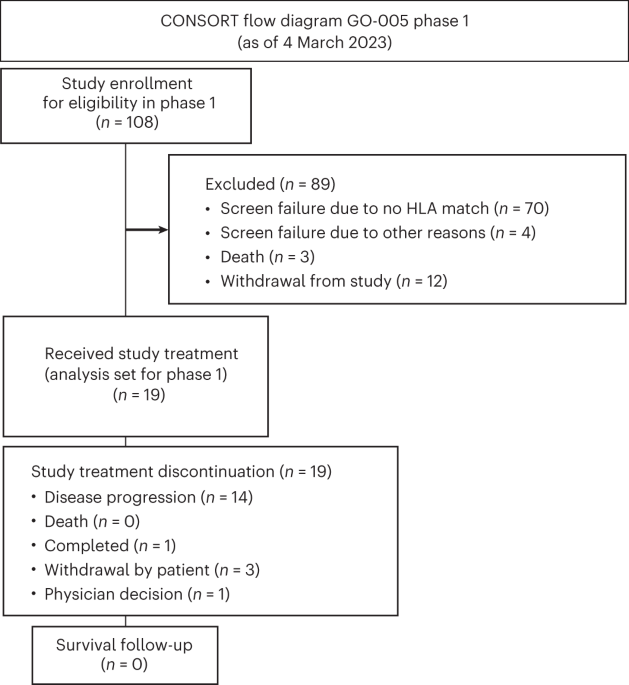
Fig. 1
CONSORT diagram of RT1. PD, progressive disease; AE, adverse event.
The median age was 67 (range 45–82) years, 29 (60.4%) patients were male and 19 (39.6%) were female (Table 1). Twenty-two (45.8%) patients had Eastern Cooperative Oncology Group (ECOG) performance status of 1 or higher and the median cumulative illness rating scale (CIRS) score was 4 (range 0–17). The median LDH at enrollment was 335 U l−1. Sixteen (34.8%) patients had del(17p)/TP53mut, whereas 29 (70.7%) patients had unmutated IGHV. Overall, 25 (64.1%) patients had high or very high-risk CLL according to the chronic lymphocytic leukemia international prognostic index (CLL-IPI), 11 (28.2%) had intermediate risk and 3 (7.7%) had low risk. Complex karyotype (≥3 aberrations) was detected in 16 (42.1%) patients. A total of 46 (95.8%) patients had DLBCL-RT and 2 (4.2%) patients had HL-RT. In those 26 patients (54.2%) in whom clonal relatedness was evaluated by immunoglobulin heavy chain rearrangement analysis, all cases were reported as clonally related to the CLL (22 (45.8%) were unknown). The DLBCL subtype was evaluated in 15 patients with RT; 14 had a non-germinal center B cell (GCB) type and 1 had a GCB type. The median Ki-67 index was 70% (interquartile range (IQR) 50–80%). Overall, 36 (75.0%) patients had received previous CLL-directed therapy, including chemoimmunotherapy (CIT; 25 patients) and targeted agents (32 patients) as well as previous allogeneic stem cell transplant (SCT) in 3 patients. Of those patients with previous targeted treatment, 24 had received previous BTK inhibitor treatment, 22 patients had previous treatment with BCL-2 inhibitors and 2 patients had received previous combined BTK + BCL-2 inhibitor therapy (Table 1). Twelve (25.0%) patients had treatment-naive CLL. Ten patients (20.8%) had received previous RT-directed therapy, including R-CHOP-like regimens and one case of previous ibrutinib treatment. A total of 38 (79.2%) patients had not received previous RT-directed therapy (Table 1).
Table 1 Baseline patient characteristicsWith a data cutoff of 2 May 2023, 19 patients were still under ongoing treatment (Fig. 2). Overall median observation time was 13.9 months (IQR 8.7–22.2) and median observation time for patients still alive was 12.0 months (IQR 8.4–22.1). The median number of treatment cycles of tislelizumab was 9 (IQR 4–23) and of zanubrutinib 11 (IQR 5–25).
Fig. 2: Response rates and duration of treatment.
Swimmer plot depicts disease assessments and treatment phase and duration. Bar chart indicates response rates. CR, complete response; PR, partial response; SD, stable disease.
Efficacy end pointsTwenty-eight of 48 patients responded to induction therapy resulting in an ORR of 58.3% (95% CI 43.2–72.4), including 9 (18.8%) complete response and 19 (39.6%) partial response, meeting the study’s primary end point (P = 0.008) by rejecting the predefined null hypothesis of 40% (Fig. 1). Stable disease was reported in 6 (12.5%) patients and 14 (29.2%) patients had progressive disease. The ORR as assessed according to the refined Lugano criteria agreed with the ORR according to iwCLL criteria. The median DOR was not reached; the 6-month DOR rate was 70.6% (95% CI 51.0–90.2; Fig. 3a). The median PFS was 10 months (95% CI 3.8–16.3) with a 12-month rate of 46.9% (95% CI 29.4–64.5; Fig. 3b). The median overall survival was not reached (12-month overall survival rate 74.7%, 95% CI 58.4–91.0) (Fig. 3c). All deaths were associated with disease progression. The median TTNT, defined as time to initiation of a next line of treatment with censoring of deaths, was 17.9 months (12-month TTNT rate 58.5%, 95% CI 40.7–76.4)) and 12.5 months (12-month TTNT rate 50.2%, 95% CI 32.2–68.1) when defined as time to initiation of a next line of treatment or death, whatever occurred first (Fig. 3d and Extended Data Fig. 1). Three of 48 patients have not reached the end of consolidation after 12 cycles so far. The ORR in the remaining 45 patients was 46.7% (95% CI 31.7–62.1) with a complete response in 10 patients (22.2%), partial response in 11 patients (24.4%), stable disease in 3 patients (6.7%), progressive disease in 3 patients (6.7%) and missing data in 18 patients (40.0%, including 16 patients with discontinuation of therapy before reaching the end of consolidation).
Fig. 3: Kaplan–Meier analyses for secondary efficacy end points.
a, DOR. b, PFS. c, Overall survival (OS). d, TTNT.
Post-protocol treatment included chemoimmunotherapy in 21 cases (50.0%), BTK/BCL-2 inhibition in 7 (16.7%) cases and 8 (19.0%) allogeneic SCT (Extended Data Table 1). SCT was conducted as consolidation in two patients with partial response and as salvage treatment for five patients with stable disease or progressive disease (one missing response) (Fig. 2).
None of the assessed baseline clinical, serological or genomic features was significantly associated with response or non-response (Extended Data Table 2). In a univariate analysis, factors significantly associated with shorter PFS were the presence of severe constitutional symptoms, ECOG > 0, LDH, thymidine kinase and serum β2-microglobulin (>3.5 mg l−1). Shorter overall survival was associated with Binet C, age, severe constitutional symptoms, LDH, thymidine kinase and serum β2-microglobulin (>3.5 mg l−1). Shorter DOR was associated with presence of Binet C, LDH, TP53 deletion and/or mutation, thymidine kinase and serum β2-microglobulin (Extended Data Tables 3–5).
The ORR in patients without previous RT-directed therapy was 57.9% (95% CI 40.8–73.7) and 60.0% (95% CI 26.2–87.8) in patients with previous RT-directed therapy. Patients without previous RT-directed therapy had a 12-month PFS rate of 43.5% (95% CI 23.2–63.9) and patients with previous RT-directed therapy had a 12-month PFS rate of 60.0% (95% CI 19.9–100.0) (Extended Data Fig. 2a).
Patients without previous exposure to BTK inhibitors had an ORR of 69.6% (95% CI 47.1–86.8) and patients with previous BTK inhibitor therapy had an ORR of 48.0% (95% CI 27.8–68.7). The 12-month PFS rate in patients without previous BTK inhibitor therapy was 58.3% (95% CI 33.2–83.4) and 37.2% (95% CI 12.8–61.6) in patients with previous BTK inhibitor therapy (Extended Data Fig. 2b).
A post hoc analysis of all 59 eligible patients, including those not receiving study treatment for at least two cycles (ITT population), demonstrated an ORR of 47.5% (95% CI 34.3–60.9); both patients with HL responded with a partial response. The median PFS of all eligible patients was 6.7 months (95% CI 2.3–11.0) with a 12-month rate of 39.5% (95% CI 23.8–55.3), median overall survival was not reached (12-month overall survival rate 65.7%, 95% CI 49.3–82.0) and median TTNT was 17.9 months (12-month TTNT rate 55.4%, 95% CI 38.0–72.7) (Extended Data Fig. 3 and Extended Data Table 6).
Safety end pointsFor the safety analysis, all 57 included patients who had received at least one dose of any study medication were considered. A total of 56 (98.2%) patients experienced at least one grade ≥1 adverse event during the observation period. The most common adverse events of any grade occurring during the observation period were gastrointestinal disorders (56.1%), including diarrhea (28.1%) and nausea (17.5%), general disorders (52.6%), including pyrexia (19.3%), peripheral edema (17.5%), edema (8.8%) and fatigue (8.8%), blood and lymphatic system disorders (47.4%), including anemia (19.3%), neutropenia (21.1%) and thrombocytopenia (19.3%) and infections and infestations (78.9%), including COVID-19 (22.8%) and urinary tract infections (21.1%).
Cardiac toxicities, of interest in the context of BTK inhibitors, were uncommon, with one case each of angina pectoris (grade 3), cardiac failure (grade 2), cardiovascular disorder (grade 1), mitral valve insufficiency (grade 2) and sinus bradycardia (grade 1); no atrial fibrillation episodes were reported. Grade 1 to 3 hypertension was reported in three cases, of which two patients had a previous history of arterial hypertension. Hematoma was reported in five cases (grade 1 and 2) and one case of grade 3 cerebral hemorrhage occurred in a patient on prophylactic concomitating aspirin.
Potentially immune-related disorders, of interest in the context of checkpoint inhibitors, included two cases of thyroid disorders (hypothyroidism, grade 2), pyrexia (12 cases, grade 1–3) and increased liver values (five cases, one hyperbilirubinemia and four transaminitis, grade 1–4).
Overall, three grade 5 adverse events were reported in the safety population and all of them were related to fatal sepsis.
留言 (0)