
記住我


This is an ongoing phase 1b/2 multi-arm clinical trial of mosun-pola in R/R NHL. Here we present the phase 1b dose-escalation cohort in R/R NHL and the single-arm, phase 2 dose-expansion cohort in patients with second-line and later R/R LBCL (Extended Data Fig. 1). The primary efficacy endpoint during dose expansion was independent review committee (IRC)-assessed best ORR. Secondary endpoints included investigator (INV)-assessed best ORR, best complete response rate and complete response rate at the time of the primary response assessment, duration of response (DoR), progression-free survival (PFS) and overall survival. Protocol-defined pharmacokinetic and biomarker endpoints were also assessed. Exploratory endpoints included the proportion of patients who underwent ASCT or allogeneic stem cell transplant (SCT) after achieving a response and the association of response with prognostic subtypes. Safety was evaluated through the incidence and severity of adverse events (AEs).
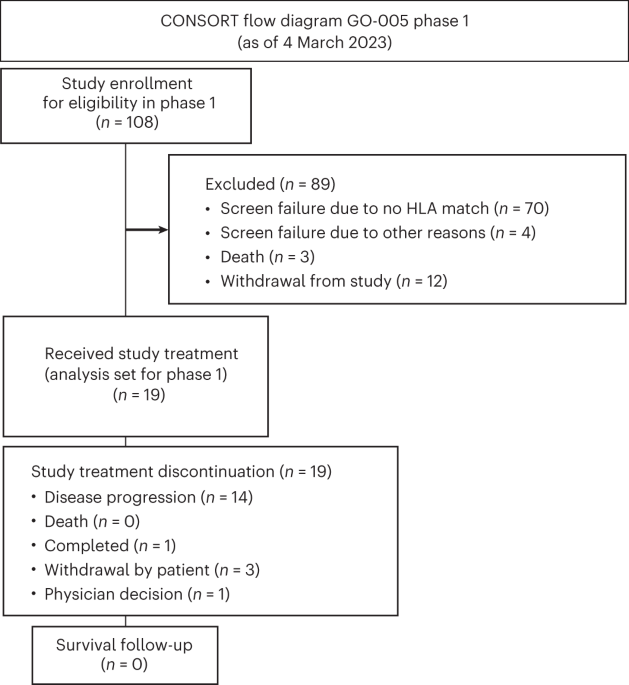
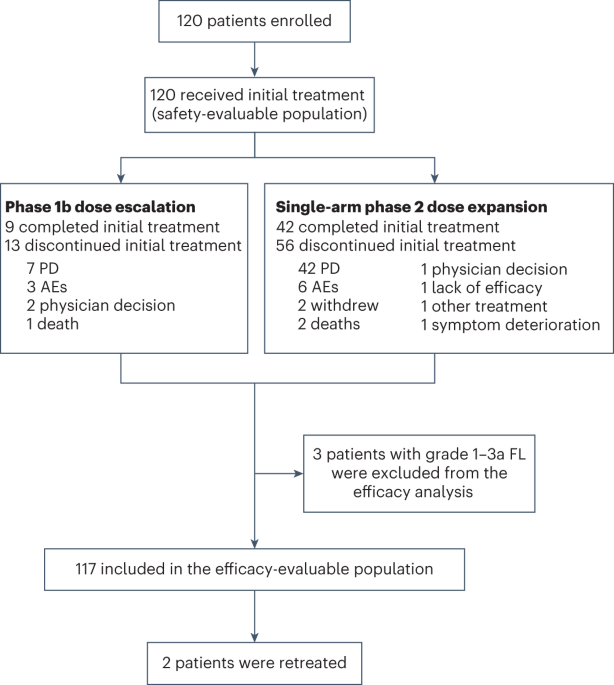
PatientsBetween 25 September 2018 and 14 February 2022, 120 patients were enrolled from 15 sites across two countries (the USA and Canada), with 22 patients treated in the phase 1b dose-escalation cohort (n = 19 with R/R LBCL and n = 3 with R/R FL) and 98 patients treated in the phase 2 dose-expansion cohort (n = 98 with R/R LBCL) (Fig. 1). The overall safety population (n = 120) included all patients with DLBCL, high-grade B cell lymphoma (HGBCL), transformed FL, grade 3b FL or grade 1–3a FL, as described in the Methods. The overall efficacy population (n = 117) excluded three patients with histologically confirmed grade 1–3a FL.
Fig. 1: Patient disposition.
A total of 22 patients were treated in the phase 1b dose-escalation cohort (n = 19 with R/R LBCL and n = 3 with R/R FL) and 98 patients in the phase 2 dose-expansion cohort (all with R/R LBCL). PD, progressive disease.
Baseline demographics and clinical characteristics of the overall R/R NHL population (n = 120) and the phase 2 dose-expansion R/R LBCL cohort treated at the recommended phase 2 dose (RP2D) are described in Table 1. In the overall population, the median age was 68 years (range, 20–88); 85% had advanced-stage disease; and 64.2% had extranodal disease. Overall, 75 patients (62.5%) had DLBCL, 23 (19.2%) had HGBCL, 11 (9.2%) had transformed FL, eight (6.7%) had FL grade 3b and three (2.5%) had FL grade 1–3a. Of 109 patients with LBCL, 22 (20.2%) had double-hit or triple-hit lymphoma (DH/THL) (Table 1). The overall population received a median of two prior lines of therapy (range, 1–10), including CAR-T cell therapy (n = 42 [35.0%]) and ASCT (n = 15 [12.5%]). Sixty-nine patients (57.5%) were primary refractory, 93 (77.5%) were refractory to their last prior therapy and 100 (83.3%) were refractory to any prior anti-CD20 therapy. Among 42 patients who received prior CAR-T cell therapy, 33 (78.6%) were refractory to prior CAR-T cell therapy (Table 1). Patient demographics and clinical characteristics were comparable between the overall population and the dose-expansion cohort (Table 1). There were five major protocol deviations from the inclusion criteria, all related to missing tumor biopsy samples at screening. One major protocol deviation from the exclusion criteria was due to the patient not having the protocol-required 4-week washout period after prior rituximab treatment. None of these deviations was deemed to have a major impact on the overall efficacy or safety endpoints of this study.
Table 1 Baseline characteristics in the overall population (all patients with R/R NHL in the dose-escalation and dose-expansion cohorts; n = 120) and the dose-expansion cohort (R/R LBCL; safety-evaluable population; n = 98)Phase 1b dose escalation to determine the RP2DMosunetuzumab was administered intravenously in 21-day cycles with cycle 1 step-up dosing: 1 mg on cycle 1, day 1 (C1D1); 2 mg on C1D8; escalated to a loading dose (9 mg, 20 mg, 40 mg or 60 mg) on C1D15 and C2D1; and then continued at the target dose (9 mg, 20 mg, 40 mg or 30 mg) from C3 onwards. Patients with a complete response completed mosunetuzumab after C8, whereas those with a partial response or stable disease continued mosunetuzumab for a total of 17 cycles. Polatuzumab vedotin was administered intravenously before mosunetuzumab at the standard dose of 1.8 mg/kg on D1 of C1–C6 (see Methods for additional details).
The maximum tolerated dose (MTD) was not reached with any of the mosunetuzumab dosing schedules investigated: 1/2/9 mg (n = 7), 1/2/20 mg (n = 3), 1/2/40 mg (n = 6) and 1/2/60/30 mg (n = 6). One dose-limiting toxicity (DLT; see protocol in the Supplementary Appendix for DLT definitions) was observed in a patient at the 1/2/40 mg dose who developed asymptomatic, new-onset grade 3 atrial fibrillation. The RP2D of mosunetuzumab was determined to be 1/2/60/30 mg in combination with polatuzumab vedotin 1.8 mg/kg, with six patients treated at this dose and schedule during this part of the study.
In the phase 1 cohort, per INV assessment, best overall complete response rate based on positron emission tomography-computed tomography (PET-CT) and/or CT scan was 47.4% (9/19; 95% CI: 24.5–71.1), and best ORR was 63.2% (12/19; 95% CI: 38.4–83.7), with median DoR not reached (95% CI, 6.3–NE) based on a median follow-up of 41.5 months.
Efficacy outcomes in the phase 2 dose-expansion cohortNinety-eight patients with R/R LBCL were treated at the 1/2/60/30 mg mosunetuzumab dose schedule in combination with 1.8 mg/kg polatuzumab vedotin. At the data cutoff date (6 July 2023), the median follow-up was 23.9 months (95% CI: 21.3–26.8). Median treatment durations of mosunetuzumab and polatuzumab vedotin were 4.9 months and 3.5 months, respectively, with patients receiving a median of eight mosunetuzumab cycles and six polatuzumab vedotin cycles. Forty-two patients (42.9%) completed initial treatment, and 56 patients (57.1%) discontinued due to progressive disease (n = 42), AEs (n = 6), death (n = 2), patient withdrawal (n = 2), lack of efficacy (n = 1), use of another anti-cancer therapy (n = 1), physician decision (n = 1) or symptomatic deterioration (n = 1).
Efficacy results are shown in Table 2. The primary efficacy endpoint of best ORR by IRC by Lugano 2014 response criteria30 was met. Best ORR by IRC assessment, based on PET-CT and/or CT scan, was 59.2% (95% CI: 48.8–69.0; P = 0.0003 at 2.5% one-sided level of significance using an exact binomial test, compared to a historical control rate of 42%)31. Best complete response was 45.9% (95% CI: 35.8–56.3; Table 2). Among 58 responders, the Kaplan–Meier-estimated median DoR was 20.8 months (95% CI: 14.2–NE; Fig. 2a and Table 2), and the 24-month event-free rate was 49.7% (95% CI: 34.3–65.2). Among the 45 patients with complete response, median duration of complete response (DoCR) was not reached (95% CI: 20.5–NE; Fig. 2b), and the Kaplan–Meier-estimated 24-month event-free rate was 60.8% (95% CI: 43.2–78.4; Table 2). Median IRC-assessed PFS was 11.4 months (95% CI: 6.2–18.7). Median overall survival was 23.3 months (95% CI: 14.8–NE; Fig. 2d).
Table 2 Efficacy summary in the R/R LBCL overall population (that is, all patients with R/R LBCL in the dose-escalation and dose-expansion cohorts; n = 117) and the dose-expansion cohort (R/R LBCL; efficacy-evaluable population; n = 98)Fig. 2: Kaplan–Meier plots by IRC.
a, DoR in responders (n = 58). b, DoCR in complete responders (n = 45). c,d, Progression-free survival (c) and overall survival (d) in the dose-expansion cohort (n = 98; efficacy-evaluable population).
Per INV assessment, best ORR was 63.3% (95% CI: 52.9–72.8), and best complete response was 51.0% (95% CI: 40.7–61.3) (Table 2). DoR and DoCR are shown in Extended Data Fig. 2a,b. Concordance between IRC and INV assessments of DoR was 82%. Six patients who were initially assessed as achieving partial response converted to complete response at subsequent follow-up assessments. Five patients converted from partial response to complete response before completion of C8. One patient with a partial response at the end of C8 converted to complete response after continuing with additional mosunetuzumab until C17. Median DoR was prolonged in patients with complete response versus partial response (not reached (95% CI: 16.1–NE) versus 3.1 months (95% CI: 2.8–10.2)) (Extended Data Fig. 2c). Kaplan–Meier-estimated PFS according to INV is shown in Extended Data Fig. 2d.
Patients with complete response who subsequently progressed after initial treatment were permitted to receive mosun-pola retreatment. Two patients were retreated (one experienced a complete response and one a partial response) with both responses lasting more than 6 months before progression.
Efficacy in high-risk subgroupsPrespecified subgroup analyses of IRC-assessed best ORR and complete response rates using PET-CT in the phase 2 dose-expansion cohort are shown in Fig. 3. Durable responses were observed with mosun-pola in patients with high-risk pathology or clinical disease course.
Fig. 3: Prespecified subgroup analysis of complete response and ORR in the dose-expansion cohort.
a,b, Complete response (CR) rates (a) and ORR (b) were determined by an IRC. Squares denote the rates, and error bars indicate two-sided exact Clopper–Pearson 95% CIs. The dashed line indicates the response in the overall main analysis cohort (n = 98). ABC, activated B cell-like; GEP, gene expression profiling; trFL, transformed follicular lymphoma.
Median PFS was 16.5 months (95% CI: 5.6–23.4) in patients who had received one prior line of therapy and 11.4 months (95% CI: 5.7–18.7) in those who had received two or more lines. In patients with DH/THL, median DoR and PFS were 20.5 months (95% CI: 3.0–NE) and 6.2 months (95% CI: 2.6–16.5), respectively. In 35 patients who received prior CAR-T cell therapy in the dose-expansion cohort, the median DoR was NE (95% CI: 8.8–NE), and the median PFS was 9.6 months (95% CI: 4.9–NE). In 26 patients who were refractory to CAR-T cell therapies, the median DoR was 12.5 months (95% CI: 2.8–NE), and the median PFS was 5.7 months (95% CI: 4.3–11.5). In patients with primary refractory disease, median DoR and PFS were 20.5 months (95% CI: 6.7–NE) and 8.5 months (95% CI: 4.9–16.9), respectively.
Treatments after progression or completion of mosun-polaOverall, 52 patients received subsequent anti-lymphoma treatment after mosun-pola. Four patients received ASCT as consolidative therapy, including two patients who achieved a complete response and received consolidative ASCT at the end of mosun-pola treatment. Seven patients received allogeneic SCT, including two patients who achieved a complete response with mosun-pola and subsequently received allogeneic SCT as consolidative therapy. Overall, 13 patients received CAR-T cell therapy, one of whom received CAR-T cell therapy while in partial response to mosun-pola. Five patients received polatuzumab vedotin–based therapy in the context of a polatuzumab vedotin–containing regimen as the next line of therapy.
SafetySafety of mosun-pola was consistent in the overall safety population and in the phase 2 dose-expansion cohort treated at the RP2D (Table 3 and Extended Data Table 1). The most common (≥20%) AEs of any grade in the overall safety cohort were fatigue (46.7%), neutropenia (35.0%), diarrhea (30.8%), nausea (30.0%), decreased appetite (22.5%), headache (21.7%), pyrexia (20.0%) and dry skin (20.0%) (Table 3).
Table 3 AE summary in the overall cohort (R/R NHL in the dose-escalation and dose-expansion cohorts; n = 120) and the dose-expansion cohort (R/R LBCL; n = 98)Grade 3/4 AEs were reported in 56.7% of patients in the overall safety cohort, and the most common (≥5%) grade 3/4 AEs were neutropenia (25.0%) and fatigue (6.7%) (Table 3). Causality of treatment-related AEs was assessed by the INV. Treatment-related grade 3/4 AEs occurred in 38.3% of patients, and grade 5 AEs (not including progressive disease) occurred in five patients (two patients (1.7%) had COVID-19 pneumonia, and one patient (0.8%) each had respiratory failure, sudden cardiac death and pneumonia). Twelve patients (10.0%) experienced AEs that led to mosunetuzumab and/or polatuzumab vedotin discontinuation, of which eight were considered treatment related: one event each of pneumonitis (grade 3), cellulitis (grade 3) and encephalopathy (grade 4); two events of peripheral neuropathy (grade 1 and 2, respectively); and three events of peripheral sensory neuropathy (two grade 2 and one grade 3). AEs led to mosunetuzumab dose interruption in 45 patients (37.5%) and polatuzumab vedotin dose modification/interruption in 39 patients (32.5%) (Table 3).
Cytokine release syndrome (CRS) occurred in 20 of 120 patients (16.7%; Table 3). Twelve patients (10.0%) had grade 1 CRS; five (4.2%) had grade 2 CRS; and three (2.5%) had grade 3 CRS. CRS onset most commonly occurred after C1D1 (eight patients, 6.7%) or C1D15 (11 patients, 9.2%), and two patients (1.7%) had CRS after C1D8. One patient had recurrent CRS with a grade 1 event after C1D1, a further grade 2 event after C1D15 and then no subsequent events (Extended Data Fig. 3). The median time to first CRS onset relative to the most recent dose was 1 day (range, 0–2), and the median duration of CRS was 2 days (range, 1–5). No patients developed CRS events beyond C1. CRS management strategies consisted of corticosteroids in six of 20 patients (30.0%), intravenous fluids in four of 20 patients (20.0%), tocilizumab in three of 20 patients (15.0%), and a single vasopressor and high-flow and low-flow oxygen each in two of 20 patients (10.0%) (Extended Data Table 2). Rates of CRS in the dose-expansion cohort were consistent with those in the overall population (any-grade CRS in 18/98 patients (18.4%), including grade 1 in 10 patients (10.2%), grade 2 in five patients (5.1%) and grade 3 in three patients (3.1%)) (Table 3).
Treatment-related neurologic AEs potentially consistent with immune effector cell–associated neurotoxicity syndrome (ICANS) occurred in six patients (5.0%) in the overall safety population, of whom five (5.1%) were in the dose-expansion cohort. Five patients had grade 1 events of lethargy, attention changes, syncope, confusion and mental status change, respectively. One patient had grade 4 encephalopathy on study D12 in the context of baseline mild dementia made worse from hospitalization and acute congestive heart failure leading to hypoxia. Another patient had grade 3 confusional state and grade 3 dysarthria in the setting of concurrent grade 2 CRS and grade 3 pneumonia (all starting on study D23), and the patient ultimately died from pneumonia.
Peripheral neuropathy occurred in 37 of 120 patients (30.8%), of whom 35 (29.2%) experienced events that were considered related to treatment. Of these, 34 patients (28.3%) had grade 1 or 2 events, and three patients (2.5%) had grade 3 events, which included two events of neuropathy peripheral and one event of sensory peripheral neuropathy. Among 37 patients who experienced peripheral neuropathy events, 11 (29.7%) had recovered by the time of data cutoff. Median time to onset of first peripheral neuropathy events was 39 days (range, 1–223), with a median duration of 55 days (range, 1–353). Five patients (4.2%) experienced peripheral neuropathy events that led to polatuzumab vedotin discontinuation. Similar rates of peripheral neuropathy were observed during dose expansion, in which events occurred in 28 patients (28.6%; all grade 1 or 2) and were considered to be related to treatment in 26 patients (26.5%).
Neutropenia occurred in 42 of 120 patients (35.0%; grade 3 or 4, 25.0%), of whom 38 (31.7%) experienced neutropenia that was considered related to treatment. A total of 33 of 40 patients (82.5%) with recovered/resolved neutropenia received granulocyte colony-stimulating factor. The median time to onset of neutropenia was 43 days (range, 2–168), and the median duration was 8 days (range, 1–809). There were no events of febrile neutropenia. No serious infections with concurrent neutropenia were noted. Rates of neutropenia in the dose-expansion cohort were consistent with those in the overall population (any-grade neutropenia in 29/98 patients (29.6%), grade 3 or 4, 20.4%), and 27 patients (27.6%) experienced neutropenia that was considered related to treatment.
Tumor flare events were reported in three patients (2.5%), all of which occurred before C2. All events were grade 1, non-serious and resolved by the time of data cutoff.
Infections occurred in 47 of 120 patients (39.2%; grade 3 or 4, 8.3%), of whom 17 (14.2%) experienced infections that were considered related to treatment. The most common infection was pneumonia in 11 patients (9.2%). Grade 5 infection occurred in three patients (2.5%), including one event of non-COVID pneumonia and two events of COVID-19 pneumonia. Ten patients (8.3%) had COVID-associated AEs. Among these, five patients (4.2%) were reported to have COVID-19 (including one grade 3 event and one grade 4 event). Another five patients (4.2%) were reported to have COVID-19 pneumonia, of whom two (1.7%) had grade 3 events and two (1.7%) had grade 5 events (previously described). One patient (0.9%) had grade 3 severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) sepsis, and one patient (0.9%) had grade 2 coronavirus test positive. In these 10 patients with COVID-related events, two patients (1.7%) had serious COVID-19, and four patients (3.3%) had serious COVID-19 pneumonia. Rates of infection in the dose-expansion cohort were consistent with those in the overall population (any-grade infection in 40/98 patients (40.8%); grade 3 or 4, 8.1%), and 13 patients (13.3%) experienced infection that was considered related to treatment.
PharmacokineticsThe pharmacokinetics of mosunetuzumab administered in combination with polatuzumab vedotin in the phase 2 dose-expansion cohort were comparable to those previously reported with single-agent mosunetuzumab (Extended Data Fig. 4)15,21.
PharmacodynamicsT cell activation, using the early activation marker CD69, was not observed after polatuzumab vedotin administration alone. However, percentages of both CD69+CD4+ and CD69+CD8+ T cells were elevated 2 h after mosunetuzumab administration at the initial step-up dose (C1D1) and at the target dose on D15 (Extended Data Fig. 5a). Increases in HLA-DR+ T cells were observed after mosunetuzumab administration on C1D15 and C2D1 (Extended Data Fig. 5b). Consistent with the pharmacodynamic effects of mosunetuzumab on T cells, margination was not observed with polatuzumab vedotin alone but was seen with subsequent doses of mosunetuzumab. Overall, prior exposure with polatuzumab vedotin did not negatively influence the previously observed pharmacodynamic effects on T cells seen with mosunetuzumab monotherapy (Extended Data Fig. 5c)32. There was no clear association of these pharmacodynamic changes with clinical response.
B cell recovery was assessed given that the mosun-pola regimen targets two distinct B cell lineage markers. B cell counts were evaluated in patients who achieved a complete response. Patients with partial response or stable disease were excluded from the analysis, as circulating tumor B cells and loss of long-term follow-up at time of progression could confound interpretation. Twenty-seven patients who achieved a complete response and had at least one B cell measurement at baseline, during treatment and during the follow-up period were included in this subset analysis. The median follow-up was 25 months (range, 13.5–35.9) for these 27 patients. Median time to B cell recovery, defined as CD19+ cells ≥70 cells per microliter (cells/µl), was 12.4 months (95% CI: 11.9–NE) from completion of C8 (13/27 patients) (Extended Data Fig. 6).
留言 (0)