Randomized Trial Analysis
Designs of the FINCH 1 (inadequate response to MTX [MTX-IR]; NCT02889796) [7], FINCH 2 (inadequate response to biologic disease-modifying antirheumatic drugs [bDMARD-IR]; NCT02873936) [8], and FINCH 3 (MTX-naïve; NCT02886728) [9] trials have been described previously. The FINCH 1 study randomized patients with MTX-IR active RA in a 3:3:2:3 ratio to FIL200 + MTX, FIL100 + MTX, subcutaneous adalimumab 40 mg every 2 weeks + MTX, or placebo + MTX [7]. Eligible patients had ≥ 6 swollen joints and ≥ 6 tender joints both at screening and day 1 despite ongoing MTX treatment for ≥ 12 weeks with stable treatment at 7.5–25 mg/week for ≥ 4 weeks. In FINCH 2, patients with active RA who were bDMARD-IR were randomized 1:1:1 to once-daily FIL200 + stable conventional synthetic DMARDs (csDMARDs, including MTX), FIL100 + csDMARDs, or placebo + csDMARDs [8]. Eligible patients had ≥ 6 swollen joints and ≥ 6 tender joints at both screening and baseline and a serum CRP level of 4 mg/l or greater based on central laboratory assessment at screening. The FINCH 3 study randomized patients who were MTX-naïve with active RA in a 2:1:1:2 ratio to FIL200 + MTX, FIL100 + MTX, FIL200 monotherapy, or MTX [9]. Eligible patients had limited (< 3 doses ≤ 25 mg) or no prior MTX exposure, swollen joint count ≥ 6 of 66 joints, and ≥ 6 tender joints of 68 joints at screening and day 1.
The randomized trials were conducted in accordance with the Declaration of Helsinki and the International Council for Harmonisation guidelines. Protocols were approved by the institutional review board or ethics committee at each site. All participants provided written informed consent on enrollment. FINCH 1 was approved by the Advarra Central Institutional Review Board (Reference # 00000971). FINCH 2 was approved by the Administrative Panel on Human Subjects in Medical Research (Reference # 4593). FINCH 3 was approved by the Ethics Committee Research UZ/KU Leuven (Reference # S59627).
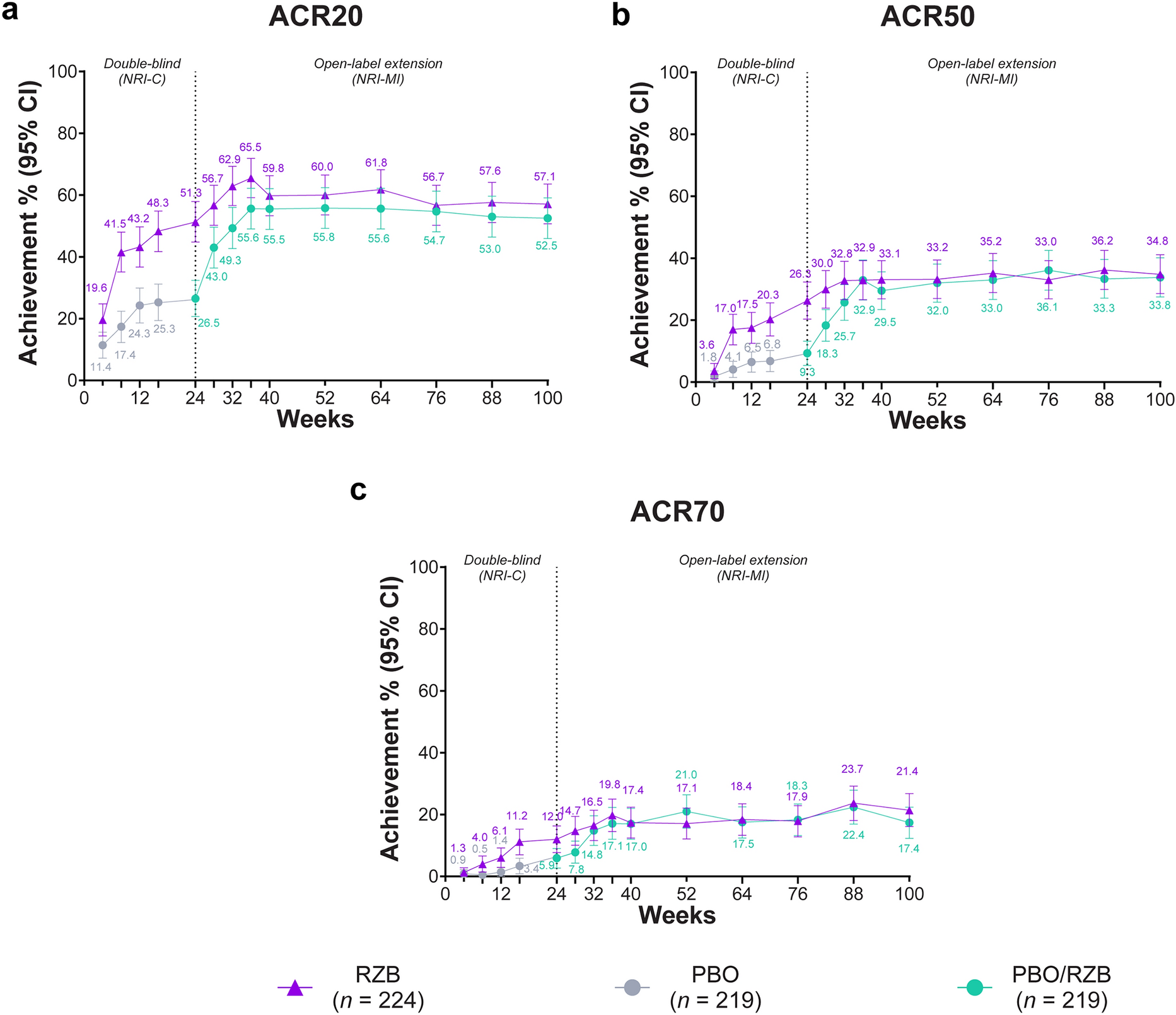
Multivariable-adjusted logistic regression models were fitted to assess the effects of self-reported current, former, or never smoking status on the likelihood of obtaining low disease activity, as measured by week 12 Disease Activity Score in 28 joints with CRP (DAS28[CRP]) ≤ 3.2. Additional efficacy endpoints included American College of Rheumatology 20, 50, or 70% improvement (ACR20, ACR50, ACR70), Clinical Disease Activity Index (CDAI) low disease activity (≤ 10), and DAS28(CRP) remission (< 2.6). Missing patient-response data were imputed using non-responder imputation (109/1755 [6%] of patients with MTX-IR, 47/448 [10%] of patients with bDMARD-IR, and 99/1249 [8%] of patients who were MTX-naïve were non-responders imputed). Baseline factors (selected based on the authors’ subject-matter expertise) were tested for association with DAS28(CRP) ≤ 3.2 response at week 12 after stratification for smoking status (self-reported as no history of smoking, former history of smoking, or current smoking); those with significant (p < 0.05) association were included as covariates in each model (Supplementary Materials Table 1). Displayed response rates and confidence intervals were determined from the logistic regression models. All p values are nominal, without adjustment for multiple testing.
Table 1 Baseline demographic and clinical characteristics among subgroups by smoking status across the FINCH 1, FINCH 2, and FINCH 3 randomized trialsInsurance Claims-Based Study
A retrospective, US-based cohort study was conducted using PharMetrics Plus data between January 1, 2006 and October 31, 2021. Patients with RA and a history of exposure to certolizumab, golimumab, etanercept, abatacept, infliximab, adalimumab, or tocilizumab were included in the cohort (baricitinib, tofacitinib, and rituximab were not approved for first-line biologic or targeted-therapy treatment in the US, and exposure to these drugs was not considered in the inclusion criteria) [11,12,13]. Patients aged < 18 years or with < 6 months of follow-up were excluded. A new-user design was employed in which patients were followed from the date of prescription of first biologic until the earliest date of switch to a different biologic or JAK inhibitor, loss of insurance coverage, or end of the study period. Recognizing that patients may switch medications for any number of possible reasons, treatment switching was the outcome of interest as a proxy for lack of medication effectiveness, as efficacy outcomes were not available from the claims data. A Cox proportional hazards model was used to estimate time to switch to a new RA biologic or JAK inhibitor drug in different smoking status groups (defined by ICD-9 or ICD-10 codes: 3051, 6490, 98,984, F172, 09933, P042, P9681, T652, Z716, and Z720 for current smokers; V1582 and Z878 for former smokers; patients with none of these codes were assumed to be non-smokers) while adjusting for sex, age, previous and ongoing csDMARD use, time since first RA diagnosis code appearing in the data, and corticosteroid use.
Patient and Public Involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination of plans of this research.




留言 (0)