
記住我





We used the National Health Insurance Service (NHIS) database, which covers nearly all Koreans (97.2% of the Korean population) and is managed by the Korean government. The NHIS encourages annual or biennial standardized health check-ups for all insured Koreans older than 40 years and employees older than 20 years. The NHIS contains the following information for each participant: demographics; lifestyle behaviors, including a PA questionnaire; anthropometric measurements; examinations; medical history, such as claims for disease diagnosis codes of the International Classification of Diseases (ICD-10); and treatments, including procedures performed and medications prescribed.
This study protocol was conducted in accordance with the ethics guidelines of the Helsinki Declaration of 1975 and was given an exemption by the Institutional Review Board of Seoul National University Hospital (H-2211-004-1373). The requirement for informed consent was waived because of the retrospective study design, and the researchers only accessed anonymous data for analytical purposes.
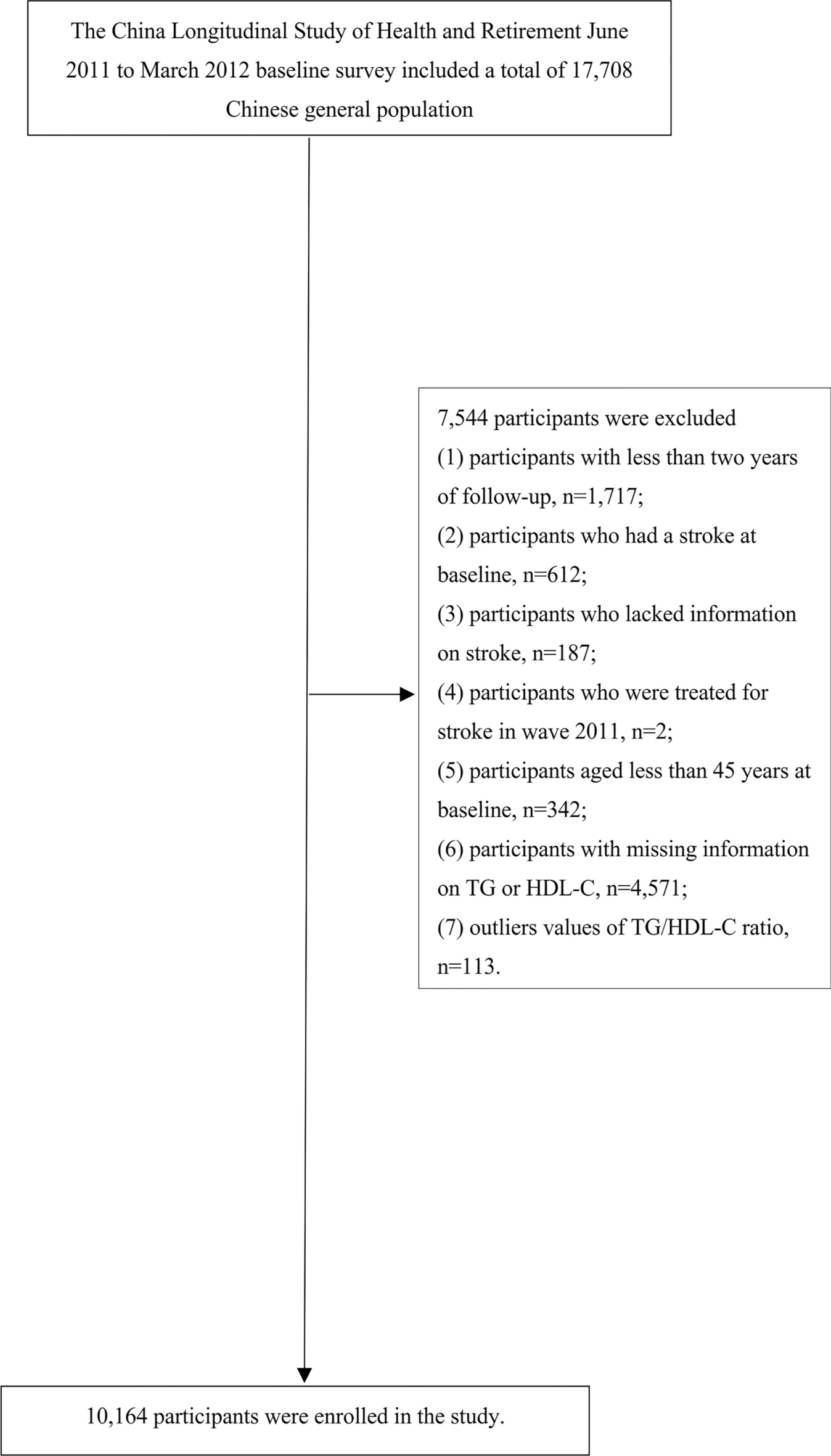
Study populationParticipants older than 20 years of age who underwent the Korean Health Screening in 2009 were initially included. Among them, participants with missing data were excluded. In addition, participants who were diagnosed with a major cardiovascular disease (stroke (I63, I64) or myocardial infarction (I21, I22)) or who had a history of major cardiovascular disease (heart disease or stroke) based on a questionnaire were excluded. Then, participants who died or had an event within 1 year (1 lag period) were also excluded. The included participants were followed up until December 2018 (Fig. 1).
Fig. 1
Flowchart of the study enrollment
PA measurementsThe PA questionnaire used by the Korean National Health Insurance Service (KNHIS) in 2009 was the last 7-day recall and is a well-validated questionnaire for national monitoring [11, 12]. Each question is used to determine the frequency of light, moderate and vigorous PA. Each individual marked how many days during the last 7 days they performed each grade of PA (Additional file 1: Table S1) [12]. To estimate the overall amount of PA in a quantitative manner, we calculated the metabolic equivalent (MET), which is widely used in medical research to quantitatively measure PA amount [13, 14]. According to The 2011 Updates on Compendium of PA, we appropriated 8, 5 and 3 METs to each question, and MET-minutes per week were calculated as follows: MET value x minutes spent per week [12,13,14]. According to MET-minutes/week, PA amount was grouped as follows: Group 1 (0), Group 2 (1-499), Group 3 (500-999), Group 4 (1000-1499), and Group 5 (≥ 1500 MET-minutes/week).
Diagnosis of MSThe diagnosis of MS was defined according to the harmonizing criteria [15]. MS was diagnosed if 3 or more of the following components were present: (1) increased waist circumference (≥ 90 for Asian men and ≥ 80 cm for Asian women); (2) high blood triglycerides (≥ 150 mg/dL) or use of a relevant drug; (3) low high-density lipoprotein cholesterol level (< 40 mg/dL for men and 50 mg/dL for women) or use of a relevant drug; (4) high blood pressure (systolic ≥ 130 mmHg and/or diastolic ≥ 80 mmHg) or use of an antihypertensive medication; and (5) high blood sugar level (≥ 100 mg/dL) or use of an antidiabetic drug.
Measurement of clinical parameters and biochemical analysisThe standardized self-administered questionnaires included age, sex, smoking status, alcohol consumption, annual income, PA and underlying diseases.
Height (m) and body weight (kg) were measured using an electronic scale. BMI was calculated as follows: BMI = body weight (kg)/height2 (m2). The waist circumference (WC) was measured using a tape measure at the midpoint between the lower costal margin and the iliac crest by a trained examiner. The systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured after 5 min of rest.
Blood samples were collected after overnight fasting. The biochemical analysis included assessments of serum fasting glucose, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and triglycerides. All laboratory analyses were performed using standardized laboratory methods.
The diagnoses of hypertension, diabetes mellitus (DM) and dyslipidemia were defined using anthropometric measurements and laboratory data (SBP 140 mmHg or DBP 90 mmHg; fasting glucose level ≥ 126 mg/dL; total cholesterol levels ≥ 240 mg/dL) or ICD codes (ICD I10 to I13 or I15; E11 to E14; E78) and medication use, including antihypertensive medication, insulin or oral hypoglycemic agents, and dyslipidemia medication.
OutcomesThe primary outcome was all-cause mortality. The NHIS database includes whether a person died during the follow-up duration of the study (until 31 Dec 2018) and the death date if a person died. The secondary outcome was incident CVD, including myocardial infarction and stroke. Stroke was defined when the ICD code I63 or I64 was used with hospitalization and when a claim for an imaging study, including magnetic resonance imaging or computed tomography, was made. Myocardial infarction was diagnosed when ICD code I21 or I22 was used with hospitalization.
Statistical analysisContinuous variables are expressed as the means ± standard deviations, and categorical variables are expressed as numbers and percentages. Between-group comparisons were performed using Student’s t test or a one-way analysis of variance for continuous variables and chi-square tests for categorical variables. Log transformation was performed for nonnormally distributed variables. All-cause mortality or incident cardiovascular disease was calculated as the number of events per 1,000 total person-years. Multivariable Cox proportional hazards regression analyses were performed after adjustment for covariates, in which estimates were presented as adjusted hazard ratios (aHRs) with 95% confidence intervals (CIs).
The interaction term “presence of MS” x “amount of PA” was analyzed to evaluate whether there was a multiplicative interaction between the presence of MS and the amount of PA on all-cause mortality.
Statistical analyses were performed using R version 3.2.3 (The R Foundation for Statistical Computing, Vienna, Austria) and SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). A two-sided P value less than 0.05 was considered statistically significant.
留言 (0)