Familial Hypercholesterolemia (FH) is a common treatable monogenic disorder found throughout the world with an estimated prevalence of 1 in 300 people in the largest analysis to date, though various regional population estimates range from approximately 1 in 100 to 1 in 500. 1 Untreated FH increases mortality 25-fold by age 60-years 2 by causing nearly 20% of myocardial infarctions prior to the age of 45 3 and conveying a 50% risk for males (historically higher than females) for a myocardial infarction before age 50-years. 1, 2, 3 Despite these outcomes, only ∼1% of the FH population has been diagnosed and specifically treated for it in most countries, including the United States (US), where there are 600,000 to >1 million people presumed to have FH. 4, 5, 6 Pharmacotherapy may occur without the diagnosis but guidelines on LDL-C for FH may not be followed and lead to undertreatment of affected individuals. 5 In children, the disorder can be strongly suspected with LDL-C (low-density-lipoprotein-cholesterol) ≥160 mg/dL (≥4.1 mmol/L) and an appropriate family history, 7, 8, 9 or genetic testing for up to 4 known genes with causative mutations (LDLR, APOB, PCSK9, LDLRAP1). 4,10 Genetic screening in children with suspected personal or family history of FH is one of only three Tier 1 recommendations from the Centers for Disease Control. While their recommendation is not a call to initiate universal pediatric lipid screening, it further underscores the importance of treating FH as a public health priority. 11
There is limited evidence of meaningful improvement in LDL-C in children from lifestyle therapy with or without FH. 12,13 Still, lifestyle therapy controls other risk factors for early coronary artery disease and remains a cornerstone of therapy. Pharmacotherapy (generally with a statin) starting in childhood as early as age 8-10 years has a profound effect in FH on LDL-C, 9,14, 15, 16, 17 in some cases reducing carotid intima-media thickness already present in young children, 15,17 and possibly decreasing the risk of cardiovascular disease to the level of the general population. 17 While these studies and decades of suggestive observations and expert recommendations from the American Academy of Pediatrics, the National Lipid Association and the National Heart, Lung and Blood Institute are compelling, the United States Preventive Services Task Force has recently found insufficient evidence to adopt universal pediatric lipid screening, 7,9,18, 19, 20, 21, 22, 23 and US healthcare providers have been reluctant to adopt screening or treatment for FH. 8,24,25 Slovenia may be unique to reliably provide this preventive care under a governmental mandate, 26 but undertreatment remains rampant throughout most of the world. 5
Pediatricians report discomfort with interpretation of lipid results 21 and may prioritize screening overweight/obese children who are not at higher risk for FH, but who may benefit from enhanced nutritional advice and other lifestyle changes. 18,22,23 When extremely high LDL-C is found, there is no clear agreement among pediatricians that pharmacotherapy is advisable in childhood 21,22 despite the evidence and guidelines supporting it for FH. 7, 8, 9
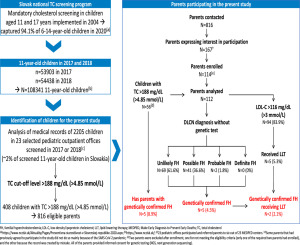
Our study reports on the clinical experience with pediatric lipid screening in Kaiser Permanente Southern California, a large healthcare system managing 4.7 million enrollees (over 1% of the US population) including 930,000 children. In this practice, universal pediatric lipid screening 27 at age 9 to 11-years is recommended (though the recommendation was also stated as “optional” until 2020). A second screen at age 11 to 16-years is recommended for overweight/obesity or if screening was missed during age 9-11 years. A third screen is recommended for all people 17 to 21-years, but only age 17-years applies to pediatrics providers in this medical group because 18-year-olds are transferred to an adult primary care provider. The intent of screening was not specifically stated to identify FH, and we believe that many providers did not likely see that as a consideration or that pharmacotherapy might follow the screening.
We hypothesize that a recommended universal lipid screening strategy without clear messaging on identifying FH, interpreting results, or establishing appropriate follow up planning leads to extremely low success at identifying FH cases and initiating appropriate pharmacotherapy. Still, determining the deficiencies more precisely in these data may suggest specific methods to improve the process.

留言 (0)