
記住我
Pregnant and lactating people (PLP) are at increased risk of acquiring HIV [1] and at elevated risk of vertical HIV transmission when viral loads are elevated [2]. In a national population-based South African evaluation, early vertical HIV transmission was 10.7% for pregnant women who seroconverted in pregnancy [95% confidence interval (CI) = 6.2%, 16.8%] compared with. 2.2% (95% CI = 1.7%, 2.8%) for mothers known to be living with HIV [2,3]. In 2020 alone, roughly 120 000 pregnant or breastfeeding women became newly infected in sub-Saharan Africa, according to UNAIDS estimates [4]. PLP who seroconvert during pregnancy or lactation are at highest risk of vertical HIV transmission and an estimated 45% of new paediatric HIV cases are attributed to incident maternal HIV infection [3,5,6].
Daily oral preexposure prophylaxis (PrEP) TDF/FTC was introduced in South Africa (SA) in 2016 and guidelines were updated in October 2021 to include PrEP for PLP, as recommended by WHO [7,8]. Comprehensive scale-up of oral TDF/FTC for HIV prevention has expanded to reach PLP without HIV. Concerns have been raised about PrEP use during pregnancy and postpartum periods because of the potential for adverse pregnancy and birth outcomes conceivably resulting from in utero antiretroviral exposure [9–11]. Prior studies have evaluated PrEP for safety among PLP without HIV as well as antiretroviral therapy in women living with HIV [12–16]. A recent randomized control trial of n = 540 pregnant women comparing immediate to delayed PrEP use in pregnant women found that PrEP was not associated with preterm birth nor small for gestational age (SGA) [17]. The risk difference for preterm birth was –4.7% (90% CI = –10.7, 1.2), 2.5% for low birthweight, and 0.9% for SGA; all limits exceeded the noninferiority margin [17]. However, the study's exposure was based on randomization to PrEP (not actual use) and was underpowered.
Existing insights into the possible effect of PrEP use on pregnancy outcomes face significant limitations in their reliance on self-reported use. To date, exposure has been measured using self-reported recent adherence or pill counts [17–19], which may result in an over or under-reporting of actual use and drug exposure. Potential nondifferential misclassification of exposure can lead to underestimation of the true measure of effect [20]. Future studies using objective measures of PrEP exposure in PLP are needed to advance knowledge of safety and effectiveness of TDF/FTC as PrEP in PLP. To our knowledge, our study is the first to evaluate pregnancy and birth outcomes in a large cohort of pregnant women using both objective levels of tenofovir diphosphate (TFV-DP) in dried blood spots (DBS) in addition to subjective, self-reported PrEP use.
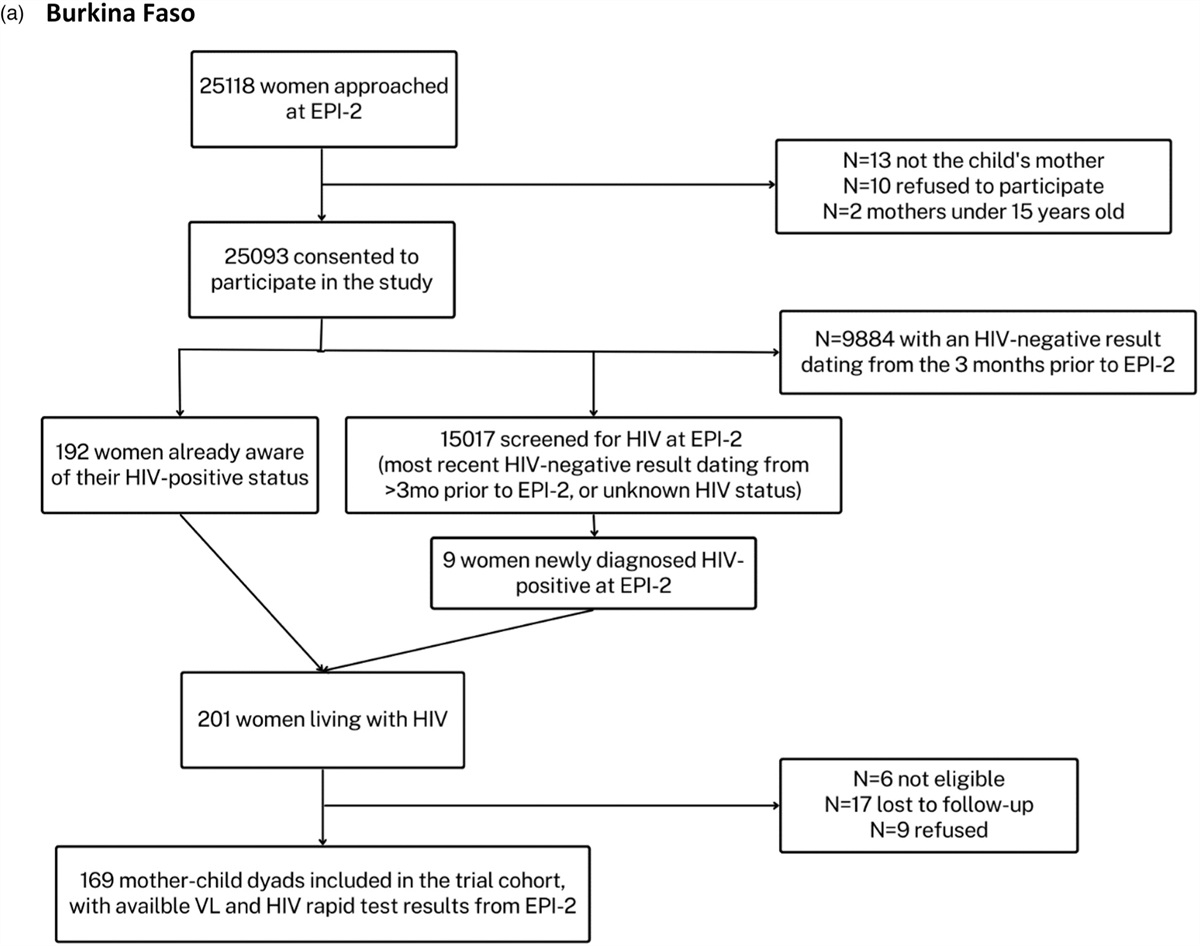
Methods Study design and settingWe conducted a prospective cohort study which enrolled consenting pregnant, adolescent girls and women (age > 15 years) without HIV at their first antenatal clinic (ANC) visit. We followed participants through 12-months postpartum. We recruited from one public health clinic in a peri-urban township in Cape Town, Western Cape. The clinic serves as a public health routine service site, Midwife Obstetric Unit, and primary care facility operated by the Government, serving approximately 350 000 individuals with an estimated antenatal HIV prevalence of 30% [21].
Study participants and procedureThe study recruitment began in August 2019 and concluded in October 2021. Study follow up continued through February 2023. The study protocol has been described elsewhere [22]. Briefly, participating individuals were required to have: confirmed HIV-negative by a fourth generation antigen/antibody HIV test, confirmed pregnancy status, intention to stay in Cape Town through 12-months, and absence of contraindications to PrEP. Women 16–17 years old were eligible to enroll in the study as emancipated minors per national guidance on research participation for adolescents. Healthcare providers at study facility provided group counselling to all pregnant women attending antenatal clinic, which included information on HIV testing, prevention of HIV vertical transmission, and the importance of HIV prevention for women without HIV.
Participants received PrEP counselling from trained study staff and surveys were conducted by study interviewers. Women were counselled to continue with PrEP, condom use and other HIV prevention methods (including partner testing and STI testing/treatment), regardless of recent sexual activity or condom use. As previously described [22,23], women were offered aetiological testing for C. trachomatis, N. gonorrhoeae and T. vaginalis at enrolment study visit. All women with a positive STI test result received treatment in line with the South African National guidelines [24]. Participants were followed antenatally for one to four study visits, depending on the gestational age at enrolment, and postnatally for up to 12 months. The participants were reimbursed 120 South African Rand (∼US$8) in grocery vouchers for their time and effort in the study, as well as remuneration for transportation costs. We enrolled n = 1195 eligible pregnant women in the study.
Data collection and managementAt each visit participants received individual counselling about HIV prevention, including daily oral PrEP. Data collected included maternal demographics, pregnancy history and healthcare information using REDCap [25]. If the participant decided to start PrEP at any visit, the study nurse provided the participant with a one-month supply of TDF/FTC and an invitation card to return in one month for follow-up testing (after which participants received a three-month prescription to correspond with quarterly study follow-up visits). For this study, we restricted analysis to participants who had available pregnancy or birth outcomes.
Study definitionsFor this analysis, exposure to PrEP was defined in two ways:
(1) Any PrEP use during pregnancy, defined as receipt of TDF/FTC prescription during pregnancy and self-reported to have taken any PrEP whilst pregnant. (2) Tenofovir diphosphate (TFV-DP) present in dried blood spots (DBS) among women who reported taking PrEP in the last 30-days, measuring cumulative PrEP adherence over several weeks using erythrocyte intracellular TFV-DP levels detected by liquid chromatography and mass-spectroscopy [26]. We defined objective PrEP use as: any TFV-DP detected DBS results during pregnancy among those on PrEP vs. unquantifiable levels, and categorical TFV-DP detected as below the limit of quantification (BLQ) compared with <2 days/week, 2–6 doses/week and ∼7 doses/week in pregnancy [27]. Pregnancy and obstetric outcomesThe study abstracted pregnancy and infant outcome data from women who returned in postpartum for study visits using maternal case files and infant Road to Health cards. For those who did not return (censored, lost to follow up or moved), pregnancy and obstetric outcomes were abstracted from obstetric records and maternity case records at clinics or hospitals throughout Western Cape. Birth anthropometrics were abstracted from the child Road to Health Booklets at the 7-day postpartum visit where mother-infant pairs were evaluated by study teams. Maternal case records and child Road to Health cards are generally complete, yet may have errors noted by providers in birthweight, etc. If pregnancy loss was reported telephonically, gestational age at event may be incorrect or missing.
Gestational age was estimated based on the date of the last menstrual period or ultrasound dating recorded in the maternity case records at first antenatal care visit. Miscarriage or pregnancy loss was defined as noninduced pregnancy loss ≤20 weeks of gestation. Stillbirth was defined as delivery of a baby with no sign of life ≥20 weeks of gestation, including foetal demise. Neonatal mortality was defined as death of a newborn in the first 28 days of life. Preterm live birth was defined as birth before completion of 37 weeks of gestation. Low birthweight was defined as birthweight < 2500 g. In singleton births, the INTERGROWTH-21st Project Standards was used to calculate birthweights ≤10th percentile for gestational age, classified as small for gestational age (SGA); between 10th and 90th percentiles were classified appropriate for gestational age (AGA); and ≥90th percentile were classified large for gestational age (LGA) [28]. WHO guidelines were used to categorize adverse birth outcomes [29]. The primary outcome of interest was composite adverse outcomes, which included pregnancy loss (miscarriage or stillbirth), neonatal death, and singleton births reported as preterm, low birthweight, or SGA. Separate logistic regression models evaluated outcomes by exposure: self-reported PrEP use after prescription, or TFV-DP during pregnancy (analysed as continuous, categorical [27] [BLQ, <2 doses/week, 2–6 doses/week, ∼7 doses/week], and binary (any vs. none) in pregnant women reporting PrEP use in past 30 days). Models adjusted for maternal age, gestational age at baseline, gravidity, and socio-economic status (composite of maternal education, employment, income, home type and assets). We included gestational age at baseline for a proxy of time in study and time on PrEP.
Imputation processWe imputed missing pregnancy outcome data in supplementary analyses. After removing nonsingleton preterm births, a total sample of n = 1138 of 1145 was used. To assess whether the missing variable was suitable for imputation, all available variables were individually regressed onto each of the missing variables of interest using univariable logistic regression with the outcome of captures vs. missing; infant birthweight (missing, n = 13 of 1138, 1%), SGA (missing, n = 16 of 1138, 1%) and self-reported PrEP exposure (missing, n = 140 of 1138, 12%). Explanatory variable with P-values <0.05 were suggestive of missing at random, and these significant variables were used to impute each of the missing variables respectively (Tables 1 and 2, Supplemental Digital Content, https://links.lww.com/QAD/C979).
A method of multivariate imputation by chained equations (MICE) was used for the imputation processes. For each missing variable within the MICE function, logistic regression was applied for self-report PrEP exposure, while Bayesian linear regression was applied for baby weight at birth. A set of 100 imputed data sets were created. The imputed infant birthweight were bound between 0 to 7 kg. The pooled dataset was used to perform logistic regression to obtain the effect estimates in Table 3, Supplemental Digital Content, https://links.lww.com/QAD/C979.
For participants in which no DBS were taken or analysed (due to budgetary restrictions), a logical inference was made to explore the possible reason for missingness. In the first scenario of extrapolation, participants who self-reported no PrEP exposure during pregnancy or those who received PrEP during pregnancy but did not return for a follow-up visit to confirm they started PrEP while pregnant, were considered as ‘Not on PrEP’ or ‘No TFV-DP Present’. Alternatively, those who had received PrEP during pregnancy and self-reported PrEP use (without a biomarker collected and analysed) were considered as ‘On PrEP’ or ‘Any TFV-DP Present’, thus, increasing numbers in both the exposed to PrEP group and the reference group (Table 4).
EthicsThe PrEP-PP study was approved by the Human Research Ethics Committee at the University of Cape Town (#297/2018) and by the University of California, Los Angeles Institutional Review Board (IRB#18-001622). Written informed consent was provided by all participants in English or isiXhosa.
Results Baseline characteristicsBetween August 2019 and October 2021, we enrolled 1195 pregnant women and 96% (n = 1145) had an ascertained pregnancy or birth outcome rendering them eligible for analysis. Of the 1145 women, 72% (n = 826) confirmed PrEP use during pregnancy (prescription received and self-reported having taken PrEP) and 16% (n = 178) never used PrEP during pregnancy (no prescription or self-report of having taken PrEP), whereas 12% (n = 141) had an unconfirmed PrEP exposure (received prescription but did not return to ascertain if they ever took PrEP). Women who had more than one previous pregnancy were more likely to receive a PrEP prescription during pregnancy (67 vs. 56%, P = 0.017).
The median age of participants was 26 years [interquartile range (IQR): 23–31] and the median gestational age at baseline was 21 weeks (IQR: 15–31). Almost all women (97%) reported being sexually active during pregnancy with 3% (n = 36) reporting more than one partner in the past 3-months. Among women who reported being in a sexual relationship in the past 3-months, 72% reported condomless sex. Almost one-third of women (29%) reported having a partner who was either living with HIV or of unknown serostatus. (Table 1). One woman seroconverted around labour and delivery and was included in this analysis as she was censored after her seroconversion was identified.
Table 1 - Baseline characteristics of pregnant women offered preexposure prophylaxis in antenatal care in Cape Town, South Africa between August 2019 and October 2021. All women, N (%) Received PrEP prescription, n (%) Did not receive PrEP in pregnancy, n (%) P-value Sociodemographic characteristics 1195 (100) 1080 (90) 115 (10) Maternal age (median, IQR) years 26 (23–31) 26 (23–31) 25 (22–31) 0.3 GA at booking (median, IQR) weeks 21 (15–31) 21 (15–30) 23 (13–33) 0.6 Creatinine at booking (median, IQR) μmol/l 46 (41–52) 46 (41–52) 46 (40 – 49) 0.6 BMI at booking (median, IQR) kg/m2 31 (26–36) 31 (26–36) 31 (27–35) > 0.9 Gravidity 0.017 1 405 (34) 354 (33) 51 (44) ≥2 790 (66) 726 (67) 64 (56) Family planning prior to current pregnancy 0.3 No contraception 777 (65) 695 (64) 82 (71) Occasional contraception 325 (27) 301 (28) 24 (21) Using contraception 93 (8) 84 (8) 9 (8) Education level completed 0.2 Some primary 7 (1) 5 (1) 2 (2) Primary 574 (48) 521 (48) 53 (46) Secondary or tertiary 614 (51) 554 (51) 60 (52) relationship with father of child > 0.9 Married/cohabiting 450 (38) 407 (38) 43 (37) Not married nor cohabiting 745 (62) 673 (62) 72 (63) Employment status 0.7 Full-time employment 313 (26) 286 (26) 27 (23) Part-time employment 116 (10) 103 (9) 13 (11) Unemployed or attending school/college 766 (64) 691 (64) 75 (65) Socioeconomic status (SES) 0.3 Low SES 381 (32) 349 (32) 32 (28) Moderate/high SES 814 (68) 731 (68) 83 (72) Personal monthly income 0.8 None 657 (55) 594 (55) 63 (55) <$100 118 (10) 104 (10) 14 (12) $100–350 329 (27) 300 (28) 29 (25) $351+ 91 (8) 82 (7) 9 (8) Psychosocial characteristics EPDS threshold 0.3 Below threshold <11 1106 (93) 996 (92) 110 (96) Above threshold ≥11 89 (7) 84 (8) 5 (4) Alcohol use during current pregnancy 72 (6) 68 (6) 4 (3) 0.3 Ever experienced IPV 147 (12) 137 (13) 10 (9) 0.3 Any STI at enrolment (CT/NG/TV) >0.9 Positive 373 (31) 338 (31) 35 (30) Negative 822 (69) 742 (69) 80 (70) Partner's serostatus 0.4 Concordant HIV-negative 849 (71) 763 (71) 86 (75) Serodiscordant or unknown 346 (29) 317 (29) 29 (25) HIV risk perception at enrolment >0.9 No chance at all 650 (54) 587 (54) 63 (55) Some/high chance 545 (46) 493 (46) 52 (45) Sexual behaviour in the past 3 months Number of sex partners 0.8 No sex partner 33 (3) 29 (3) 3 (3) 1 sex partner 1126 (94) 1018 (94) 108 (94) 2+ sex partners 36 (3) 33 (3) 3 (3) Condom use during sex 0.5 Sometimes/always 298 (25) 271 (25) 27 (23) Never/rarely 864 (72) 780 (72) 84 (73) No sex partner 33 (3) 29 (3) 4 (4) Prior knowledge of PrEP 321 (27) 288 (27) 33 (29) 0.7 PrEP initiation at baseline <0.001 Did not initiate PrEP at baseline 186 (16) 71 (7) 115 (100) Initiated at baseline 1009 (84) 1009 (93) 0 (0)ANC, antenatal care; GA, gestational age; IPV, intimate partner violence; IQR, interquartile range; n, number of participants; PrEP, preexposure prophylaxis; SD, standard deviation.
Among the 1145 for which we had ascertained pregnancy and birth outcomes, 94.5% (n = 1082) had a live birth with a median birthweight of 3.2 kg (IQR: 2.9–3.5). Overall, 5.5% of women experienced pregnancy loss (n = 63), including 3.1% (n = 36) miscarriages (≤20 weeks’ gestation), 2.2% (n = 25) stillbirths (>20 weeks’ gestation), and 0.2% (n = 2) terminations of pregnancy. Among live births, 8.4% were preterm births (n = 91) and 10.2% (n = 110) were low birth weight (<2500 g). Overall, 8.8% (n = 96) were SGA: 8% were SGA among those born full term (n = 87) and 0.8% (n = 9) were SGA among those born preterm (Table 2).
Table 2 - Pregnancy and birth outcomes of women ever exposed compared to women never exposed to PrEP during pregnancy (n = 1145 women with confirmed and unconfirmed PrEP exposure measures and known pregnancy outcomes). All women, N (%) PrEP exposed (self-report), n (%) PrEP unexposed (self-report), n (%) Unconfirmed PrEP exposure (no self-report), n (%) Total of all women with pregnancy outcomes 1145 (100) 826 (72) 178 (16) 141 (12) Pregnancy losses Total pregnancy losses 63 (5.5) 27 (3.3) 10 (5.6) 26 (18.4) Miscarriage GA ≤20 weeks 36 (3.1) 11 (1.3) 5 (2.8) 20 (14.2) Stillbirth GA >20 weeks 25 (2.2) 14 (1.7) 5 (2.8) 6 (4.2) Termination of pregnancy 2 (0.2) 2 (0.2) 0 (0) 0 (0) Live birth outcomes Total live births 1082 (94.5) 799 (96.7) 168 (94.4) 115 (81.6) Full term delivery GA ≥37 weeks 991 (91.6) 731 (91.4) 157 (93.5) 103 (89.6) Preterm delivery GA <37 weeks 91 (8.4) 68 (8.5) 11 (6.6) 12 (10.4) Neonatal death 6 (0.6) 6 (0.8) 0 (0) 0 (0) LBW< 2500 g 110 (10.1) 85 (10.6) 15 (8.9) 10 (8.7) Birth weight (median, IQR) grams 3.2 (2.9–3.5) 3.2 (2.9–3.5) 3.3 (2.9–3.6) 3.3 (2.9–3.5) Gestational age at birth (median, IQR) weeks 39 (38–40) 39 (38– 40) 39 (38–40) 39 (36.8–40) Full term gestational percentiles SGA (≤10th percentile) 87 (8) 67 (8.4) 11 (6.6) 9 (7.8) AGA (>10th and <90th percentile) 767 (70.8) 567 (71) 129 (76.8) 71 (61.7) LGA (≥90th percentile) 107 (9.8) 79 (9.9) 17 (10.1) 11 (9.6) Preterm gestational percentiles SGA (≤10th percentile) 9 (0.8) 7 (0.9) 1 (0.6) 1 (0.9) AGA (>10th and <90th percentile) 60 (5.5) 48 (6) 6 (3.6) 6 (5.2) LGA (≥90th percentile) 14 (1.3) 8 (1) 3 (1.9) 3 (2.6) Composite adverse outcome Adverse outcome 250 (21.8) 169 (20.5) 35 (19.7) 46 (32.6) No adverse outcome 895 (78.2) 657 (79.5) 143 (80.3) 95 (67.4)AGA, appropriate for gestational age; GA, gestational age; IQR, interquartile range; LBW, low birthweight; LGA, large for gestational age; PrEP, preexposure prophylaxis; SGA, small for gestational age.Composite adverse outcome includes all miscarriage, stillbirth, neonatal death, preterm birth, and SGA.
In those with self-reported PrEP use in pregnancy compared to those who did not report PrEP use in pregnancy (n = 1004), there were no observable differences in pregnancy or birth outcomes in crude and adjusted analyses. Pregnancy loss (defined as miscarriage, stillbirth or neonatal death in analyses) did not differ between women with and without self-reported PrEP use exposure, 4% (n = 33) vs. 5.6% (n = 10) (aOR = 0.65, 95% CI = 0.32, 1.47; P = 0.3). Similarly, preterm delivery did not differ among women with self-reported PrEP exposure during pregnancy compared to those without (8.2% vs. 6.2%, respectively; aOR 1.17, 95% CI = 0.62, 2.40; P = 0.6). Among all singleton live births, there was no statistical difference detected for babies born SGA between women with and without self-reported PrEP exposure during pregnancy (9 vs. 7%, respectively; aOR for SGA vs. AGA/LGA = 1.58, 95% CI = 0.86, 3.13; P = 0.2). Composite adverse outcomes included pregnancy loss, preterm delivery, SGA or neonatal death. The overall proportion with an adverse outcome was 20% in the self-report exposed or unexposed groups (aOR = 1.07, 95% CI = 0.71, 1.63; P = 0.8) (Table 3).
Table 3 - Unadjusted and adjusted association between self-reported PrEP intake during pregnancy (confirmed only) and adverse birth outcomes between August 2019 and October 2021 (N = 1004 women with pregnancy and birth outcomes and PrEP exposure confirmation). Outcome measure Predictor (n, %) N Odds ratio (95% CI), P-value Adjusted odds ratio^ (95% CI), P-value Preterm delivery (<37 weeks)a PrEP unexposed (n = 11, 6.2%) 178 Ref Ref PrEP exposed (n = 62, 8.2%) 820 1.24 (0.67–2.54), 0.5 1.17 (0.62–2.40), 0.6 SGA (≤10th percentile)a PrEP unexposed (n = 12, 7%) 177 Ref Ref
留言 (0)