
記住我
This study is a multicenter, prospective, non-randomized controlled multicomponent study entitled “Rehabilitation including Social and Physical Activity and Education in Children and Teenagers with Cancer” (RESPECT) (Clinical Trial registration NCT01772849 and NCT01772862) and is part of the work of the Center for Integrated Rehabilitation (CIRE) [28].
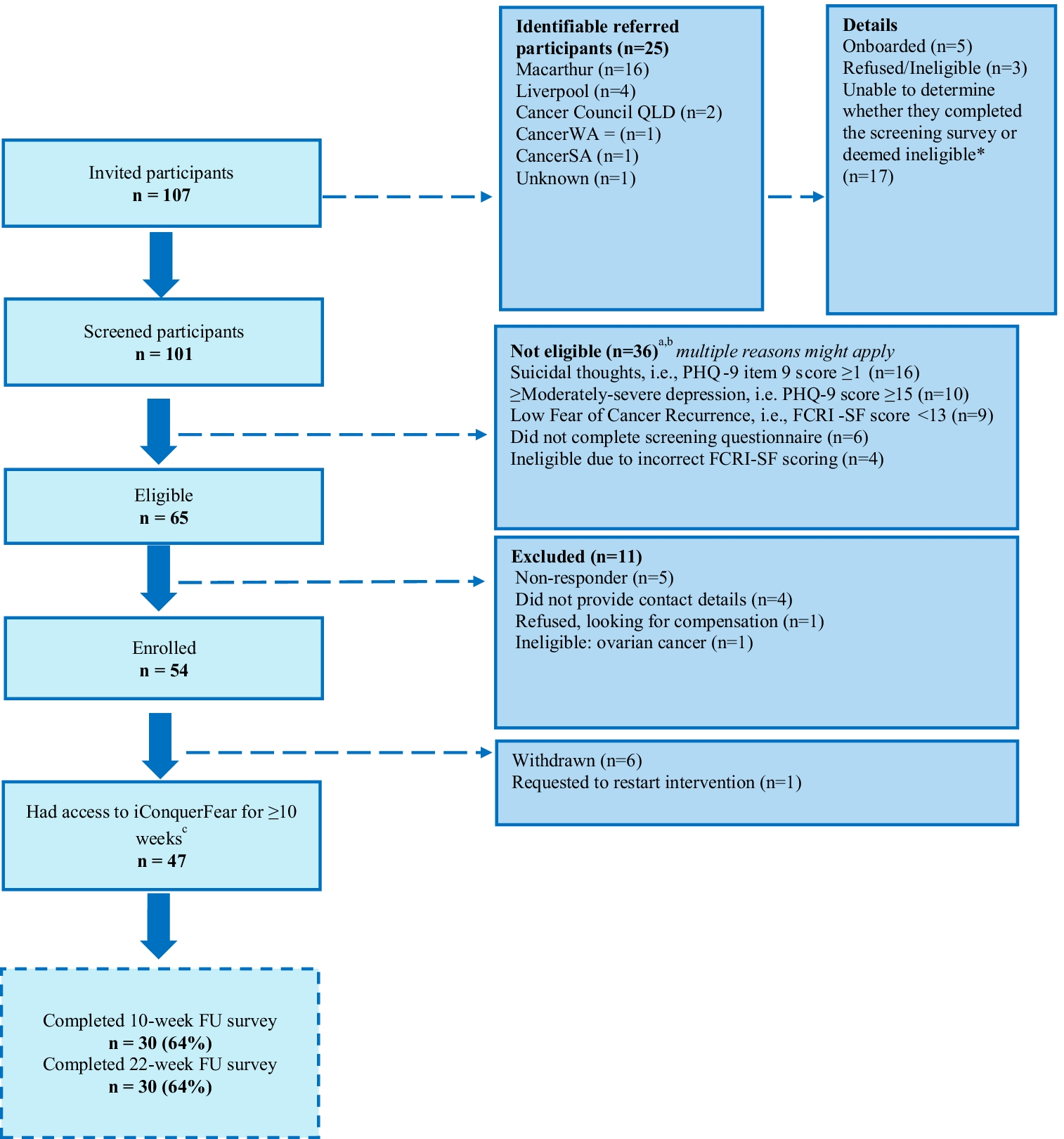
ParticipantsWe included participants during January 2013–February 2018. Inclusion criteria were age 6–18 years; any cancer diagnosis or myelodysplastic syndrome (MDS) or Langerhans cell histiocytosis (LCH); treatment with chemotherapy and/or radiation therapy; enrolled in school at diagnosis; and able to communicate in Danish. Exclusion criteria were mental disability (e.g., Down syndrome) and severe co-morbidity. We included children treated at the University Hospital of Copenhagen, Rigshospitalet, in the intervention group, and children treated at Odense University Hospital and Aarhus University Hospital in the patient control group. The patient control group received standard institutional, guided care. We excluded participants if they had experienced a recurrence of their primary diagnosis or were diagnosed with a secondary cancer. Further, we included age- and sex-matched children without a cancer history and/or chemotherapy/radiation as a community control group. The community control group consisted of a subgroup of ambassadors (n = 64) and a subgroup of participants without a history of cancer from the Acute Lymphoblastic Leukemia Survivor Toxicity and Rehabilitation (ALL-STAR) study (n = 30) assessed at the University Hospital of Copenhagen [29]. Figure 1 shows the enrollment process.
Fig. 1
Flowchart of the enrollment process and reasons for dropouts in the RESPECT (Rehabilitation including Social and Physical Activity and Education in Children and Teenagers with Cancer) study
Intervention componentsThe intervention consisted of three components. (1) We conducted a 90-min educational session for the child with cancer’s school class on cancer treatment and its side effects, everyday life at the hospital, supportive care, the benefits of physical activity, and the RESPECT study. (2) We selected two classmates as “ambassadors” in collaboration with the teachers, the classmates’ parents, and the child with cancer [30]. The ambassadors were invited to be co-admitted every 14th in- and outpatient day throughout the entire treatment period. The ambassadors were co-admitted to the hospital for the day (i.e., 9 a.m. to 3 p.m.) and were present during the daily routines at the department and participated in school, social, and physical activities. The primary role of the ambassadors was to provide peer support, maintain social inclusion, and increase the motivation of the child with cancer to engage in school and physical activities. The planning of an ambassador co-admission has been presented previously [27]. (3) We conducted an in-hospital supervised physical activity intervention (the RESPECT physical activity program) carried out during admissions to the Department of Pediatric Oncology. The RESPECT physical activity program consisted of individually designed activities (duration 5–30 min) offered three times per week (Monday, Wednesday, and Friday) and group sessions (duration 30–120 min) including all eligible children with cancer and their ambassadors on Tuesdays and Thursdays, as shown in Table 1. Daily, we designed each physical activity session to accommodate the wellbeing (e.g., presence of nausea, pain, and dizziness), training category (able to walk/not in isolation, able to walk/ in isolation, and bedbound), and physical capacity of the child with cancer (Table 1). We had not pre-defined a targeted intensity of the physical activity program before study initiation. The aim of the physical activity sessions was to mobilize the children and accomplish as high an intensity as possible on a given day. Each session started with cardiorespiratory fitness exercises spanning simple mobilization to targeted aerobic exercises (provided the child’s wellbeing permitted) followed by activities and/or games designed to improve muscle strength and balance [31]. Key equipment consisted of stationary cycle-ergometers, treadmills, dumbbells, balls, and various other items to facilitate games. We previously reported the intensity during group sessions elsewhere [6]. We measured the intensity of the individual and group physical activity program in a subgroup of CCS (n = 50) from September 2013 to September 2015. The mean heart rate was 145 beats/min [95% CI 142 to 149] or 69.3% [68.1 to 70.4%] of age-specific predicted maximal heart rate. The maximal heart rate was 185 beats/min [95% CI 174 to 184] or 89% [95% CI 87.7% to 90.4%] of age-specific predicted maximal heart rate [6]. Training frequency was calculated by dividing the number of days with physical activity by the number of weekdays admitted to the pediatric oncology department (excluding weekends and holidays).
Table 1 The in-hospital RESPECT activity programAnthropometry, body composition, and medical characteristicsWe weighed the participants to the nearest 0.1 kg and measured height to the nearest 0.1 cm. Body mass index (BMI) was calculated by dividing weight by height2.
Physical outcome evaluationThe primary outcome was VO2peak measured with the cardiopulmonary exercise test (CPET). The secondary outcomes were Sit-to-Stand, Timed Up and Go, and Handgrip Strength. We carried out the tests 1-year post-treatment ± 180 days. The treating physician permitted the tests providing the child’s thrombocyte count was > 10 billion/L, hemoglobin count was > 5 mmol/L, and the temperature was < 38°. Exclusion criteria (for testing) included active diarrhea, cough or a cold, and side effects preventing testing. We held annual meetings with all centers to ensure comparability, and we distributed instruction videos to all members of the test teams. The tests are described in detail elsewhere [22]. All children in the age- and sex-matched control group were tested at Copenhagen University Hospital, Rigshospitalet, using the same equipment as the intervention group.
Following a modified Godfrey protocol, we performed the CPET on an electronically braked cycle ergometer (Lode Corival Pediatric or Monark Ergomedic 839 E) [22, 32]. We determined breath-by-breath ventilation and gas exchange data (INNOCOR ergo-spirometry-system, INNO00010, Innovision, DK-5260 Odense, Denmark, or Jaeger Master Screen® CPX System (MS-CPX) and JLAB Software Package™). VO2peak was defined as the highest mean over 60 s and expressed in mL/kg/min. The maximal watt of the test was recorded. Heart rate and oxygen saturation were measured every 30 s (Polar FT2 sport tester Polar Electro, Kemple, Finland). Following consultation with experts on CPET testing in healthy children [33], we considered the CPET to be valid if one subjective criterion and two objective criteria were fulfilled. The subjective criteria were signs of intense effort. The objective criteria were heart rate > 180 beats/min and respiratory exchange ratio > 1.05 [33]. We stopped the test if oxygen saturation was under 90 or the child could not maintain the minimum required tempo (70 rpm).
Physical function testsThe children performed the Sit-to-Stand test [34] using a chair that allowed the child to flex the legs at a 90° angle. The child was instructed to fold his/her arms across the chest or to let them hang to the side, stand straight, and then touch the chair with their bottom while returning to a seated position. Strong verbal encouragement was given during the test. The test score equated the number of repetitions during a 30 second period.
The children performed the Timed Up and Go 3-m test [35] using a chair that allowed the child to flex the legs at a 90° angle. From the start position, with the back resting against the chair and arms on knees, we instructed the child to stand up, walk 3 m as fast as possible, turn around, and return to the start position. Completion time was recorded in seconds to the nearest two decimals. Strong verbal encouragement was given during the test. The last score of three tries was used in the analysis.
Handgrip Strength was measured using a Saehan hand dynamometer (Glanford Electronics, Scunthorpe, UK) and measured in kilograms. Two attempts per arm were performed either standing or sitting and without use of the elbow or the dynamometer touching anything. Strong verbal encouragement was given during the test and the highest score was used in the analysis [36].
Ethics approval and consent to participateAll participants and their parents gave written informed consent to participate in the educational sessions, to the inclusion of ambassadors, and to participation in the RESPECT activity program. The study was approved by the Regional Ethics Committee for the Capital Region (file. H 3-2012-105) and the Danish Data Protection Agency (file. 2007-58-0015/nr.30-0734) and complies with the Helsinki II Declaration.
Statistical methodThe power calculation is based on the primary endpoint 1-year post-treatment being VO2peak, and the power calculation is based on an anticipated 10% higher VO2peak in the intervention group compared with the control group. We based the power calculation on a pilot that found a baseline VO2peak of 24.3 (SD 5.9) [37]. The significance level 1 year after treatment end was 0.025, and the power was 0.90, resulting in 120 children in each group of children with cancer [22].
We analyzed VO2peak (mL/kg/min), VO2peak (L/min), max watt, Sit-to-Stand, Timed Up and Go, and Handgrip Strength using analysis of covariance (ANCOVA) models with the residual variance depending on the group (intervention group, patient control group, and community control group). VO2peak (L/min), Sit-to-Stand, Timed Up and Go, and Handgrip Strength were log-transformed before analyses, and the back-transformed relative effects were presented as percentage difference to the reference level. To investigate whether the impact of adjusting for the differences between the three groups could result from differences in sex, age, cancer diagnosis, and time since diagnosis, the groups were compared in three different models: (1) a raw model without any adjustments, (2) a model adjusted for the sex-dependent effects of relative age differences (10% increase in age), and (3) a model further adjusted for cancer-type-dependent effects of time since diagnosis. We categorized the types of cancers in three groups: (1) hematological cancers receiving maintenance therapy (i.e., acute lymphoblastic leukemia (ALL), acute promyelocytic leukemia, t-cell non-Hodgkin’s lymphoma); (2) other hematological cancers (i.e., Hodgkin’s lymphoma, Burkitt non-Hodgkin lymphoma, acute myeloblastic leukemia, myelodysplastic syndrome, Langerhans cell histiocytosis and children with acute lymphoblastic leukemia who were treated with hematopoietic stem cell transplantation); and (3) other oncological diseases (extracranial solid tumors and tumors located in the central nervous system).
We categorized the types of cancers in these three groups based on two previous observations. Firstly, we previously showed that children with acute lymphoblastic leukemia responded differently to physical activity than other oncological diseases (extracranial solid tumors and tumors located in the central nervous system) but not between children with extracranial solid tumors and children with tumors located in the central nervous system [38]. Secondly, we decided to account for the time since the diagnosis, as length of treatment could affect the results. In addition, we evaluated whether the difference between the three groups (intervention group, patient control group, and community control group) depended on sex or age by adding two-factor interactions as well as three-factor interactions between group, sex, and relative age difference to Model 3. The three-factor interaction was insignificant for all outcomes (all p > 0.18), and the two-factor interaction between group and sex was insignificant for all outcomes (all p > 0.20). However, for some outcomes, the differences between the groups appeared to depend on age. Therefore, estimated group differences for age 8 years and age 18 years are presented for all outcomes. We performed all analyses in R (version 3.6.0) and R-studio.
留言 (0)