
記住我

A 62-year-old Japanese man was admitted to our hospital for evaluation of renal dysfunction and skin lesions. At age 40 years, he was diagnosed with T2D. He was treated by a diabetes specialist with diet and an alpha-glucosidase inhibitor and had very good glycemic management. At age 51 years, the patient started treatment with the DPP-4 inhibitor sitagliptin. At that time, creatinine was 0.87 mg/dL, the estimated glomerular filtration rate (eGFR) was 72 mL/min/1.73 m2, and urine protein was 2+ in the qualitative test. In the subsequent 10 years, the hemoglobin A1c (HbA1c) level was maintained at 6.0–7.0%.
At age 61 years, the patient was switched from sitagliptin to vildagliptin, and one month later, widespread bullous eczema appeared. Vildagliptin was discontinued. The patient’s skin lesions were treated with conservative dermatological treatments, such as steroid ointments, and slightly improved. Four months after vildagliptin was discontinued, sitagliptin was started again. One month later, the skin rash worsened, and during the course of treatment, renal dysfunction slowly progressed. Consequently, the patient was admitted to our hospital.
On admission, the patient was 172 cm tall and weighed 80 kg. His blood pressure was 151/70 mm Hg; pulse rate, 70 beats per minute; and body temperature, 36.1 °C. Bullous lesions were present all over his skin (Fig. 1a). The bilateral lower legs were edematous. No abnormalities of the heart, lungs, or abdomen were found.
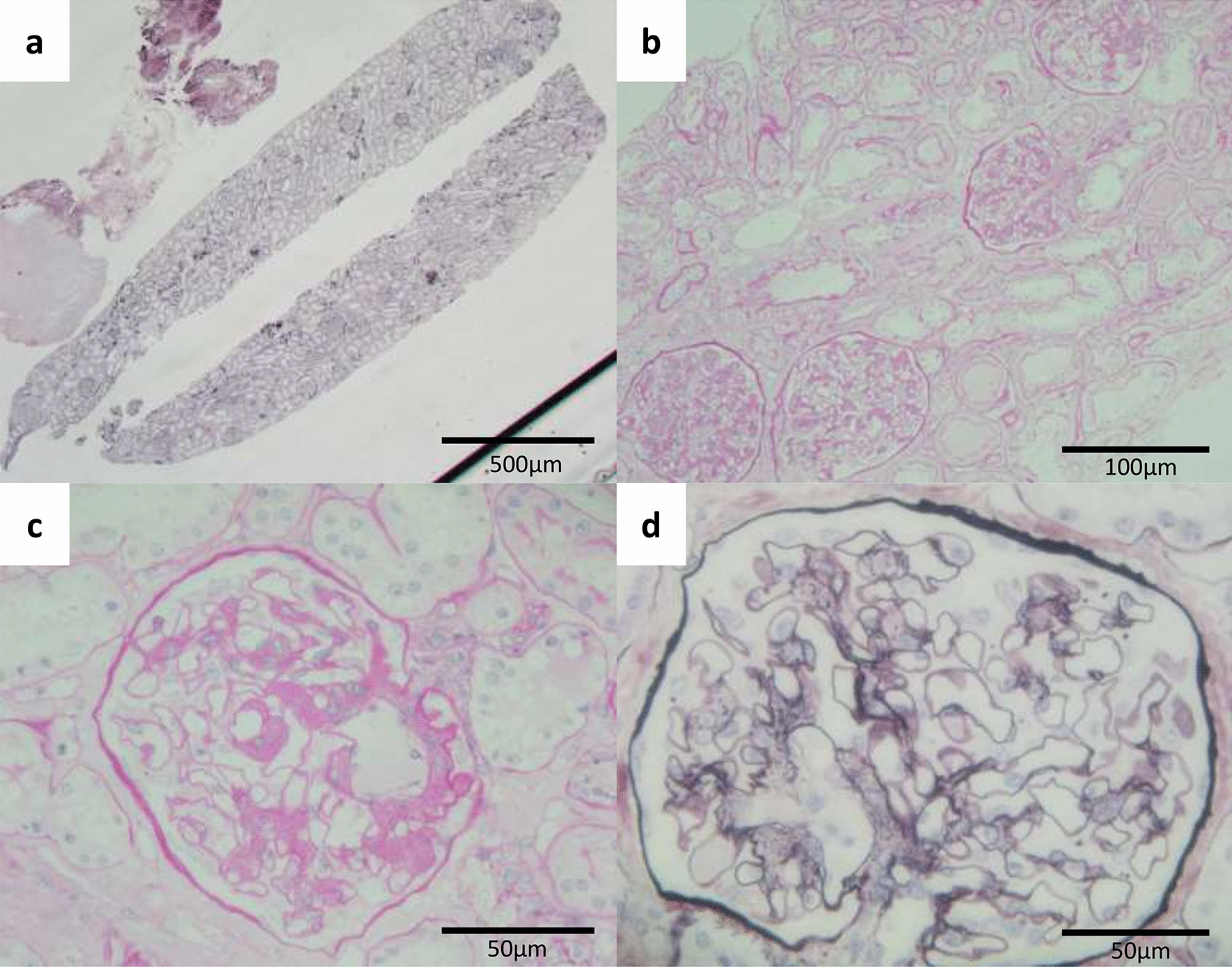
Fig. 1
Skin lesions. a Numerous bullous lesions on the lower legs. b Skin biopsy with subepidermal rip (blisters; arrow); hematoxylin–eosin stain (original magnification × 40). c Inflammatory cell infiltrate, mainly eosinophils, in the dermis; hematoxylin–eosin stain (original magnification × 200). d Linear deposition of immunoglobulin G (arrow) at the dermo-epidermal junction in immunofluorescence analysis
Laboratory findings were as follows (Table 1): leucocytes, 9100/μL; hemoglobin, 9.9 g/dL; thrombocytes, 211,000/μL; creatinine, 3.05 mg/dL; eGFR, 17.5 mL/min/1.73 m2; glucose, 222 mg/dL; HbA1c, 5.9%; triglyceride, 125 mg/dL; total cholesterol, 177 mg/dL; total complement activity (assessed as CH50), 53 U/mL (normal value, > 30 U/mL); complement 3, 74 mg/dL (reference range 86–160 mg/dL); complement 4, 26 mg/dL (reference range 17–45 mg/dL); immunoglobulin G (IgG), 1467 mg/dL (reference range 861–1747 mg/dL); rheumatoid factor, 56 U/mL (reference range < 10.0 U/mL); cyclic citrullinated peptide antibodies, 742 U/mL (reference range: < 4.5 U/mL); and anti-bullous pemphigoid 180 antibody, 5.9 U/mL (reference range: < 9 U/mL). The various other autoantibody tests, including anti-dsDNA antibody, anti-Sm antibody, anti-SS-A/Ro antibody, anti-RNP antibody, anti-desmoglein 1 antibody, and anti-desmoglein 3 antibody, were all negative. Urinary protein excretion was 4.6 g/day, and the sediment contained 1–4 erythrocytes per high-power field. The level of urinary N-acetyl-β-d-glucosaminidase was 17.3 IU/day and that of urinary β2-microglobulin, 0.7 mg/day.
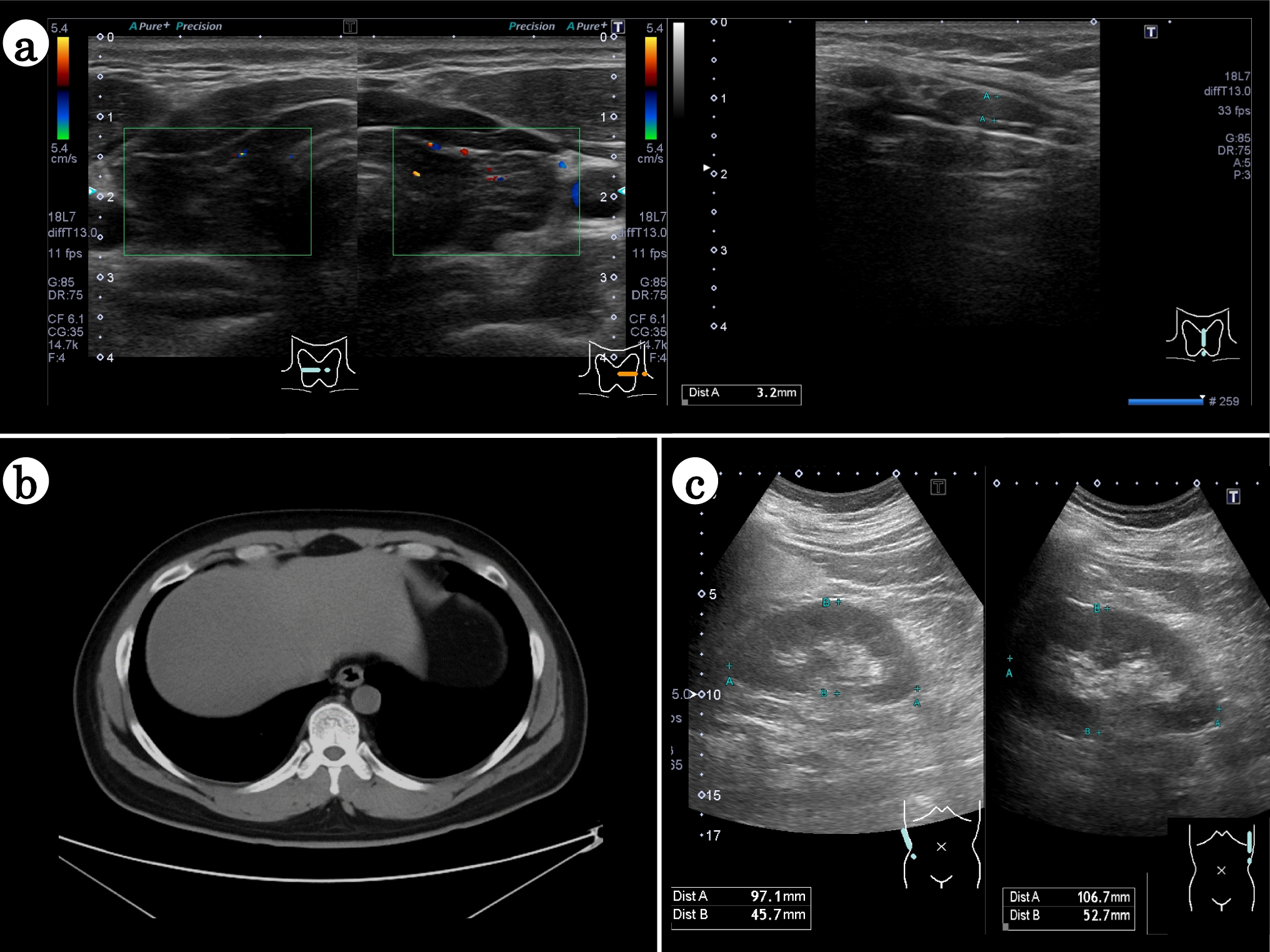
Table 1 Laboratory fndings on admissionChest X-ray showed an increased cardiothoracic ratio and left-sided pleural effusion. Computed tomography showed bilateral atrophic kidneys, with a long diameter of 84 mm.
留言 (0)