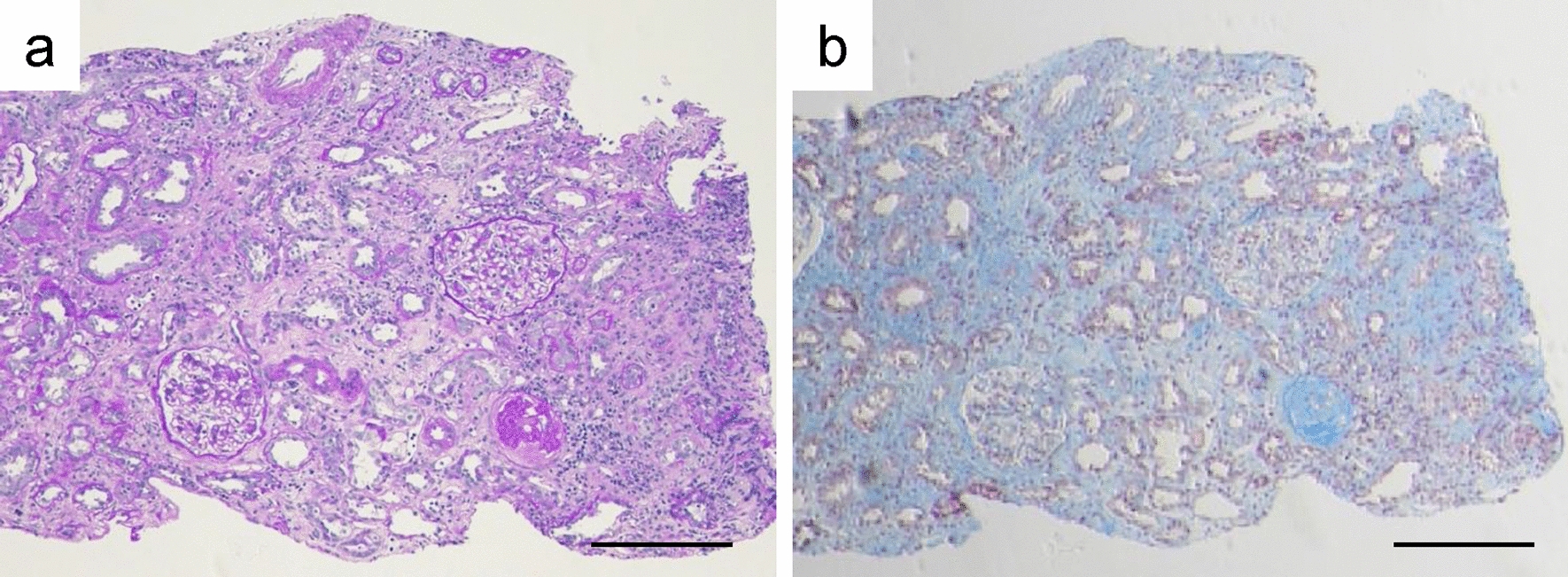
In the current case, renal biopsy was performed to investigate the patient’s renal dysfunction, despite normal urinalysis findings. Histological findings revealed minimal glomerular abnormalities; however, some glomeruli exhibited wrinkling of the GBM and collapse of the glomerulocapillary lumen, indicating ischemic changes. In addition, in contrast to the expected decrease in eGFRcreat, there was no decline in eGFRcys. Concomitant liver dysfunction, elevated creatinine kinase levels in the blood, and dyslipidemia were also observed, and further investigations revealed the presence of hypothyroidism associated with chronic thyroiditis. Treatment of the hypothyroidism improved the patient’s renal function, evaluated by eGFRcreat, and reduced the dissociation between eGFRcre and eGFRcys.
Patients with CKD are known to have a higher prevalence of thyroid dysfunction compared with the general population [11] due to factors such as decreased renal excretion of iodine [12], increased levels of inflammatory cytokines, and inhibition of thyroid hormone activation caused by oxidative stress [7]. However, the present patient’s renal function was initially within the normal range.
Although hypothyroidism is considered to be a relatively rare cause of renal dysfunction, some nephrologists recognize it as a potential pitfall. The mechanisms of renal dysfunction in hypothyroidism include nephritis, such as membranous nephropathy and IgA nephropathy, which are associated with immunological mechanisms involving the deposition of thyroid peroxidase. However, nephritis was not considered in the present case based on urinalysis and histological findings. On the other hand, reduced RPF has also been reported as a mechanism by which hypothyroidism can cause renal dysfunction, by decreasing cardiac output and direct involvement of renal hemodynamics [8]. Increased creatinine levels in hypothyroidism have previously been suggested to primarily reflect an increase in creatinine production by the muscles, independent of GFR [13]. In contrast however, recent data from humans showed no association between hypothyroidism and urinary creatinine excretion, suggesting that kidney dysfunction truly reflected a decrease in GFR [14]. Accordingly, the current patient showed no increase in urinary creatinine excretion. He also had normal cardiac function, and we therefore suspected that his renal dysfunction was mainly attributable to a reduction in RPF due to direct renal hemodynamic changes caused by thyroid dysfunction.
Although a comprehensive evaluation of the renal artery microcirculation was not feasible in the current case, the presence of renal dysfunction without abnormal urine analysis, histological ischemic finding without organic abnormalities, the absence of other evidence, and the improvement in his renal function following therapeutic intervention for hypothyroidism all supported this mechanism. We were unable to conduct this evaluation because of its excessive invasiveness and a lack of a non-experimental method for accurately evaluating renal microcirculation dynamics. To the best of our knowledge, there have been no reports of renal pathology in hypothyroidism-related renal dysfunction.
Several previous reports also support this potential mechanism. The direct renal hemodynamic effects of hypothyroidism include impaired vasodilation [15], decreased expression of vasodilators, such as vascular endothelial growth factor and insulin-like growth factor-1 [16], increased adenosine [8, 17, 18], and contraction of afferent arterioles [17] due to the tubulo-glomerular feedback mechanism. Pathologically, hypothyroidism has been reported to cause changes in glomerular structure, including thickening of the glomerular basement membrane and expansion of the mesangial matrix, leading to a decrease in RPF [19].
The dissociation of eGFRcreat and eGFRcys and its improvement after treatment for hypothyroidism also may support the involvement of hypothyroidism in the current pathology. Intracellular metabolism is suppressed in patients with hypothyroidism, leading to decreased cystatin C secretion from nucleated cells [20]. Additionally, transforming growth factor beta-1, which stimulates vascular smooth muscle cells to secrete cystatin C [21], is significantly reduced in hypothyroidism. These factors are considered to contribute to the discordance between eGFRcreat and eGFRcys in patients with hypothyroidism.
Thyroid hormones have been reported to exert their effects on thyroid hormone receptors expressed on macrophages, suppressing inflammation and contributing to the inhibition of CKD progression [22]. Furthermore, thyroid hormone replacement therapy may also improve kidney injury due to diabetes [23]. These findings suggest that thyroid hormone replacement therapy is crucial, not only for correcting hormone levels in hypothyroidism, but also for renal protection.
Hypothyroidism is known to be linked to muscle metabolism and may thus affect creatinine values [24]. However, treatment for hypothyroidism in the current patient led to improved renal function within a relatively short period of time. He was a young man and was thus unlikely to experience muscle mass loss within that time frame; furthermore, the renal biopsy findings confirmed the presence of ischemic changes.
Evaluating the microcirculation dynamics of renal arteries in general practice is challenging. To the best of our knowledge, this is the first reported case in which renal dysfunction associated with hypothyroidism-induced ischemia was evaluated through renal biopsy.
The patient was able to avoid irreversible renal dysfunction by receiving thyroid hormone replacement therapy for hypothyroidism. Organ damage, including to the kidneys, caused by changes in hemodynamics triggered by hypothyroidism can be restored through an accurate diagnosis and appropriate treatment.
To demonstrate decreased RPF, it would have been necessary to measure para-aminohippuric acid clearance. In the current case however, consideration of the mechanism of renal dysfunction occurred after confirming the histology of the kidney biopsy and after the initiation of thyroid hormone medication, thus making it unfeasible to perform this measurement. This represents the main limitation of this study.
In conclusion, we present the case of a patient in whom hypothyroidism was identified based on the dissociation between eGFRcreat and eGFRcys, and the presence of renal ischemia was confirmed through renal biopsy. Treatment for hypothyroidism improved his renal function evaluated by eGFRcreat, and reduced the dissociation between eGFRcreat and eGFRcys. This case highlights the importance of considering hypothyroidism as a potential cause of renal dysfunction, and the utility of renal biopsy for elucidating the underlying pathophysiology. The correlation between hypothyroidism and renal dysfunction is significant, emphasizing the importance of thyroid hormone replacement therapy in terms of renal protection.










Comments (0)