Tenascin-C is believed to have a significant role in the immune system and the development of inflammatory diseases. In this specific study, it was observed that the levels of serum tenascin-C were notably elevated in cases of ARF and CRHD, with statistical significance marked by a P-value of 0.04 and 0.01, respectively.
In a study parallel to ours, Golledge et al. [5]. discovered that patients with rheumatic heart disease had significantly elevated levels of serum tenascin-C when compared to control subjects (P < 0.05). This observation was further corroborated by Karatas and colleagues [11], who found a notable increase in tenascin-C levels in patients with ARF and CRHD compared to their control group (P < 0.05). They even suggested that the extent of the rise in serum TnC levels can be used as a dependable predictor for ARF.
Davutoglu et al. [12]. explored the progression of rheumatic carditis in their study, emphasizing its association with immunological and biochemical disturbances. They pointed out that the development of rheumatic heart valve disease in carditis is a complex process, influenced by genetic factors that make an individual more susceptible to autoimmune reactions [13]. The link between heart valve damage, the development of valve fibrosis, and immune-inflammatory response is well-recognized [14]. Degenerative valve lesions exhibit several characteristics typical of active pathological processes, such as chronic inflammation, lipoprotein deposition, and active calcification [15]. Moreover, the role of expressional tenascin-C in the development of fibrosis during tissue repair has also been established [14].
In this study, it was found that serum tenascin-C levels were lower in children with severe mitral valve insufficiency compared to those with mild and moderate insufficiencies, a finding that aligns with results reported by Karatas et al. Vollmer et al. [16] suggested that in the absence of tenascin-C, neutrophil invasion remains unaffected, but monocyte chemotaxis and macrophage migration are inhibited, potentially leading to insufficient tissue repair. This was supported by a study on tenascin-deficient mice, which showed less neointimal proliferation, indicating that impaired tenascin-C production could result in failed tissue repair.
Karatas et al. [11] also found in their chronic rheumatic heart disease (CRHD) group that valve replacement was performed in three patients with very low tenascin-C levels in the chronic phase. This suggests that low serum tenascin-C levels could be a useful predictor for surgical treatment. They concluded that the immune system-mediated tissue repair process is completed appropriately in rheumatic carditis in cases with normal tenascin-C levels, and that serum tenascin-C could be used to predict the disease’s prognosis.
In the present study, no significant correlation was found between serum tenascin-C and CRP, ESR, and ASOT in ARF. This is in agreement with data from Karatas et al. [11], who reported no statistically significant difference between patients with ARF in terms of serum tenascin-C and other acute phase reactants (CRP, ASOT, ESR). This suggests that serum tenascin-C is more sensitive in diagnosing ARF than other acute phase reactants.
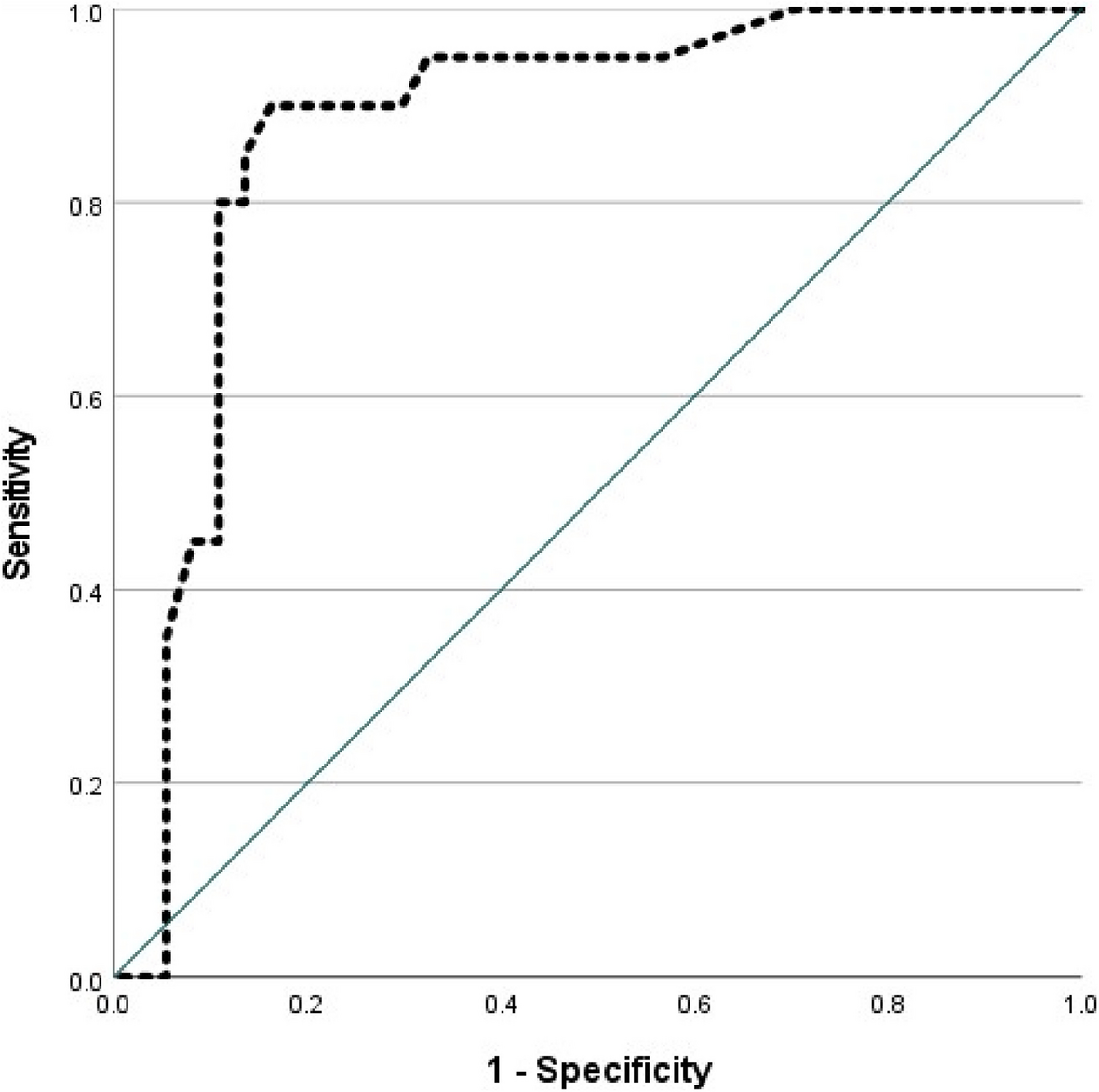
In terms of ARF, the area under the curve (AUC) in our study was 0.682 (P = 0.05) with a cutoff point of 73.76 ng/ml, a sensitivity of 75%, a specificity of 65%, a positive predictive value of 68.2%, and a negative predictive value of 72.2%. For CRHD, the AUC was 0.73 (P = 0.04) with a cutoff point of > 3.76 ng/ml, a sensitivity of 90%, a specificity of 65%, a positive predictive value of 72%, and a negative predictive value of 86.7%. These results suggest that serum tenascin-C is a very useful test for identifying ARF and CRHD.
Karatas et al. [11] reported similar findings in a study conducted on 25 patients with ARF and 25 patients with CRHD. For ARF, the ROC analysis AUC was 0.953, with a cutoff point of 2.08 ng/ml, a sensitivity of 93.3%, and a specificity of 95%. For CRHD, the AUC was 0.92 (P < 0.001) with a cutoff point of 1.56 mg/ml, a sensitivity of 83.3%, and a specificity of 85%. These findings support the use of serum tenascin-C as a new biomarker for the diagnosis of ARF and CRHD.


Comments (0)