
記住我


The adult-onset Still's disease (AOSD) is a rare, multisystem auto-inflammatory disease with four major clinical manifestations: high fever, transient rash, arthralgia, and hyperleukemia with neutrophils ≥80%.[1] The diagnosis and the accurate assessment of the disease activity for AOSD are difficult due to the absence of disease-specific clinical manifestations and biomarkers.[2,3] An early diagnosis may improve the prognosis, and there is also an urgent need for a better understanding of this complicated disease.[4] Although the etiology of AOSD is unclear, some elements of evidence have been recently reported demonstrating an increase in the formation of neutrophil extracellular traps (NETs) in AOSD patients.[5,6] The NETs, including the chromatin filaments, are one of the reticular structures released by the neutrophils in an inflammatory response due to the infection or the non-infectious factors.[7,8]
The human neutrophil lipocalin (HNL), a protein belonging to the lipocalin family, was first discovered in and purified from human neutrophils.[9–11] It is a pre-formed molecule stored in the secondary (specific) particles of the neutrophils, which can be released easily by the cells upon activation.[10] Increasing attention has been drawn to the investigation of the generation of HNL by the epithelial cells, as the generation of HNL by the renal tubular epithelial cells is triggered by a process that affects renal function.[12,13]. There are the monomeric (24,000) and heterodimeric (>90,000) molecular forms present in the neutrophils, but the molecular forms purified from neutrophils are mainly in a homodimer form with a molecular weight of 45,000 Da.[10,14]. The homodimer molecular form appears to be specific for the neutrophils, whereas only the monomeric form is generated by the epithelial cells. The differences between the antibodies against the two molecular forms have been explored to investigate whether the HNL is originated from the neutrophils or the epithelial cells.[14,15] Although HNL has been demonstrated to bind to the siderophores and there is an anti-bacterial property for HNL, the actual biological function of HNL is still unclear.[16]
As shown in the previous studies, the use of HNL to distinguish the viral infection from the bacterial infection performs well, and there is a high potential for HNL to become a clinical biomarker.[10,17,18] The elevated serum HNL was observed in a group of Sjögren's syndrome patients complicated with bronchial hyperresponsiveness.[19] Similarly, there were high HNL levels in the synovial fluid in rheumatoid arthritis (RA) patients.[20] However, HNL has rarely been evaluated in the AOSD patients who are characterized as the neutrophil activation. The purpose of this study was to explore the expression of serum HNL in the AOSD patients and to evaluate the correlation of the HNL with the clinical manifestations and the disease activity.
Methods Ethical approvalThe study was approved by the Ethical Committee of Peking University People's Hospital. All patients signed an informed written consent form.
SubjectsA total of 129 AOSD patients aged ≥18 years were recruited from 2003 to 2019, who were diagnosed according to the Yamaguchi criteria.[21] The cause of infection was confirmed for all of the patients under infection with the serological, microbiological, and/or polymerase chain reaction (PCR) methods. From these patients, the medical history, clinical manifestations, and the laboratory parameters were collected, whereas the serum samples were collected from all the study participants. The sera from 40 healthy volunteers were recruited from the blood donors to serve as controls. All of the sera were kept in a freezer maintained at −80°C.
Systemic score, demographic information, clinical manifestations, and laboratory parametersA systemic score was used for the evaluation, which was proposed by Pouchot et al[22] in 1991 and demonstrated to show a significant correlation with the mortality. One point will be assigned to each of the following manifestations, respectively, during the system score index ranking (range: 0–12): fever, evanescent rash, pharyngalgia, myalgia, abdominal pain, leukocytosis ≥15,000/mm3, lymphadenopathy, liver involvement (abnormal liver function tests or hepatomegaly), splenomegaly, pneumonia, pleuritis, and pericarditis. A standardized form was used to collect the following demographic information: gender, age, disease duration, age when diagnosed, and the previous history or family history of rheumatic disease. The clinical manifestations, including the systemic score and the arthralgia for the AOSD patients, were collected from the medical records. The hematology tests, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), serum ferritin, serum interleukin-18 (IL-18), alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactic dehydrogenase (LDH), fibrinogen (FIB), and serum levels of immunoglobulin A (IgA), IgG, IgM, complement 3 (C3), and complement 4 (C4) was done for the patients group. The serum HNL level in the AOSD patients was compared with that in the healthy controls (HCs) in the statistical analysis, where the HNL positive cutoff value was established based on the HNL results from the HCs. An analysis on the demographic information, clinical manifestations, and laboratory test results from the AOSD patients was completed for the patient group.
HNL and IL-18 concentrationsA commercial enzyme-linked immunosorbent assay (ELISA) kit (Changchun Bode Biotechnology Co., Ltd, Changchun, Jilin, China) was used to perform the serum HNL test according to the manufacturer's instructions and a sandwich ELISA (Beijing FM Bioscience Co., Ltd, Beijing, China) method was used to perform the serum IL-18 concentration test according to the manufacturer's instructions.
Statistical analysisThe statistical analysis was carried out with the Statistical Package for Social Sciences version 17.0 (SPSS, Chicago, IL, USA). The ratios and the means are shown for the descriptive data for the patients and HCs, respectively. A Student's t test or a non-parametric test was performed for the continuous data, where the frequencies were compared with the chi-squared test or Fisher's exact test as appropriate. The data in a normal distribution are expressed as a mean ± standard deviation (SD). The Pearson or Spearman's correlation test was performed to evaluate the correlation between the serum HNL and disease-related variables. The mean ± 3 SD and the receiver operating characteristic curve were used to define the grouping cutoff between different patient groups. The multivariate analysis was then used to compare variables with a P value <0.05 in the single-variable analysis. P < 0.05 will be used to ascertain the statistical significance in all of the statistical analyses, with a two-tailed test.
Results Demographic and clinical characteristics, laboratory test results, and drugs used in patients and HCsA total of 129 AOSD patients including 93 (72.1%) females and 36 (27.9%) males were enrolled in the study with a mean age of 37.2 ± 17.0 years, among whom 99 patients suffered from AOSD only, and 30 AOSD patients were under infection (17 with bacterial infection, five with viral infection, one with mycoplasma, and seven with unclassified infection). A total of 40 HCs with a mean age of 34.9 ± 9.4 years and a female/male ratio of 33/7 were recruited from the blood donors. The mean age and female/male ratio between the patients and the HCs were similar with P values of 0.485 and 0.319, respectively.
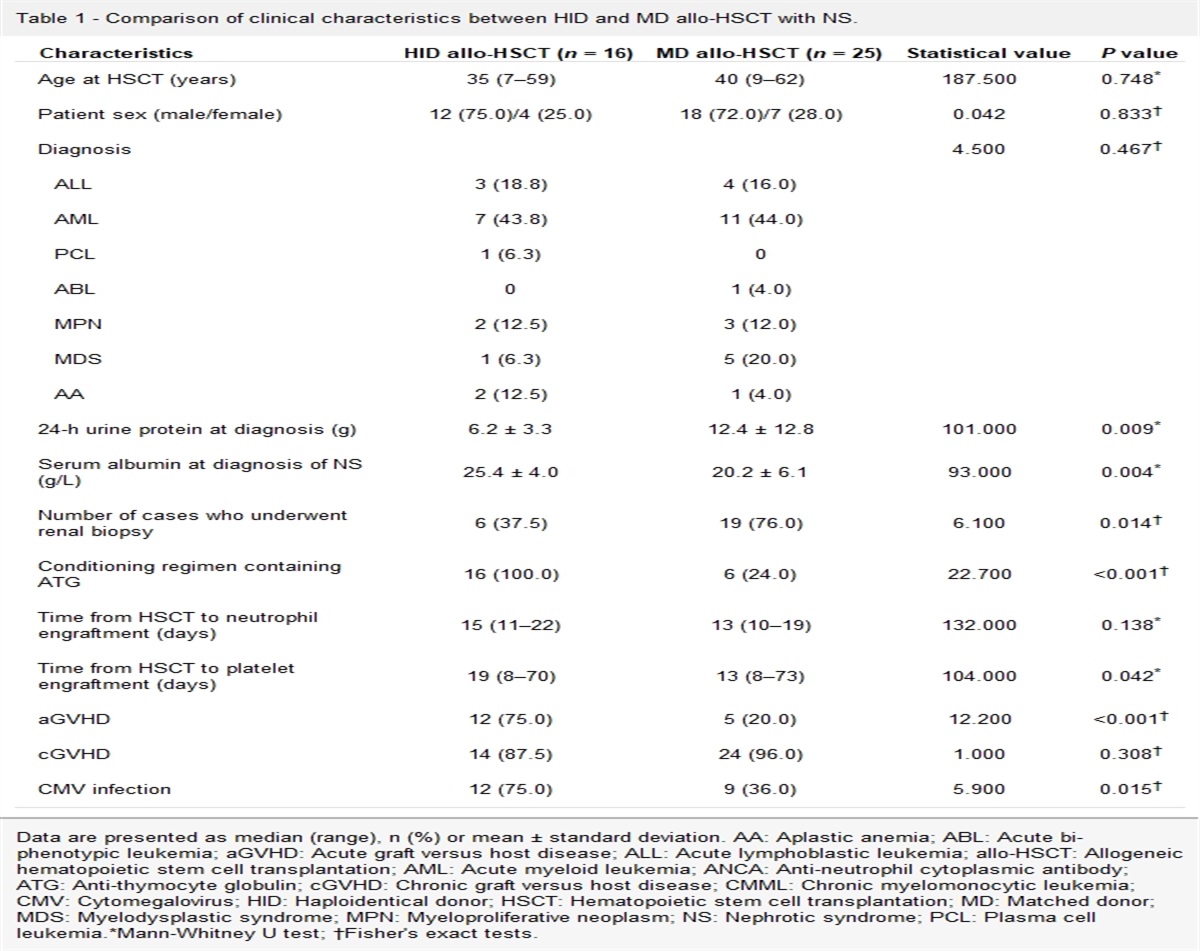
The multivariate logistic regression was used to assess the effect of age, gender, and HNL level on AOSD. As shown by the multivariate logistic regression in which the age, gender and HNL were included, the HNL levels were associated with AOSD, and the risk of AOSD was increased by 2.8% with the increase of one HNL unit (P < 0.001; 95% CI: 1.015, 1.040). The demographic and clinical characteristics and laboratory test results in patients from the two groups are demonstrated in Table 1. Drugs used in patients with AOSD only and in the AOSD patients with infection are shown in Table 2.
Table 1 - Demographic, clinical and laboratory features of AOSD patients. Characteristics AOSD without infection (n = 99) AOSD with infection (n = 30) Statistical values P values Age (years) 36.3 ± 15.9 38.2 ± 14.9 0.564∗ 0.524 Female/male 70/29 23/7 0.406† 0.863 Disease duration (years) 1.5 ± 2.0 3.2 ± 5.8 1.659∗ 0.010 Clinical data, % (n/N) Fever 42.4 (42/99) 53.3 (16/30) 1.107† 0.200 Evanescent rash 60.6 (60/99) 63.3 (19/30) 0.135† 0.714 Pleuritis 5.1 (5/99) 33.3 (10/30) 17.922† <0.001 Pneumonia 1.0 (1/99) 31.0 (9/29) 23.108† <0.001 Pericarditis 8.1 (8/99) 13.3 (4/30) 0.753† 0.386 Liver involvement 46.4 (46/99) 66.7 (20/30) 1.616† 0.204 Splenomegaly 41.4 (41/99) 46.7 (14/30) 0.260† 0.610 Lymphadenopathy 46.5 (46/99) 43.3 (13/30) 0.091† 0.763 Leukocytosis ≥15,000/mm3 32.3 (32/99) 26.7 (8/30) 0.344† 0.557 Sore throat (%) 42.4 (42/99) 50.0 (15/30) 0.536† 0.464 Myalgia (%) 23.2 (23/99) 33.3 (10/30) 1.234† 0.267 Abdominal pain (%) 2.0 (2/99) 6.7 (2/30) 1.654† 0.198 Arthritis (%) 62.6 (62/99) 53.3 (16/30) 0.832† 0.362 Laboratory findings WBC (×109/L) 12.98 ± 0.53 (n = 99) 13.07 ± 8.93 (n = 30) 0.069∗ 0.945 NE (×109/L) 9.21 (6.71, 12.97) (n = 97) 9.20 (4.81, 13.41) (n = 29) 0.580‡ 0.562 Hb (g/L) 109.41 ± 18.63 (n = 99) 103.26 ± 18.67 (n = 30) 1.584∗ 0.116 PLT (×109/L) 286.94 ± 107.82 (n = 99) 247.66 ± 109.92 (n = 30) 1.740∗ 0.084 ALT (U/L) 27.00 (13.00, 56.00) (n = 99) 37.00 (17.50, 88.75) (n = 30) 1.422‡ 0.109 AST (U/L) 32.00 (18.00, 61.00) (n = 99) 34.00 (18.75, 87.25) (n = 30) 0.817‡ 0.414 ESR (mm/1h) 64.82 ± 3.91 (n = 90) 70.42 ± 36.77 (n = 26) 0.679∗ 0.498 CRP (mg/L) 70.25 (19.18, 110.75) (n = 94) 73.85 (30.70, 129.75) (n = 28) 0.904‡ 0.366 Ferritin (ng/mL) 1792.00 (570.30, 5429.00) (n = 95) 2000.00 (646.05, 5742.75) (n = 30) 0.561‡ 0.575 IgA (g/L) 2.62 (1.80, 3.48) (n = 89) 2.28 (1.94, 3.24) (n = 27) 0.614‡ 0.539 IgG (g/L) 12.90 (10.55, 16.15) (n = 89) 13.02 (10.70, 15.30) (n = 27) 0.088‡ 0.930 IgM (g/L) 1.26 (0.88, 1.80) (n = 89) 1.04 (0.88, 1.74) (n = 27) 0.425‡ 0.671 C3 (g/L) 1.30 ± 0.34 (n = 89) 1.33 ± 0.36 (n = 27) 0.317∗ 0.752 C4 (g/L) 0.26 ± 0.07 (n = 89) 0.27 ± 0.08 (n = 27) 0.657∗ 0.512 HNL (ng/mL) 139.76 ± 8.99 (n = 99) 162.89 ± 123.66 (n = 30) 0.952∗ 0.261Data were presented as mean ± standard deviation, percentage (n/N) or median (P25, P75). ALT: Glutamic pyruvic transaminase; AOSD: Adult-onset Still's disease; AST: Glutamic oxalacetic transaminase; C3: Complement 3; C4: Complement 4; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate; FIB: Fibrinogen; Hb: Hemoglobin; HNL: Human neutrophil lipocalin; IgA: Immunoglobulin A; IgG: Immunoglobulin G; IgM: Immunoglobulin M; LDH: Lactate dehydrogenase; NE: Neutrophil; PLT: Platelet; WBC: White blood cell.
∗t values.
†χ2 values.
‡Z values.
AOSD: Adult-onset Still's disease; CTX: Cyclophosphamide; DMARD: Disease modifying antirheumatic drug; HCQ: Hydroxychloroquine; LEF: Leflunomide; MTX: Methotrexate; SASP: Salazosulfapyridine; TNF-α: Tumor necrosis factor-α.
∗One with interleukin-6 receptor antagonist and one with TNF-α receptor antagonists.
The mean serum HNL level in the AOSD-only patients (139.76 ± 8.99 ng/mL), the AOSD patients with infection (162.89 ± 123.66 ng/mL), and HCs (55.92 ± 6.12 ng/mL) are shown in Figure 1. The positive cutoff value of serum HNL was set to 74.28 ng/mL, which was defined as 3 SDs above the mean level in the HCs, based on which the positive rate of HNL in the AOSD-only patients (74/99, 74.7%) was determined to be significantly higher than that in the HCs (7/40, 17.5%; P < 0.001). The specificity and the sensitivity for the use of the serum HNL for the diagnosis of AOSD were 82.5% and 74.7%, respectively. The positive predictive value and the negative predictive value were 91.4% and 56.9%, respectively.
 Figure 1:
Figure 1: Serum concentrations of HNL in patients with AOSD only (n = 99), AOSD with infection (n = 30), and HCs (n = 40). Each dot represents an individual serum. Mean HNL levels were significantly higher in patients of AOSD only (139.76 ± 8.99 ng/mL) and in patients of AOSD with infection (162.89 ± 123.66 ng/mL) than in HC (55.92 ± 6.12 ng/mL) (t = 5.707, P < 0.001; t = 4.57, P < 0.001). The mean level of HNL in AOSD-only patients was not significantly different from that in patients of AOSD with infection. AOSD: Adult-onset Still's disease; HNL: Human neutrophil lipocalin; HCs: Healthy controls.
The serum HNL levels in the AOSD patients under the different type of the infection were compared, where the HNL level in the AOSD-only patients was significantly lower than that in the AOSD patients with bacterial infection (139.76 ± 8.99 ng/mL vs. 220.80 ± 30.59 ng/mL; P < 0.001), but was not significantly statistically different from that in the AOSD patients with viral infection (139.76 ± 8.99 ng/mL vs. 83.67 ± 37.23 ng/mL; P = 0.1731). The age, gender, HNL, CRP, and ferritin levels were included in the multivariate logistic regression to analyze the effects of AOSD with infection. The results showed that the risk of developing into the AOSD with infection will increase 1.009 times for one HNL unit increase.
Comparison of laboratory indicators and systemic score in HNL grouped AOSD patientsThe ratios of the patients with fever, leukocytosis ≥15,000/mm3, and myalgia were higher in the HNL-positive group than those in the HNL-negative group (P = 0.009, P = 0.023, and P = 0.007, respectively). But there were no significant differences shown in any of the other parameters used to assign the score for the clinical systemic score, including evanescent rash, sore throat, abdominal pain, lymphadenopathy, liver involvement, splenomegaly, pneumonia, pleuritis, and pericarditis (P > 0.05, Table 3).
Table 3 - The correlation between HNL and clinical manifestations in AOSD without infection. HNL-positive (n = 74) HNL-negative (n = 25) Clinical manifestations n % n % χ 2 P values Fever 37 50.0 5 20.0 6.885 0.009 Evanescent rash 47 63.5 12 48.0 1.868 0.172 Pleuritis 5 6.8 0 0 – 0.326∗ Pneumonia 0 0 1 4.0 – 0.253∗ Pericarditis 7 9.5 1 4.0 – 0.675∗ Liver involvement 39 52.7 14 56.0 0.082 0.775 Splenomegaly 32 43.2 9 36.0 0.404 0.525 Lymphadenopathy 35 47.3 11 44.0 0.082 0.775 Leukocytosis ≥15,000/mm3 29 39.2 3 12.0 5.133 0.023 Sore throat 34 45.9 8 32.0 1.488 0.223 Myalgia 22 29.7 1 4.0 – 0.007∗ Abdominal pain 2 2.7 0 0 – 1.000∗ Arthritis 49 66.2 12 48.0 2.622 0.105∗: Fisher exact method.AOSD: Adult-onset Still's disease; HNL: Human neutrophil lipocalin; –: Not applicable.
Whether a positive HNL result was correlated with the other serologic parameters and the systemic score in the AOSD patients was evaluated as shown in Figure 2, and the serum HNL level was significantly correlated with the white blood cell (WBC) count (r = 0.335, P < 0.001), neutrophil (NE) count (r = 0.334, P < 0.001), ESR (r = 0.241, P = 0.022), and CRP (r = 0.442, P < 0.0001), as well as the systemic score (r = 0.343, P < 0.0001). When the patients were grouped into the HNL positive and HNL negative groups, the levels of WBC ([13.95 ± 5.08] × 109/L vs. [10.12 ± 4.99] × 109/L; P = 0.001), NE ([11.24 ± 4.88] × 109/L vs. [7.22 ± 4.27] × 109/L; P < 0.001), CRP (82.80 [38.60–119.00] mg/L vs. 18.8 [7.69–72.40] mg/L; P < 0.001), and C3 (1.35 ± 0.34 g/L vs. 1.19 ± 0.29 g/L; P = 0.045) were significantly higher in the serum HNL-positive patients than in the serum HNL-negative patients. The same also applies for the systemic score in the serum HNL-positive patients (4.0 [3.0–5.0]) vs. that in the serum HNL-negative patients (3.0 [1.5–3.0]; P < 0.001). There was no significant difference shown in the blood hemoglobin, platelet, ESR, ALT, AST, LDH, FIB, IgG, IgA, IgM, C4, ferritin, and IL-18 between the two groups (P > 0.05) [Table 4].
 Figure 2:
Figure 2: The correlation between serum HNL and disease-related laboratory data and systemic score in AOSD patients (n = 99). The serum HNL level was correlated with WBC (r = 0.335, P < 0.001, n = 99), NE (r = 0.334, P < 0.001, n = 97), CRP (P = 0.442, P < 0.0001, n = 94), and ESR (r = 0.241, P = 0.022, n = 90), as well as the systemic score (r = 0.343, P < 0.0001, n = 99). AOSD: Adult-onset Still's disease; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate; HNL: Human neutrophil lipocalin; NE: Neutrophil; WBC: White blood cell.
Table 4 - Laboratory test results and systemic scores in AOSD patients. Laboratory data HNL-positive (n = 74) HNL-negative (n = 25) Statistical values P values WBC (×109/L) 13.95 ± 5.08 10.12 ± 4.99 3.270∗ 0.001 NE (×109/L) 11.24 ± 4.88 7.22 ± 4.27 3.611∗ <0.001 Hb (g/L) 109.60 ± 16.81 108.85 ± 23.63 0.148∗ 0.862 PLT (×109/L) 296.45 ± 113.19 258.79 ± 86.00 1.520∗ 0.132 ALT (U/L) 34.00 (15.30, 71.25) 32.00 (12.50, 83.50) 0.516† 0.606 AST (U/L) 32.00 (19.00, 57.25) 32.00 (16.50, 69.50) 0.064† 0.949 LDH (U/L) 312.00 (203.50, 435.00) 348.00 (254.00, 548.00) 1.135† 0.256 ESR (mm/1h) 68.55 ± 36.64 53.96 ± 37.07 1.643∗ 0.104 CRP (mg/L) 82.80 (38.60, 119.00) 18.80 (7.69, 72.40) 3.654† <0.001 Ferritin (ng/mL) 1896.00 (651.20, 5470.50) 1238.00 (245.25, 4422.00) 1.496† 0.135 IL-18 (pg/mL) 199.69 ± 42.65 196.97 ± 38.75 0.281∗ 0.779 FIB (mg/dL) 420.51 ± 149.35 427.87 ± 195.17 0.043∗ 0.886 IgA (g/L) 2.62 (1.83, 3.42) 2.71 (1.66, 4.23) 0.065† 0.948 IgG (g/L) 12.90 (10.80, 16.15) 12.75 (10.18, 16.55) 0.546† 0.585 IgM (g/L) 1.27 (0.93, 1.73) 1.07 (0.68, 2.15) 0.684† 0.494 C3 (g/L) 1.35 ± 0.34 1.19 ± 0.29 2.035∗ 0.045 C4 (g/L) 0.26 ± 0.08 0.26 ± 0.06 0.179∗ 0.858 Systemic score 4.00 (3.00, 5.00) 3.00 (1.50, 3.00) 3.946† <0.001AOSD: Adult-onset Still's disease; ALT: Glutamic pyruvic transaminase; AST: Glutamic oxalacetic transaminase; C3: Complement 3; C4: Complement 4; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate; FIB: Fibrinogen; Hb: Hemoglobin; HNL: Human neutrophil lipocalin; IgA: Immunoglobulin A; IgG: Immunoglobulin G; IgM: Immunoglobulin M; IL-18: Interleukin 18; LDH: Lactic dehydrogenase; NE: Neutrophil; PLT: Platelet; WBC: White blood cell. Data were presented as mean ± standard deviation, median (P25, P75).
∗t values.
†Z values.
The sensitivity, specificity, and predictive value of CRP and HNL in the differentiation of the AOSD patients with or without bacterial infection are shown in Table 5, where the optimal cutoff levels of CRP or HNL to differentiate the AOSD patients with or without bacterial infection are presented; based on which, there was a better performance to use HNL than to use CRP to differentiate the AOSD patients from AOSD patients with bacterial infection (Youden index 0.60 and 0.29, respectively).
Table 5 - Predictive values of HNL and CRP in the discrimination of AOSD from AOSD with bacterial infection. Predictive value (%) Items
留言 (0)