Diagnosis of tamponading pericardial effusion, in proper time, is of utmost importance, to prevent any clinical deterioration.
We tried in this study to determine if relatively new echocardiographic modalities that became readily available in most of the new machines, namely tissue Doppler imaging, can prove itself superior in the detection of cardiac tamponade. For this purpose, we benchmarked conventional and tissue Doppler-derived parameters against clinical evidence of tamponade in a small cohort of patients visiting our facility for different purposes.
Diastolic dysfunction is a recognized feature of cardiac tamponade; the underlying process for the development of tamponade is a marked reduction in diastolic filling, which results when transmural distending pressures become insufficient to overcome increased intrapericardial pressures. Tachycardia is the initial cardiac response to these changes to maintain the cardiac output [13].
Awaiting, compressive features such as right atrial collapse or right ventricular collapse might not give any advantage over clinically overt tamponade, since it means that full-blown tamponade has occurred already. The only standard echocardiographic sign of tamponade that might really point to early diastolic dysfunction is the variation in mitral inflow velocities [14], and hence the statistical significant difference encountered between the two study groups in the prevalence of variable mitral flow velocities, which was noticeably higher in patients with clinical signs of tamponade.
However, variation of mitral flow inflow velocities is largely qualitative and operator dependent.
A study by Simeonidou and colleagues concluded that variation of mitral inflow velocities continued after complete drainage of pericardial effusion and failed to correlate with signs of clinical improvement [15].
Hence, the need arose for more specific and non-operator-dependent echocardiographic signs for the detection of tamponade that are predictors of early diastolic dysfunction occurring in acute pericardial effusion.
Chalikias et al. explored the diagnostic accuracy of peak systolic tricuspid annular velocity in the detection of cardiac tamponade and proved that tissue velocity is a better marker of tamponade, and offers benefit over routine echocardiographic signs [16].
Another case report by Siniorakis and colleagues showed significant respiratory variation of tricuspid annular velocities, as an earlier sign of tamponade [17].
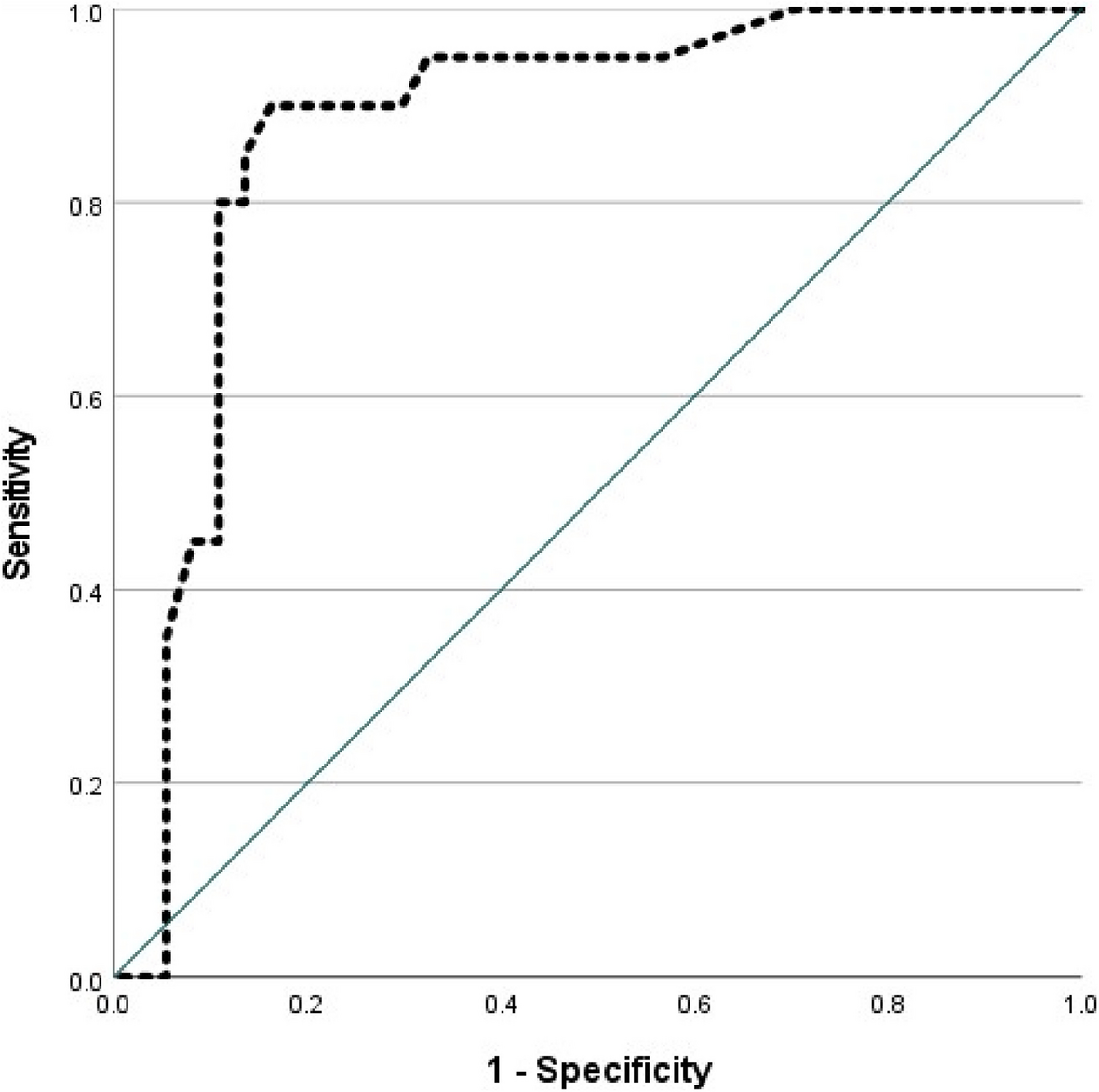
To our knowledge, this study is the first to explore the diagnostic accuracy of RV and LV E/E′ ratios in the detection of tamponade; this research showed definite superiority over conventional signs, both of them had a sensitivity of 100%, while LV diastolic dysfunction was more specific in proving effusion compared to RV, 100% vs. 93%.
This contradicts the general concept that right ventricular filling is more likely to be affected by pericardial lesions [18] and might be also linked to the underlying diagnoses of our effusion patients, notably chronic kidney disorders. The latter might be associated with LV hypertrophy, which increases the likelihood of impaired relaxation and thus can bias our data towards a higher specificity of LV indices over RV.
Coexistence of left ventricular dysfunction with pericardial effusion might delay classic signs of effusion. Elevated left atrial pressures exceed pericardial pressure and delay the appearance of pulsus paradoxus, leading to masking of tamponade. This can add an additional explanation to the findings of our study and shows how tissue Doppler imaging can be useful in early detection of tamponade in the context of impaired myocardial functions [19].


Comments (0)