
Remember me







The study aims to (1) directly compare the efficacy of maintaining ETV and switching to TDF on HCC recurrence risk and survival in patients with prolonged ETV therapy before surgery, (2) compare the safety of ETV maintenance and TDF switch after surgery through adverse event records, and (3) offer evidence and guidance for perioperative antivirus strategies in HBV-related HCC patients with prolonged ETV therapy.
Study designThis trial adopts a prospective, randomized, controlled, single-center design and is scheduled to commence at West China Hospital from May 2022 to August 2027. Figure 1 illustrates the study process.
Fig. 1
Flow chart of the study design
Trial registrationThis study was registered with chictr.org.cn (chiCTR2200057867).
Participant recruitmentFrom May 2022 to May 2024, patients with HBV-related HCC who have received long-term ETV therapy before surgery that scheduled for hepatectomy in West China Hospital will be screened for eligibility for this trial.
Inclusion criteriaThe inclusion criteria are as follows: (1) aged 18 to 70; (2) newly diagnosed with HBV-related HCC following clinical diagnosis criteria of the American Association for the Study of Liver Diseases (AASLD) [21]; (3) Barcelona Clinic Liver Cancer (BCLC) stage 0 or A, receiving curative liver resection or ablation; (4) ETV monotherapy for over 1 year with pre-surgery HBV-DNA load under 100 IU/mL; (5) Child-Pugh class A with or without cirrhosis, Eastern Cooperative Oncology Group (ECOG) performance status (PS) score ≤ 1; (6) appropriate renal function (serum creatinine < 124 mmol/L).
Exclusion criteriaThe exclusion are as follows: (1) recurrent HCC; (2) concurrent HCV, HIV, or other serious infections; (3) other malignancies or mental illness; (4) prior anti-tumor therapies pre-surgery, including portal vein ligation/embolization, radiofrequency ablation, transarterial chemoembolization, etc.; (5) participation in conflicting ongoing trials.
Participants can withdraw at any time, and poor compliance may lead to removal. Withdrawal reasons will be recorded in case report forms (CRFs), and data will be analyzed following the intention-to-treat principle [22].
Sample size calculationThe sample size calculation was performed using the software PASS (version 2015). The parameters were obtained from our previous randomized clinical trial, which evaluated the efficacy of TDF and ETV in early-stage HBV-related HCC patients after surgery. In that study, the 3-year RFS rates were 70.4% and 82.4% for patients receiving ETV and TDF, respectively. Assuming 3-year RFS rates of 70% for the control group and 85% for the treatment group, with a one-sided alpha of 0.05 and 80% power, the corresponding sample size is 190. Accounting for a 20% dropout rate, a total of 238 patients will be included in this study.
Randomization and allocationBlock randomization with a block length of four will be employed. For each block, enrolled participants will undergo 1:1 randomization into the continuing-ETV therapy group and the switch-TDF therapy group. Randomization numbers will be generated using STATA/SE 15.1 and sealed in envelopes.
InterventionParticipants will be equally randomized into two groups: the experimental group (postoperative antivirus strategies with switch-TDF therapy) and the controlled group (postoperative antivirus strategies with continuing-ETV therapy). TDF dosage is 300 mg per day, and ETV dosage is 0.5 mg per day.
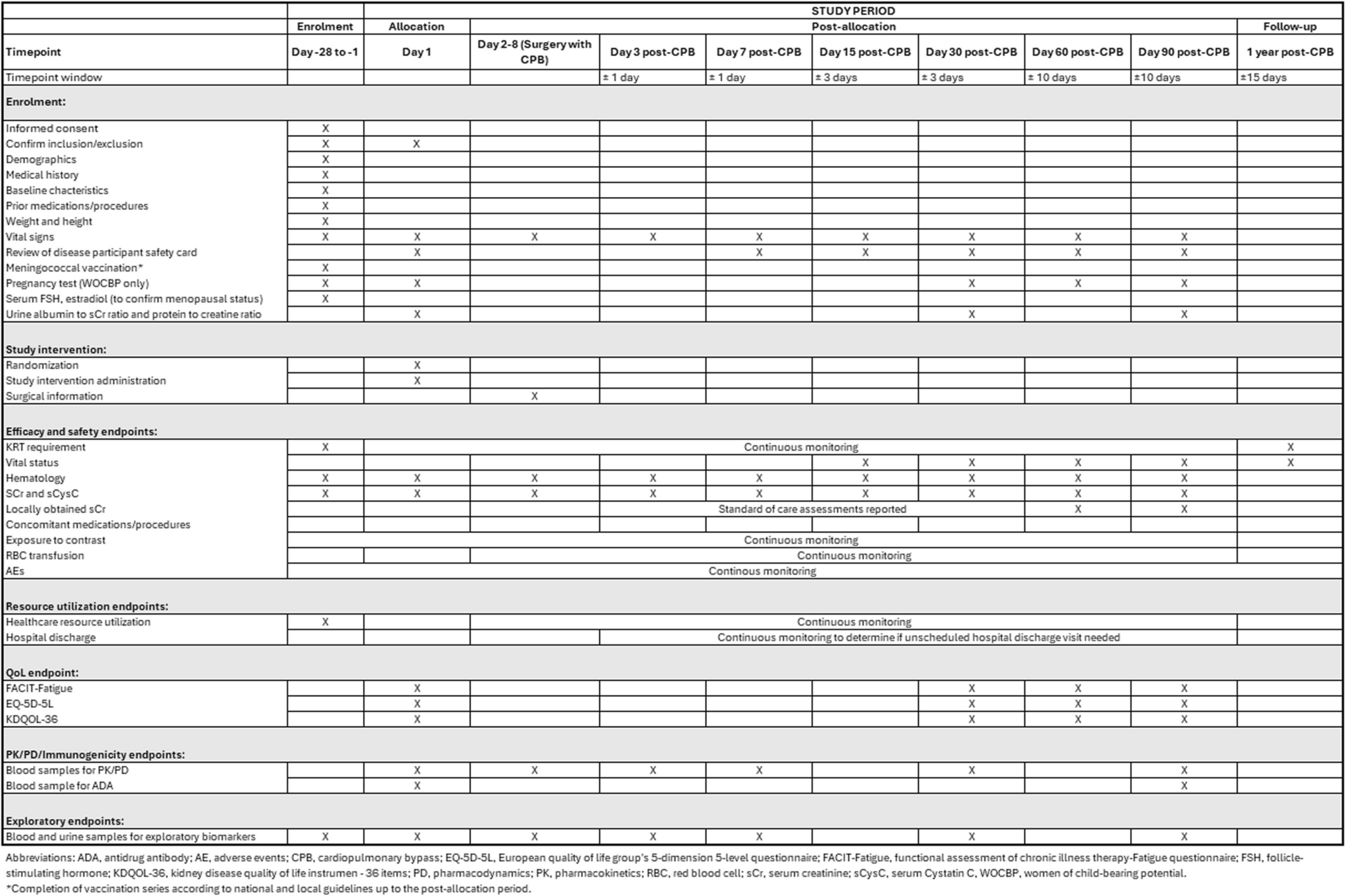
Follow-upPatient follow-up begins post-hospital discharge. Visits to the surgical team will occur every 3 months during the first 3 years post-surgery. Check-ups, including CT and/or MRI, ultrasound, routine blood tests, liver and kidney function assessments, AFP, PIVKA, and HBV DNA level measurements, will be conducted at each visit (Table 1).
Table 1 Participant timelineEndpointsThe primary endpoint is 3-year RFS, defined as the interval from the operation to the date of the first diagnosed HCC recurrence, recorded in months. The secondary endpoint is 3-year OS, defined as the interval from surgery to death or the date of the last follow-up, recorded in months.
Safety reportingBoth treatments’ safety will be evaluated through vital signs, physical exams, laboratory data, adverse events (AEs), and serious adverse events (SAEs). AEs encompass unexpected medical events or worsening conditions not necessarily linked to treatment, including hypophosphatemia, dizziness, diarrhea, nausea, vomiting, rash, fatigue, flatulence, and transaminase elevation. SAEs are events leading to death, life-threatening situations, hospitalization, deformities, birth defects, or significant permanent damages. AEs and SAEs will be documented in CRFs, with SAEs reported to ethics and administrative departments within 24 h.
Definition of the end of study is as follows: (1) participants have completed the last follow-up, (2) participants exhibit recurrence via imaging tests, and (3) participants die from any cause.
Mid-term analysisBesides final analysis, a mid-term analysis will be scheduled in the study. The purpose of mid-term analysis is about the safety and efficacy of the study. The scheduled time for mid-term analysis is set at 1 year after the last enrolled patient. If the RFS invalid hypothesis is rejected prior to final analysis, the trial might be discontinued.
Data collection and managementInvestigators and coordinators will receive specialized training for data collection. All trial-related data will be recorded on study-specific CRFs. In particular, plenty factors, including different stages of cirrhosis, would play an important role in survival of patients with HCC after surgery. Comprehensive clinical data, including Ishak score of the resected specimen, fibrosis-4 index, aminotransferase-to-platelet ratio index, and other parameters for liver cirrhosis to evaluate the baseline stage of cirrhosis, will be prospectively collected. Besides, the death from decompensation of cirrhosis, HCC recurrence, and other reasons will be precisely recorded and recognized during the follow-up since decompensation in patients with cirrhosis is a competing event from HCC recurrence. Baseline assessments will be conducted pre-randomization, and missing data will be stored until received or confirmed as unavailable. Personal information will remain confidential. Data will be entered into Excel by two independent collectors, using participant numbers for identification. Access to information will be restricted. A data manager will oversee routine accuracy checks and address any issues with the investigators. Hard copy documents will be stored securely, and electronic files will have password protection. All documents will be saved for at least 5 years post-publication, with original data available upon request to the principal investigator.
Statistical analysisBackground measures will be presented as mean ± standard deviation for continuous variables or as numbers/percentages for categorical variables. Continuous variables will be compared using a two-sided student t-test or Mann-Whitney U test, while categorical variables will undergo the chi-square test or Fisher’s exact test. Patient survival (RFS and OS) will be calculated via the Kaplan-Meier method with log-rank test. In particular, cancer-specific survival will also be calculated since decompensation serves as a competing event from HCC recurrence for death. Stage of cirrhosis, tumor burden, antiviral regimen, and other factors which may affect survival after surgery would be considered when conducting survival analysis. Generalized linear models will analyze primary and secondary endpoints. An ITT analysis, including protocol deviations, will be conducted using IBM SPSS version 26.0 software. A p-value < 0.05 indicates statistical significance.
Comments (0)