
記住我


This review was run in keeping with the PRISMA statement for systematic reviews [17]. The literature search was launched on 30 March 2023 in the PubMed and Embase databases. The keywords used were “Medtronic 780G”, “MiniMed 780G”, “advanced hybrid closed loop”, and “advanced hybrid closed loop system”. Non-English language papers were excluded. We included randomized trials, retrospective studies, observational studies and case reports regarding children, adolescents and non-pregnant young adults up to 25 years of age with T1D who were treated with the Medtronic MiniMed™ 780G in auto mode. Reviews, letters, commentaries, editorials and guidelines were excluded. The studies were taken into consideration irrespective of study setting (real-life conditions, an experimental setting, diabetes camps), duration of intervention, and baseline treatment. We decided to comment on case report papers as well because they investigate uncommon situations such as prolonged starvation or surgical procedure. These case reports may support clinicians in clinical practice.
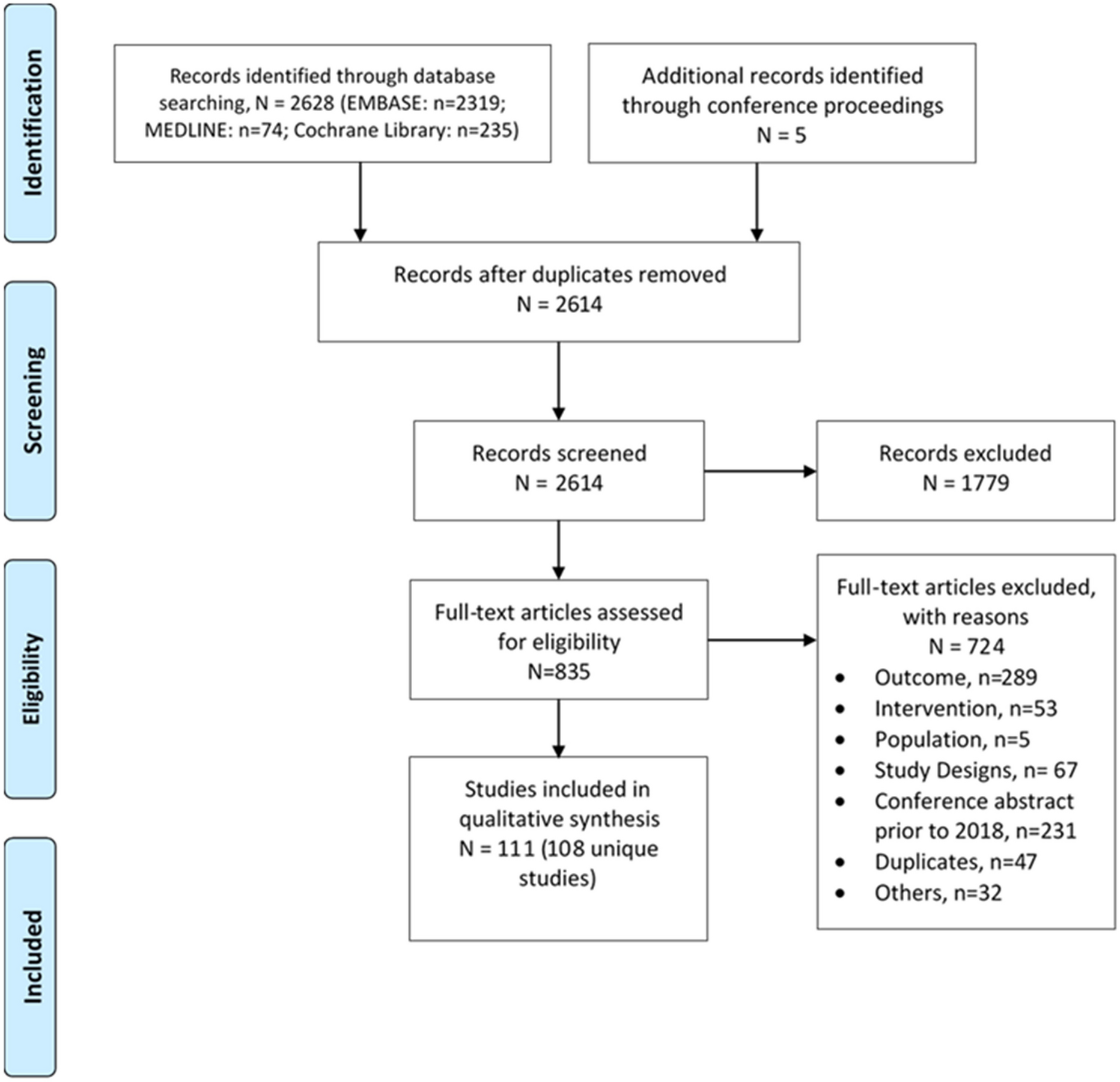
Data ExtractionFour authors (BB, SP, MM, CM) worked independently on the two different online databases. The search retrieved 783 papers. They screened all records and excluded 136 duplicates. The remaining 647 records were screened by title and abstract and 565 of them were excluded. Eighty-two full texts of potentially eligible studies were retrieved for evaluation. Disagreements between authors were resolved by discussion and consensus with the supervision of the senior authors. At the end of the selection process, 31 manuscripts were selected for this review (Fig. 1). Six of the 31 investigated psychological issues and 23 investigated metabolic outcomes. Twelve papers investigated safety issues and five papers were case reports.
Fig. 1
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
OutcomesWe retrieved data about blood glucose control, defined as glycated haemoglobin (HbA1c), and about the CGM metrics, in keeping with the International Consensus Statement [18]. In particular, we evaluated the time in range (TIR), time in tight range (TITR), time below range (TBR), time above range (TAR), mean sensor glucose (SG) level, glucose management indicator (GMI), glycaemia risk index (GRI), coefficient of variation (CV) and standard deviation of blood glucose (SD). In addition, when available, we evaluated the percentages of time spent with glucose levels between 54 and 69 mg/dL (3.0–3.9 mmol/L, level 1 hypoglycaemia) (TBR1) and below 54 mg/dL (< 3.0 mmol/L, level 2 hypoglycaemia) (TBR2) and the percentages of time spent with glucose levels between 181 and 250 mg/dL (10.1–13.9 mmol/L, level 1 hyperglycaemia) (TAR1) and above 250 mg/dL (> 13.9 mmol/L, level 2 hyperglycaemia) (TAR2). When available, CGM metrics were extracted both for 24-h and overnight periods. Fear of hypoglycaemia and sleep quality were considered as the main psychological outcomes.
Information was extracted from each manuscript and summarized as (1) the participants’ features (age, sex, diabetes duration, HbA1c before AHCL initiation); (2) inclusion and exclusion criteria in the case of clinical trials; (3) the study design, outpatient setting and follow-up duration; (4) metabolic outcomes; and (5) psychological outcomes (fear of hypoglycaemia and sleep quality).
Safety outcomes, such as diabetic ketoacidosis (DKA) and severe hypoglycaemia (SH), were considered.
Data AnalysisExtracted data were evaluated and synthesized using a narrative analysis. Evidence from qualitative studies was summarized thematically. If data were collected in cohorts with different age ranges, we only considered data about children, adolescents and young adults aged < 25 years, if clearly stated.
Studies on MiniMed™ 780G EffectivenessClinical TrialsThe effectiveness of the MiniMed™ 780G was first demonstrated by a randomized crossover clinical trial comparing an AHCL system to a sensor-augmented pump + predictive low glucose management (SAP + PLGM). Thirty-three out of 59 individuals involved in the study were children and adolescents. The authors reported that AHCL use in youth was associated with better CGM metrics. In particular, mean SG levels, overall TIR, daytime TIR, nighttime TIR, and TAR were significantly improved (p < 0.001) in the AHCL group. No between-group differences in TBR1 and TBR2 were found [19].
Nimri et al. tested the home-based feasibility of the MiniMed™ 780G in their prospective, single-arm study of 12 adolescents and young adults with T1D, which included the following phases: a first stage consisting of a 6-day open-loop run-in period with the predictive low-glucose suspend feature on; a second stage characterized by 6 days/5 nights in a supervised hotel setting while using the AHCL system; and finally, 3 weeks with unrestricted home use. HbA1c decreased from 7.1% (6.7; 7.9) to 6.8% (6.6; 7.4) (p = 0.027) and TIR increased from 68.4 ± 10.6% to 74 ± 6.1% (p = 0.06). Significant improvements occurred in nighttime TIR (64.6 ± 17.4% vs 80.7 ± 7.8%; p = 0.007) and TAR (30.7 ± 20.7% vs 16.8 ± 7.6%; p = 0.035). No significant changes in mean SG, SD and TBR were reported [20].
In a multicenter single-arm clinical trial of a large cohort of 39 adolescents, 90-day AHCL use was compared to a baseline run-in period in which SAP ± PLGM was enabled for 14 days. The study revealed that HbA1c (p < 0.001), TBR (p = 0.021), TIR (p < 0.001), TAR (p < 0.001) and TAR2 (p < 0.001) significantly improved in the adolescents. Changes in daytime and nighttime CGM metrics were similar [21].
A multinational, seven-centre, randomized crossover trial known as the FLAIR study showed that the AHCL system was also able to improve HbA1c levels (p = 0.03), TIR (p < 0.001) and TAR (p < 0.001) without increasing TBR (p = 0.42) in 113 adolescents and young adults with T1D when compared to the hybrid closed-loop (HCL) system. Both daytime and nighttime TIR were significantly higher (p < 0.001) in the AHCL arm. Additionally, the 24-h glucose profile showed that AHCL led to a consistently lower mean SG [16]. Further analyses from the FLAIR study showed that there were no differences in TIR, TITR, TAR, TBR, CV or mean SG between AHCL and HCL systems in postprandial glucose control [22] or in the impact of temporary glucose targets (i.e. 150 mg/dL) [23].
A prospective, single-arm study showed that 12 weeks of AHCL use allowed significant improvements in HbA1c, TIR, TAR, mean SG values (p < 0.001 for all) and TBR2 (p = 0.008) in adolescents who previously underwent multiple daily injection (MDI) therapy [24]. Similar findings were reported by another recent prospective, single-arm, dual-centre study on 20 youths who were previously treated with MDI but did not meet their glucose targets. All participants greatly improved their glycaemic control, as indicated by HbA1c, TIR and TAR (p < 0.001). The mean SG and CV were also lower after 3 months of AHCL therapy [25].
A recent open-label prospective Finnish study reported that the AHCL device was also effective in children with T1D who were younger than 6 years of age. Across a 12-week intervention, use of the MiniMed™ 780G system was associated with improvements in glycaemic control, as indicated by HbA1c (p = 0.01), TIR (p < 0.001), TAR (p < 0.001) and TAR2 (p = 0.001), and no negative effects on TBR or CV [26].
A prospective, open-label, two-arm study on 34 adolescents using the MiniMed™ 780G system revealed that precise and accurate carbohydrate counting resulted in a higher TIR and lower TAR2 (p = 0.043 and p = 0.012, respectively) compared with the use of three personalized fixed amounts of carbohydrate [27].
Finally, a randomized controlled trial evaluated the impact of a more aggressive system setting (glucose target 100 mg/dL and AIT 2 h) versus a less aggressive setting (glucose target 120 mg/dL and AIT 3 h) on glucose control during Ramadan fasting in adolescents and young adults with T1D. The authors demonstrated that there were no significant differences in TIR (81.0 ± 9.9% vs 82.0 ± 10.2%) and TBR (2.8 ± 0.8% vs 3.0 ± 0.3%) between the two different settings [28].
Observational StudiesMost observational studies included in this review reported the changes from a baseline run-in period of 2 or 4 weeks during which individuals used a device endowed with a PLGM function in manual mode.
An analysis of 661 MiniMed™ 780G system users younger than 15 years of age who had at least 10 days of sensor glucose data pre- and post-AHCL initiation revealed that TIR increased by 11.7% while TAR and TBR decreased by 11.6% and 0.1%, respectively. The mean SG was 16.7 mg/dL lower than baseline, and GMI also decreased by 0.4% [15].
Schiaffini et al. reported that TIR increased from 65.7 ± 16.6% to 70.5 ± 17.3% (p = 0.002) and TAR decreased from 27.2 ± 13.2% to 23.5 ± 13.9% (p = 0.05) after 4 weeks of MiniMed™ 780G system use without any changes in TBR [29].
A multicentre observational real-world study on 111 children and adolescents showed that TIR, TAR1, TAR2, GRI, mean SG, and GMI significantly improved at both 3 and 6 months of AHCL use compared with baseline (p < 0.001 for all). No differences were reported in TBR, TBR1, TBR2 or CV [30]. These findings are in line with those reported by Piccini et al. in their single-centre study, which demonstrated a significant improvement in all glycaemic outcomes except for CV and TBR, as indicated by the mean change between manual and auto modes at each follow-up time point (i.e. 14 days, 3 months and 6 months) [31]. An analysis investigating the real-world performance of the MiniMed™ 780G system in 332 users from Latin America who were younger than 15 years of age revealed the following CGM outcomes: TIR 74.2 ± 8.9%, TAR 23 ± 9.0%, TAR2 5.2 ± 4.4%, TBR 2.9 ± 2.0%, TBR2 0.6 ± 0.7%, CV 35.9 ± 5.0%, mean SG 146.5 ± 14.1 mg/dL, SD 52.9 ± 10.7 mg/dL, and GMI 6.8 ± 0.3% [32]. Another retrospective study evaluating the raw data for 4193 patient-days of 34 children using the AHCL system reported the following results for glucose control indicators: HbA1c 7.1 ± 0.9%, TIR 80.5 ± 7.8%, TAR1 14.5 ± 6.2%, TAR2 2.5 ± 2.2%, TBR1 2 ± 1.5%, TBR2 0.5 ± 0.8%, CV 33.1%, mean SG 136.7 ± 11.6 mg/dL, SD of mean glucose 45.5 mg/dL, and GMI 6.6%. No differences in the main CGM metrics were found between children older and younger than 9 years of age [33].
The successful use of the MiniMed™ 780G system has also been demonstrated when compared with conventional insulin pump therapy. Gianini et al. conducted a study on 24 children and adolescents who were using an AHCL system and had switched from a previous continuous subcutaneous insulin infusion (CSII) therapy, including insulin pumps with intermittently scanned CGM, PLGM systems and HCL devices. The authors reported significant improvements in TIR (p < 0.001), TAR (p = 0.001), TAR2 (p = 0.006), mean SG (p = 0.002) and SD (p = 0.011) 3 months after starting the new treatment. No changes in TBR and CV were described [34]. In a retrospective study, the AHCL system was compared to the first-generation AID system in a real-world setting. Despite lower baseline HbA1c levels in the MiniMed™ 780G system group [7.1% (6.8; 7.6) vs 7.7% (7.3; 8.3), p = 0.02], no significant between-group differences in CGM metrics were detected after 6 months of use [35].
A 1-year follow-up prospective study including 43 young adults aged < 25 years who were previously on conventional CSII or MDI therapy showed significant changes in TIR, TAR, TAR2, GMI, mean SG and SD after switching to the MiniMed™ 780G. TBR, TBR2 and CV did not change [36]. A retrospective study including 38 users ≤ 18 years showed that TIR increased by 22.3% and TAR1 and TBR1 decreased by 6.5% and 0.3%, respectively, after 1 year of MiniMed™ 780G system use [37].
Finally, Seget et al. reported the benefits of the AHCL system in 50 Polish children with well-controlled T1D and adolescents previously treated with low-glucose suspend (LGS)/predictive LGS (PLGS) systems. Four weeks after switching the therapy systems, TITR increased from 53.8 ± 12.4% to 61.7 ± 8.9% (p < 0.001) and TIR increased from 76.2 ± 10.3% to 81.3 ± 7.7% (p < 0.001), while TAR1 decreased from 15.6 ± 7.1% to 11.9 ± 5.5% (p < 0.001) and TAR2 decreased from 3.4 ± 3.7% to 1.9 ± 2.1% (p < 0.001). The mean SG and GMI also significantly decreased (p < 0.001 for both). More evident improvements were reported for the parameters monitored at night than for those monitored during the day [38]. Data from this study population were further analysed after 1 year. Compared with the first 2 weeks of MiniMed™ 780G system use, significant reductions in TBR1 (4.2 ± 2.7% vs 3 ± 1.8%, p < 0.05) and TBR2 (1.1 ± 1.1% vs 0.8 ± 0.8%, p < 0.05) were found. No significant differences in other glycaemic control indicators and in body mass index (BMI) z-score were observed [39].
Psychological OutcomesOnly a few studies have explored psychological outcomes in AHCL users in the paediatric and young-adult populations.
The first AHCL-associated improvement in subjective sleep quality compared with SAP + PLGM was demonstrated by Wheeler et al. [40] in subjects above 16 years of age in a randomized, two-sequence crossover study (4 weeks for each arm). The authors also reported a higher Diabetes Treatment Satisfaction Questionnaire Change (DTSQc) score in adolescents aged 13–17 years (14.8 ± 0.7 vs 12.1 ± 0.8, p = 0.024).
Higher diabetes treatment satisfaction was also found in children and adolescents aged 7–17 years upon comparing the first 12 weeks of AHCL use with previous MDI therapy [24]. Importantly, 53% of the enrolled subjects were in MDI therapy and self-monitoring blood glucose before the beginning of the study and had no previous experience with AID. The DTSQ with 12 and 14 items rated from 0 (very unsatisfied) to 6 (very satisfied) was administered to children/adolescents and their parents respectively. Average score increased from 3.6 ± 0.6 to 4.6 ± 0.8 (p = 0.001) in youths and similar results were found for their parents, with an average DTSQ score of 3.5 ± 0.6 at baseline and 4.8 ± 0.9 at the end of the study (p = 0.001). In a longer study, Gianini et al. [34] showed that the AHCL system decreased the fear of hypoglycaemia (from 60.5 ± 17.0 to 49.4 ± 3.5, p < 0.001) and the diabetes-related emotional distress (from 19.3 ± 12.3 to 8.6 ± 8.3, p = 0.001), thereby increasing the well-being perception (from 68.2 ± 16.8 to 80.5 ± 14.2, p = 0.03), in 24 users aged 10–18 years after 4 months of use. These findings were obtained regardless of HbA1c value (< 7% or ≥ 7%) at the beginning of the study: both subgroups showed a statistically significant improvement in the quantitative scores. Only the well-being score showed a nonsignificant improvement in the HbA1c ≥ 7% subgroup. A negative correlation between diabetes-related emotional distress and well-being was found in subjects with HbA1c ≥ 7%; instead, diabetes-related emotional distress was correlated with fear of hypoglycaemia in the HbA1c < 7% subgroup. In addition to the quantitative results, qualitative assessment, achieved through interviews, also demonstrated an increased quality of life with AHCL usage, as it reduced the exhaustion related to disease management and stress due to dysglycaemia while increasing sleep quality, with both children/adolescents with T1D and their parents expressing their satisfaction.
AHCL was also associated with a reduction in parental diabetes distress in very young children’s parents [26], as evaluated by the Problem Areas in Diabetes Scale-Parents Revised (PAID-PR) score, which decreased from 37.5 (18.2) to 27.5 (14.8) (p = 0.006) after 12 weeks of use. Interestingly, the score did not correlate with markers of glycaemic control, total daily dose (TDD) of insulin, age or diabetes duration (p = 0.22–0.91) at the beginning of the study, and no significant correlations were found between the PAID-PR score and glycaemic markers or TDD (p = 0.15–0.80) at 12 weeks either.
A randomized, two-period (12 weeks in each arm), crossover trial comparing AHCL versus HCL use revealed significant improvements in glucose monitoring satisfaction subscale scores for emotional and behavioural burdens (p < 0.01) with the use of AHCL in a cohort of 113 adolescents and young adults [41]. A further correlation analysis of glycaemic outcomes (TAR, TBR2 and percentage of time spent in auto mode) with satisfaction measures demonstrated that satisfaction increased as less time was spent in hyper- or hypoglycaemia. More time in the auto mode [86%, interquartile range (IQR) 77–91 vs. 75%, IQR 64–83%, in Medtronic 780G vs 670G, respectively] was associated with greater glucose satisfaction [16].
留言 (0)