
記住我
The mean age of participants was approximately 28 years at enrollment. Most had completed primary level education (60%), and 55% lived in informal housing (i.e., not regulated by the state in terms of building codes or safety regulations and/or no legally identified owner or address). The majority of our participants were married and living with their partners with 25 and 35% of participants’ partners having additional wives/partners in the intervention and control groups respectively (see Table 1).
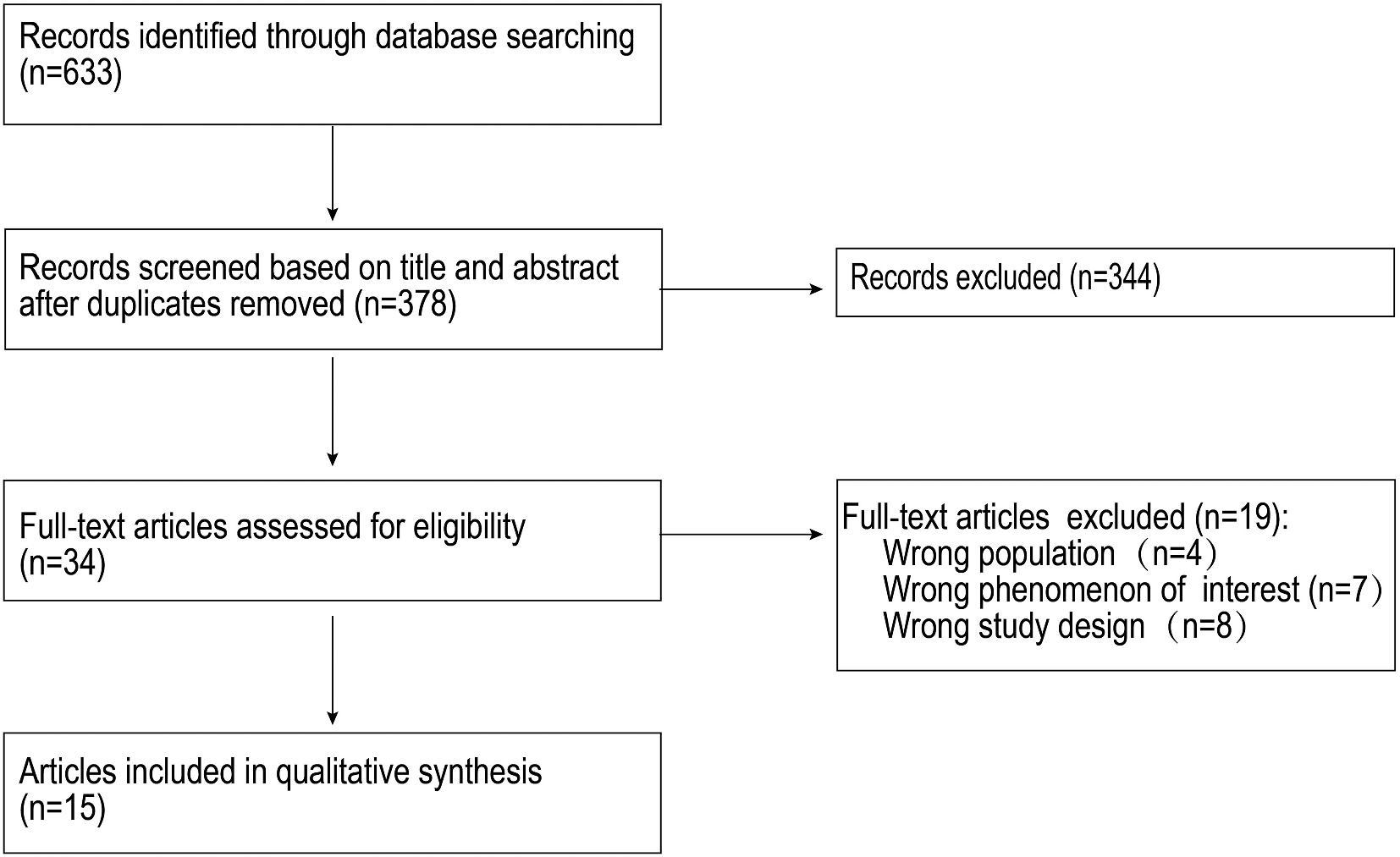
Table 1 Baseline characteristicsAssociations between the intervention and food security and depressive symptomsFood insecurity decreased during the study period with median scores of 11.5 and 2.0 for the intervention group compared to 12.0 and 9.0 for the control group at baseline and 6 months postpartum, respectively (see Table 2). There was a significantly greater reduction in food insecurity scores from baseline observed in the intervention group when compared to the control group at 6 weeks and 6 months postpartum (p = 0.0008 and p < 0.0001, respectively, Table 2). More than half of participants in each group were severely food insecure at baseline, but by 6 months postpartum, three (15%) women in the intervention group compared to 10 (50%) women in the control group were severely food insecure (see Table 2, see also Fig. 2 for categorized HFIAS scores across time).
Table 2 Measured scores and linear mixed modelFig. 2
HFIAS scores by categories of food security
Median PHQ-9 scores for the intervention group decreased from 8.5 at baseline to 3.0 at 6 months postpartum, and in the control group median scores decreased from 6.5 to 5.0 between baseline and 6 months postpartum. The overall decrease in PHQ-9 scores for both groups was significant at 6 weeks and 6 months postpartum (p < 0.0001 and p = 0.029, respectively) but there was no significant difference in decrease between groups (see Table 2, see also Fig. 3 for categorized PHQ-9 scores across time).
Fig. 3
PHQ-9 scores by categories of depressive symptom severity
Mean PSS scores decreased (indicating decreased stress) across the intervention period. For the intervention group, scores decrease from 17.9 at baseline to 12.6 at 6 months postpartum and for the control group scores decreased from 15.8 to 15.1 between baseline and 6 months (there was no statistically significant decrease or difference between groups, see Table 2).
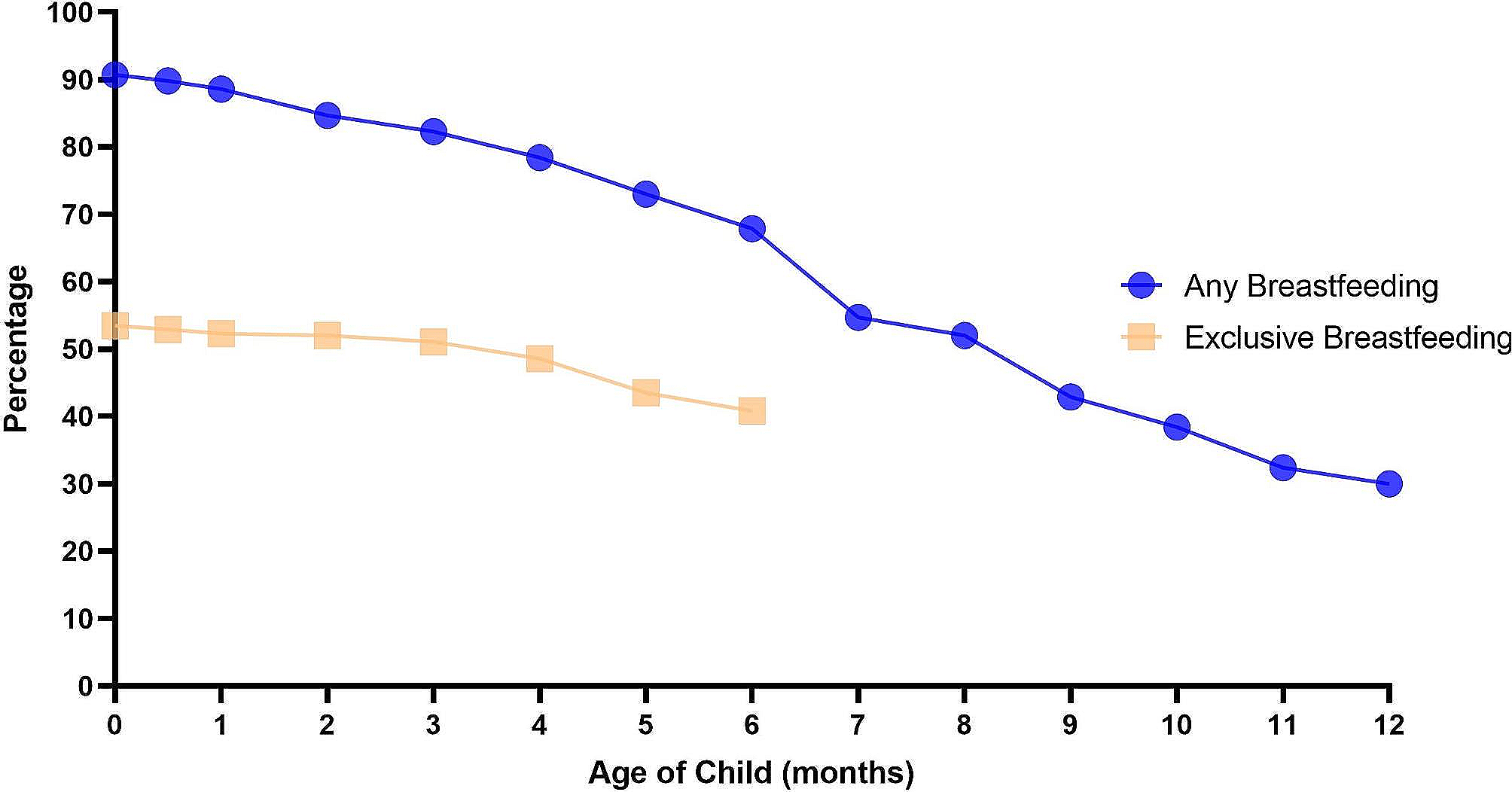
Breastfeeding behaviorsMost women in both groups planned to exclusively breastfeed at baseline, but around a quarter of women overall either did not believe they would produce enough breastmilk or were unsure. Follow-up surveys revealed that all women in the intervention group consistently reported feeding their babies “breastmilk only” while three (15%) women in the control group reported already giving their baby water at 2 weeks postpartum. In terms of perceived milk insufficiency, most women in both groups reported they were producing enough milk to satisfy their baby from 2 to 12 weeks postpartum. However, when asked if anything could help them to produce more breastmilk, most women in the control group answered, “yes, more food”, whereas nearly all women in the intervention group answered “no” (i.e., they were not lacking anything needed to support breastmilk production). At around 6 months postpartum, most women in the intervention group reported introducing complementary foods or had plans to begin doing so at 6 months postpartum or shortly thereafter. Meanwhile, less than half of the women in the control group reported introducing complementary feeding at 6 months postpartum with at least three women introducing earlier than recommended and nine women planning to wait until their baby was 7-months-old (see Table 3).
Table 3 Baseline and follow-up questions about breastfeeding behaviorsExit interview findings 1.How was the unconditional cash transfer used?
Above all and without exception, women used the money to purchase food and water. In addition to these basic needs, most women also reported buying clothes, baby items, or other household items such as mattresses for sleeping or pots for cooking. Using the money for rent, school fees, medical bills, or for transportation to the clinic was also mentioned by most. More than a quarter of women used part of the funds to revive or start-up small businesses, and around the same number of women allocated money to support the needs of their close family members or church. Women also paid off debts and/or saved some of the money.
2.What happened when financial insecurity was reduced for women?
“It has changed my life” is how most participants described their experience with Supporting Healthy Mothers. Women explained, the money transfers had spared them from desperate circumstances such as needing to beg for money or food. Financial insecurity had been a primary stressor for women—straining relationships and leaving at least two women feeling so hopeless they had thoughts of ending their life.
PID 18- It would have been bad [without the money]. I do not think this marriage would have survived…Because (sighs) you cannot be staying together, and the children are not going to school and you are just there and you know you also need food. The children also need food, they need clothes to put on, it would have been very tough, it would have been a tough life…(Sighs).
According to participants, the funds provided instant relief from overwhelming worries, through increased food security, improved relationships and better options for caring for their infants and other children. Women explained that this relief brought them joy, happiness and hopefulness.
PID 20: It relieved me from the stress I had in my heart. I can see the progress I have made, and it has helped me in so many ways.
Several women, also mentioned using the funds to support their engagement in HIV care.
PID 20: Yes. I am currently experiencing a lot of changes even when my VL [viral load] test is done, the levels are going down, my weight is good.
The unconditional cash transfers also decreased women’s dependence on others and increased their ability to provide for their family, which together with the relief from stress led women to feel empowered, strong, motivated and courageous.
PID 04- I just felt totally empowered. It has motivated me with my baby because you know when you lack, and you have a baby, sometimes you can be angry, you can react…overreact, but as of now, I was living a comfortable life.
Naturally, women sought ways to sustain this financial security/ independence. Nearly all women were planning to engage in income generating activities or were already working by the time of the exit interview including eight of nine women who, at baseline, reported having no occupation or independent source of income even prior to pregnancy.
PID 06- I used to work in a kiosk, I have a kiosk. I used to buy soap, detergent, sugar. It collapsed, and when I began receiving this money, I began saving bit by bit, I was not using it all. I would save little by little… I began stocking…Currently I have everything, I am selling charcoal, kerosene and the likes. I have developed with the help of this money, it has helped me by the way, yes.
Most relationships between women and their partners improved during the study period. Over half of the women told their partners about the money either because they felt disclosure was unavoidable or because they wanted to tell. In contrast, many did not disclose or withheld details such as the amount being received or the number of payments because they feared their partners would stop providing or try to take control of the money. Among women who reported a lack of support or problems with partners during the intervention, all reported the problems were preexisting and/or unrelated to the money and no women reported being worse off in their relationship. Regardless of whether or not women told their partners about the money, relationships improved for most in various ways. Some women reported feeling closer to their partners as they collaborated to decide about how to spend the money.
PID 15- Yes, very much. We became close, we could tell stories, we could do stuff together and he could even laugh whenever we were talking.
For others, having the money made them feel more respected or valued by their partners.
PID 18- He does not speak rudely to me because he knows I am everything. If a child was in need of anything, he can send the child to ask me for it because he knows I have it.
Women also reported improved infant feeding experiences related to the unconditional cash transfers. For example, several women noted that improved food security facilitated adequate breastmilk production.
PID 11- The intervention? Giving us that money helped us. I would go and buy food with that money because I know the baby had to breastfeed. So, I had to eat the food so that I can have plenty of milk for the baby to breastfeed and get satisfied.
Other women noted the money allowed them (stress free) time to stay home from work, breastfeed and care for their baby or that it allowed them to purchase adequate complementary foods.
PID 02- Since you started funding me, I have not been outside my door, I have not been leaving. So, people are like, (mentions her own name) stays at home, how has she been paying her rent? How does she feed when she is just home? You see, the stress of rent and how I feed is gone.
When asked how they felt about the money transfers ending, most women described feeling positive, prepared or grateful. That said, some believed a bit more time supported by the money would put them in a better position to sustain themselves as their baby would be older and/or their business more established and income more stable. Others wished the money transfers would be extended to sustain optimal infant care—continued breastfeeding, optimal complementary feeding and more time with their baby before starting back to work.
PID 13- [explaining why the money should continue for another year] R: Okay, sometimes someone has not organized himself/herself, how I was eating the balanced diet will reduce and the way to feed the baby good food as recommended can also reduce. Sometimes it will reduce, and she will be unable to access the food well, and she will not be able to get sufficient milk, so I do not know.
3.What practical skills and knowledge were gained from the infant feeding support sessions that women could apply?
The majority of women were able to accurately recall what they learned about breastfeeding technique, including many technical skills such as how to position their baby, how to achieve an effective latch, how and why to burp their baby, how to understand whether or not their baby was getting enough milk and the importance of feeding on demand and giving their attention to their baby while breastfeeding. Most women also recalled key knowledge including the primary factors that impact milk production and the concepts of foremilk and hindmilk. Understanding foremilk and hindmilk provided women with a rationale for breastfeeding duration and frequency and for alternating between breasts. In addition, women explained that watery foremilk was evidence that their babies did not need water in addition to breastmilk (a commonly held belief among women locally) [43, 44].
PID 09- the more the baby breastfeeds, the more milk is produced…. It signals the brain to produce milk when there is none, and the more you breastfeed, the more milk is produced. I felt that was true, because when I was breastfeeding her, despite how hungry I felt, more milk would still be produced whenever I breastfeed her.
Women also credited the lactation specialist with teaching them about the many benefits of breastfeeding and specifically exclusively breastfeeding for the first 6 months.
PID 07 - I had thought that I would wean her at 2 months because considering that I was going to leave her with someone else while I go to work. When I received the information, I continued breastfeeding her and I did not wean her until 6 months.
Finally, nearly all women gained important (and new) information about complementary feeding including the types of food to give, how to prepare baby’s food and the consistency and quantity of food their baby needs at each stage.
PID 10 - Actually before the lessons, before lessons, I didn’t know how to feed the baby. After giving me that balanced diet, that chart, yes, I know what to give and what not to give.
4.What was the perceived impact of the infant feeding support sessions?
Women reported that the information and support given in the sessions about breastfeeding and their baby’s progress as well as the opportunity to talk about their concerns reduced their worries and made them feel more happy, confident, informed and capable.
PID 11- You see, I normally have stress and I do not talk about it but whenever I come here, I tell you about my issues, I pour them out to you, I leave you with that burden…when I leave here, I am okay, I do not even remember those things (Laughter). But when I keep them to myself, they eat me up, it becomes a problem, and even eating is a problem because the stress affects me everywhere.
A major concern the lactation specialist addressed for women was worry about mother to child transmission of HIV.
PID 13- All along I was worried that I would infect the baby with HIV, so the information gave me courage and made me know that…it removed my worries that I previously had. It removed the worries that I had and made me courageous, and I just breastfed my baby until he was 6-months-old.
The information, support, reassurance and encouragement women received was also critical to helping women resist social/cultural pressures that impede optimal infant feeding and health, including “plastic teeth” removal (a practice that involves a traditional provider cutting an infant’s gums or actually extracting the infant’s primary tooth buds while claiming to have removed “plastic teeth” that are allegedly plaguing the infant) [45, 46].
PID 12- No, since you had told me about it [referring to plastic teeth removal], I am now an expert on them, I am an expert, I can tell someone else not to take the baby to the metal place [to the traditional healer who “removes plastic teeth”].
Seeing their infants’ weight at the beginning of each session was additional reassurance for women that their baby was getting enough breastmilk and many women noted that this increased their confidence and contentment with their baby’s progress.
PID 04- According to me, it was about weight gain, it made me so happy. I was happy with it because every month I went, I could see him grow, change, and gain weight and I became confident, and I was also happy.
For some participants, knowledge gained through the sessions led to improved complementary feeding practices, such as not forcefully feeding the baby.
PID 18- The information I got from the lactation specialist helped me big time, because with the other children, the older ones, I would begin forcefully feeding them porridge once they were 6-months-old. The lactation specialist informed us that we should not forcefully feed the baby, so I do not forcefully feed my last baby, I did not force him.
Notably, several women were experiencing challenges with complementary feeding (baby not taking food or spitting up porridge) at the time of the exit interview and wished for continued support.
5.Was the intervention acceptable to women?
All women reported that the intervention was good just the way it was delivered, reporting that it helped, it changed their life, that there was nothing negative and/or that they felt supported. All women thought the intervention should continue helping women and/ or be expanded to reach other women (who are suffering).
With regards to the infant feeding support sessions: Most women were happy with the length and timing of the sessions, though a few would have liked to meet with the lactation specialist immediately after birth and some women wished for the sessions to continue until they were done breastfeeding or until they had overcome the challenges of complementary feeding. Women liked that the sessions were private/ personalized, that the lactation specialist and research coordinator held their baby, that refreshments were given, that they were free to call with concerns and that much more than the standard information and support were provided (i.e., much more in comparison to the PMTCT clinic).
With regards to the money transfers: More than half said, the money was a major help but that they needed more to meet all the basic needs of their house, with most saying 15–20,000KES ($110-145USD) would have been enough. Just less than half said the money was sufficient or more than sufficient for all basic needs. Most were happy with payments being delivered monthly and some specifically noted they appreciated that the money was given: without conditions, on time, at the beginning of the month and/or via M-PESA. M-PESA proved particularly effective and secure. Even in the two cases when women lost access to their phones, they were able to recover their funds, since the money is delivered to a specific registered phone number, and not connected to a physical phone or sim card. In terms of being socially acceptable, most women did not tell anyone except for their partner about the money, and no one disclosed to more than one or two close friends/ relatives. Women did not discuss the money with others for a variety of reasons. Some felt being associated with such an intervention would reveal their HIV status, others thought people might think the money came from “evil” and some preferred not to tell simply because they believed others would ask them to share the money. Several family members who heard about the unconditional cash transfers were indeed suspicious about the source of the funds but eventually accepted or came to understand that the money came from a benign source. Overall, disclosing or not disclosing information about the money received was not problematic for women. In fact, we screened women at every visit, asking “Was there any negative thing you experienced as a result of receiving this money?” and all women at every visit responded, “no”.
留言 (0)