
Remember me







This study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments and was approved by the ethics committee of Hirosaki University (reference number: 2017-026 and 2019-009). All included participants provided informed consent.
All participants of the Iwaki Health Promotion Project, a community-based preventive medicine programme that aims to improve average life expectancy by conducting general health examinations and prophylactic interventions, were included in this study as previously described [15, 16]. In the 2017 and 2019 projects, a total of 1902 volunteers participated. Data of those who participated in both the 2017 and 2019 projects were analysed using the 2017 data. Since the EKOA prevalence is higher in women than in men [17], this study focussed on female participants with no radiographic abnormalities. In total, 1000 participants were excluded for the following reasons: male sex (n = 867), radiographic abnormalities [Kellgren–Lawrence (KL) grade ≥ 2, n = 115], rheumatoid arthritis (n = 9), no radiograph (n = 1), incomplete data (n = 1), or a history of knee injury (n = 7). Female participants without radiographic abnormalities were randomly selected for MRI. A total of 359 participants were included in the final analysis (Fig. 1), and their mean age was 51.3 ± 11.7 years (range 22–85 years) (Table 1).
Fig. 1
Flowchart illustrating the selection of participants. The participants included in or excluded from the current study are shown. Values in parentheses indicate the number of participants excluded. KLG Kellgren–Lawrence grade, KOA knee osteoarthritis
Table 1 Luyten’s classification criteria proposal for early knee OA [18]Questionnaires were administered to investigate lifestyle habits such as habitual drinking, smoking and exercise frequency. Height and weight were measured and body mass index (BMI) was calculated during anthropometric evaluation.
Radiographic evaluations and bone mineral densityPlain knee radiographs were obtained using the CXDI-40EG digital radiography system (Canon Inc., Tokyo, Japan). Orthopaedic surgeons with over 10 years of experience in radiographic examinations obtained full-extension, weight-bearing and anteroposterior radiographs of both knees with foot map positioning on the day of examination. Sequencing was set at 60 kV, 50 mA and 80 ms for all participants. KL grade ≥ 2 in the most affected knee was defined as knee OA. Two orthopaedic surgeons graded all the joints. Discrepancies were resolved through mutual consultation. Bone mineral density (BMD) at one-third of the distal radius of the nondominant hand was measured on the same day by dual-energy X-ray absorptiometry using the DCS-600EXV bone densitometer (Hitachi Aloka Medical, Tokyo, Japan).
Classification criteria for EKOAParticipants without knee OA findings on plain radiography were classified into the EKOA group if they met the Luyten’s classification criteria [18] described below; others were classified into the non-EKOA group (Table 1).
(a) Patient-based questionnaires including the availability of the Knee Injury and Osteoarthritis Outcome Score [19], with at least two of the following required to score positive (i.e. ≤ 85%): pain, symptoms, activities of daily living (short version) and knee-related quality of life.
(b) Clinical examination required the presence of at least one of the following: joint line tenderness or knee crepitus.
(c) Radiographs with KL grades of 0 or 1 in the standing and weight-bearing positions.
Measurements of the proximal tibial morphology using MRIMRI was performed within 1 week of the other examinations. The right knees were examined using MRI with a rapid extremity coil and a mobile magnetic resonance unit (1.5 T) (ECHELON RX, Hitachi, Tokyo, Japan). MRI was performed in the supine position with fully extended knee. Sequences included sagittal and coronal T2-weighted fat-saturated fast spin-echo (repetition time, 5000 ms; echo time, 80 ms; field of view, 16 cm; 288 × 288 matrices; and slice thickness of 3 mm with a 1.0 mm gap between slices).
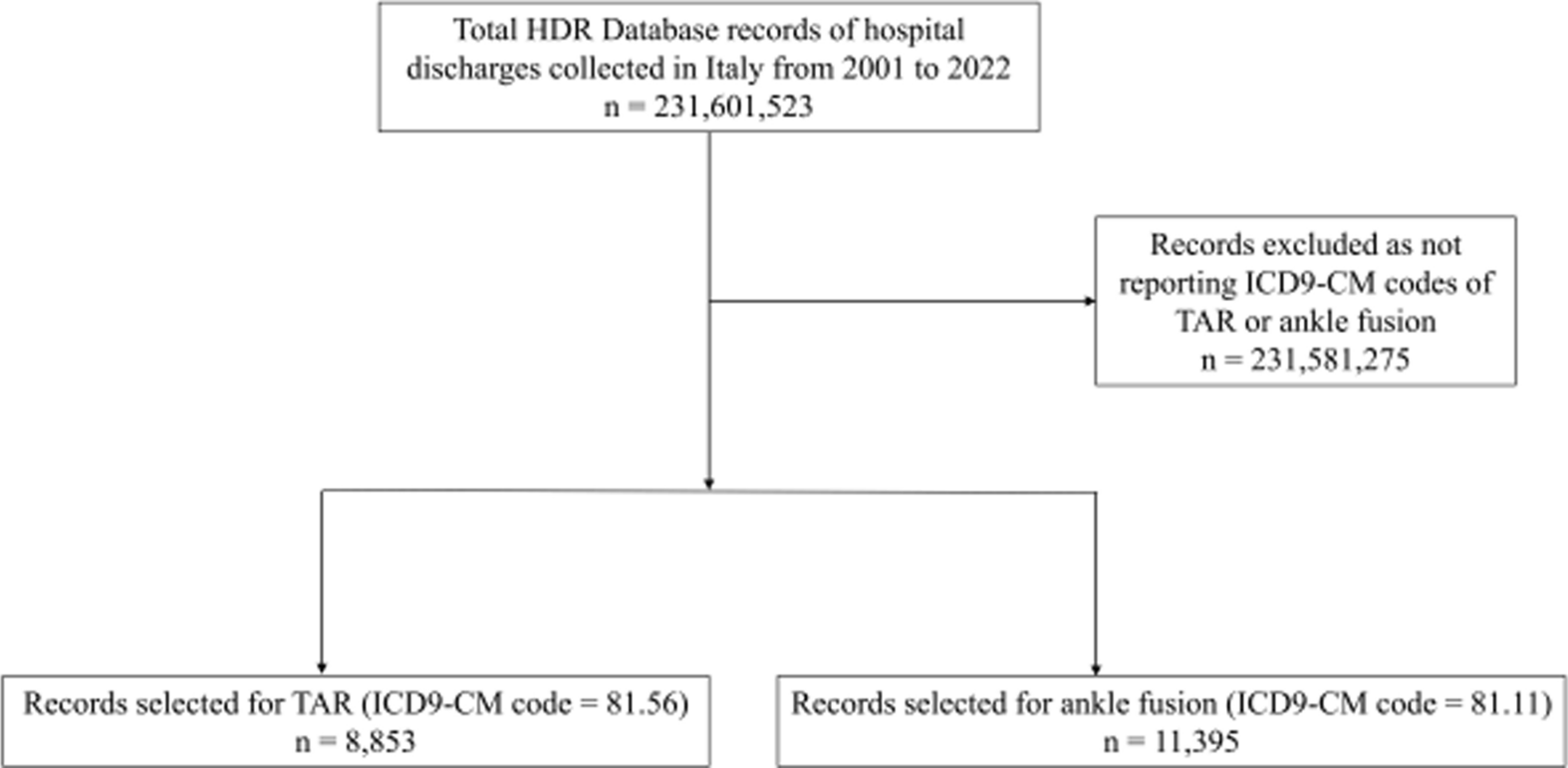
For the MPTA measurement, a slice was selected that showed the tibial anatomy and medial and lateral menisci in the coronal view of MRI [20]. It was then determined as the angle between the tibial anatomic axis and knee joint line (Fig. 2a). The medial and lateral PTSs were measured as described previously [21]. First, the central sagittal plane was determined on the slice based on the attachment of the posterior cruciate ligament and intercondylar eminence. Within this slice, two circles fitting the anterior and posterior cortices were placed on the tibia. The line connecting the centres of these two circles was used as the tibial axis (Fig. 2b). The medial and lateral PTSs (MPTS and LPTS) were determined as the angle between the axis perpendicular to the tibial axis and the line connecting the two most proximal anterior and posterior subchondral bone points at the centre of the lateral and medial tibiofemoral compartments, respectively (Fig. 2c, d).
Fig. 2
Measurements of the proximal tibial morphological parameters on magnetic resonance images. The MPTA is measured as the angle between the anatomical axis of the tibia and proximal tibial joint line in the coronal view of the MRI image (a). The central sagittal plane is determined on the slice based on the attachment of the posterior cruciate ligament and intercondylar eminence. In this slice, two circles fitting the anterior and posterior cortices were placed on the tibia. The line connecting the centres of the two circles was used as the tibial axis (b). The MPTS and LPTS are determined by the angle between the axis perpendicular to the tibial axis and the line connecting the two most proximal anterior and posterior subchondral bone points at the centre of the lateral and medial tibiofemoral compartments, respectively (c, d). MPTA medial proximal tibial angle, MRI magnetic resonance imaging, MPTS medial posterior tibial slope, LPTS lateral posterior tibial slope
Two independent observers examined the interrater reliability of 40 randomly selected images.
Pathological lesions on MRIPathological lesions on the knee joint MRIs were blindly evaluated by two independent observers based on the Whole-Organ MRI Score (WORMS) [22]. Based on the WORMS, synovitis, cartilage damage, BMLs, subchondral cysts, bone attrition, osteophytes and meniscal lesions were evaluated. Synovitis was graded collectively from 0 to 3 on the basis of the estimated maximal distention of the synovial cavity. Regarding cartilage damage, BMLs, subchondral cysts, bone attritions, osteophytes and the number of subregions with scores > 0 were calculated. The meniscal lesions were calculated as the maximum meniscal damage grade of the entire knee. The intra- and inter-rater reliabilities, expressed as interclass correlation coefficients (ICC) (1,1) and (2,1), were 0.929 and 0.921, respectively.
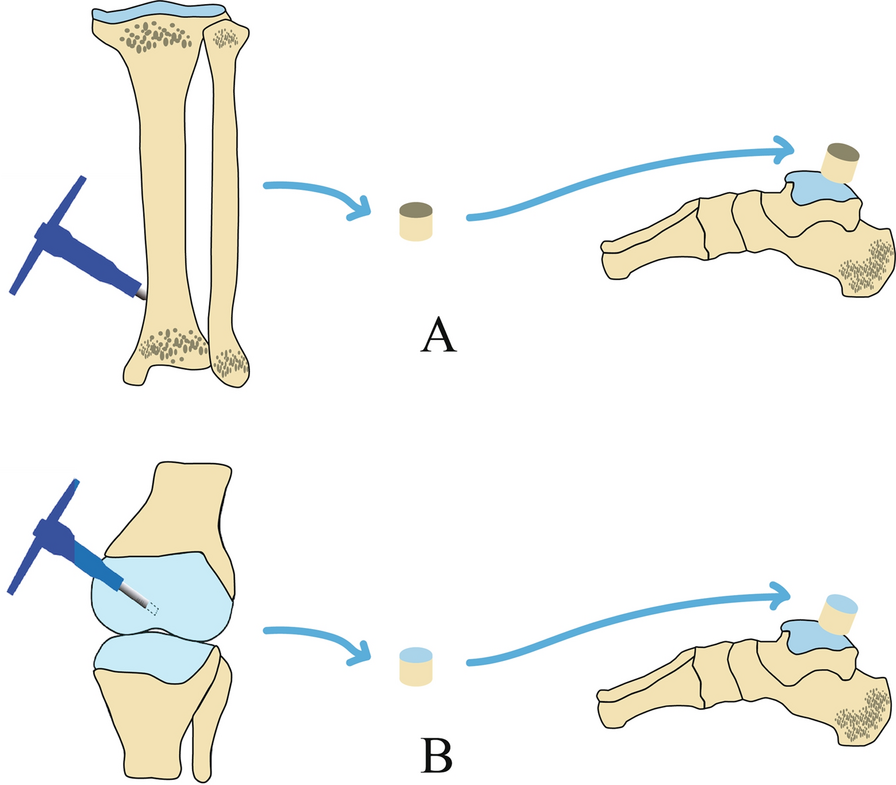
In addition to the WORMS evaluation, SRS was diagnosed as a BML spreading out like roots from the attachment of the medial meniscus posterior root on the coronal plane of the MRI images [14] (Fig. 3).
Fig. 3
Representative magnetic resonance image showing spreading root sign. Representative SRS images in the coronal plane are shown. High signal intensity is observed in the subchondral bone lesion along with the attachment of the medial meniscus posterior root on T2-weighted fat saturation fast spin-echo images. The white arrow indicates SRS. SRS spreading root sign
Statistical analysisDemographic data and proximal tibial morphological parameters in each group are expressed as mean ± standard deviation. The Mann–Whitney U and chi-squared tests were performed to compare the two groups because some demographic parameters were not normally distributed by the Shapiro–Wilk test. Proximal tibial morphologies among age groups (< 40, 40–49, 50–59 and ≥ 60 years) were compared using analysis of variance and Tukey’s test. Correlations among the proximal tibial morphologies were evaluated by Spearman’s rank correlation.
Logistic regression analysis was performed with the presence of BMLs as the dependent variable and age, BMI, BMD, lifestyle habits, presence of pathological lesions of cartilage, attrition, meniscal lesions, effusion, MPTA, MPTS and LPTS as independent variables in the non-OA and EKOA groups. These regression models were adjusted for lifestyle habits, including smoking, drinking and fitness. Additionally, to evaluate the associations between proximal tibial morphologies and SRS, logistic regression analysis was performed. SRS was defined as the dependent variable, whereas age, BMI and proximal tibial morphological parameters were defined as the independent variables. To estimate the predictive cut-off level of proximal tibial morphologies for detecting SRS, receiver operating characteristic (ROC) analysis was performed with the MPTA, MPTS and LPTS values as variables. The false-positive fraction was plotted against one true-positive fraction, and the point with the largest slope (closest to the true positive) was the cut-off point. To assess the validity of ROC analysis, the area under the curve (AUC) was calculated. Data inputs and analyses were performed using SPSS version 29.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p value < 0.05.
Comments (0)