
記住我
Excessive femoral version is a condition that can have a notable effect on one's quality of life.1,2 Knee pain, gait abnormalities, and cosmetic concerns are some of the key indications for a femoral derotational osteotomy.3 Notably, if femoral version abnormalities are left untreated, excessive femoral anteversion4,5 or retroversion6 have been suggested to lead to the development of hip arthritis. Consequently, surgical approaches and techniques have been developed to ameliorate symptomatic femoral version abnormalities7,8 and improve pain levels, gait, and overall alignment of the lower extremities in affected patients. However, there is no clear consensus among orthopaedic surgeons regarding indications for surgical intervention to address femoral version abnormalities.9,10
One important factor to consider regarding indications for femoral derotational osteotomy is patient quality of life. Heath et al11 described the importance of patients' perceived quality of life as a necessary factor when planning for lower limb deformity surgery. Indeed, capturing the patient-centered experience through patient-reported outcome measure (PROM) surveys can help surgeons provide more patient-focused and higher-quality care.12 To this end, Heath et al11 demonstrated that patients presenting with a limb deformity (limb-length discrepancy, angular deformity, or combined limb-length discrepancy with an angular deformity) scored markedly worse on preoperative survey scores compared with healthy control subjects. However, differences in PROM survey responses between patients with femoral version abnormalities and healthy control subjects have not yet been established.
The primary goal of this study was to determine the quality-of-life deficit using the Limb Deformity–Modified Scoliosis Research Society (LD-SRS)13 and the Patient-Reported Outcomes Measurement Information System (PROMIS)14 questionnaires for patients with symptomatic femoral version abnormalities compared with asymptomatic healthy control subjects.
Methods Patient SelectionAfter Institutional Review Board approval, a retrospective review of a prospectively maintained surgical database at a single institution was conducted. This surgical log search identified all patients older than 18 years scheduled for unilateral or bilateral femoral derotational osteotomies with intramedullary nail fixation for correction of femoral version abnormalities that completed a preoperative survey series, including the LD-SRS and PROMIS surveys. This study sought to assess patients' preoperative quality of life only compared with asymptomatic control subjects and thus no postoperative outcomes were reported. Patients were excluded if they were younger than 18 years, did not complete the LD-SRS and PROMIS surveys, or version abnormality was not a primary patient report. Patients indicated for concurrent lengthening or angular corrections were excluded. Patients indicated for concomitant correction of tibial malrotation were included. Patients indicated for concomitant arthroscopy of hip or knee joint were also included. This yielded 21 patients between December 2018 and September 2022. A comparison cohort was created by using the LD-SRS and PROMIS scores from 33 skeletally mature, asymptomatic volunteers with no reports of version abnormality. These individuals were previously sampled in 2021 and did not have a physical or radiographic examination. Owing to the research volunteer limitations mandated during the coronavirus pandemic, these volunteers were identified through convenience sampling and thus the authors were limited in their ability to match the version and demographics of the symptomatic and control cohorts.
Patient-Reported OutcomesFollowing the methodology of Heath et al,11 all participants completed the LD-SRS and PROMIS questionnaires. The LD-SRS is a reliable and previously validated survey, adapted from the Scoliosis Research Society (SRS) questionnaire, specifically used to measure the quality of life in patients with nonarthritic, lower extremity deformity.13 It includes four subscores (Function/Activity, Pain, Mental Health, and Self-Image/Appearance) and a total score, which is an average of the other four domains. Each subscore is measured on a Likert-rating scale of 1 to 5, with higher scores indicating higher quality of life (eg, a high LD-SRS Pain subscore specifies lower pain levels). The PROMIS questionnaire is a validated but more generalized PROM survey with subscores normalized to a mean of 50 with a standard deviation of 10. Higher scores are indicative of more of the domain being measured (eg, a high PROMIS Pain Interference subscore specifies more pain interference with daily life).15
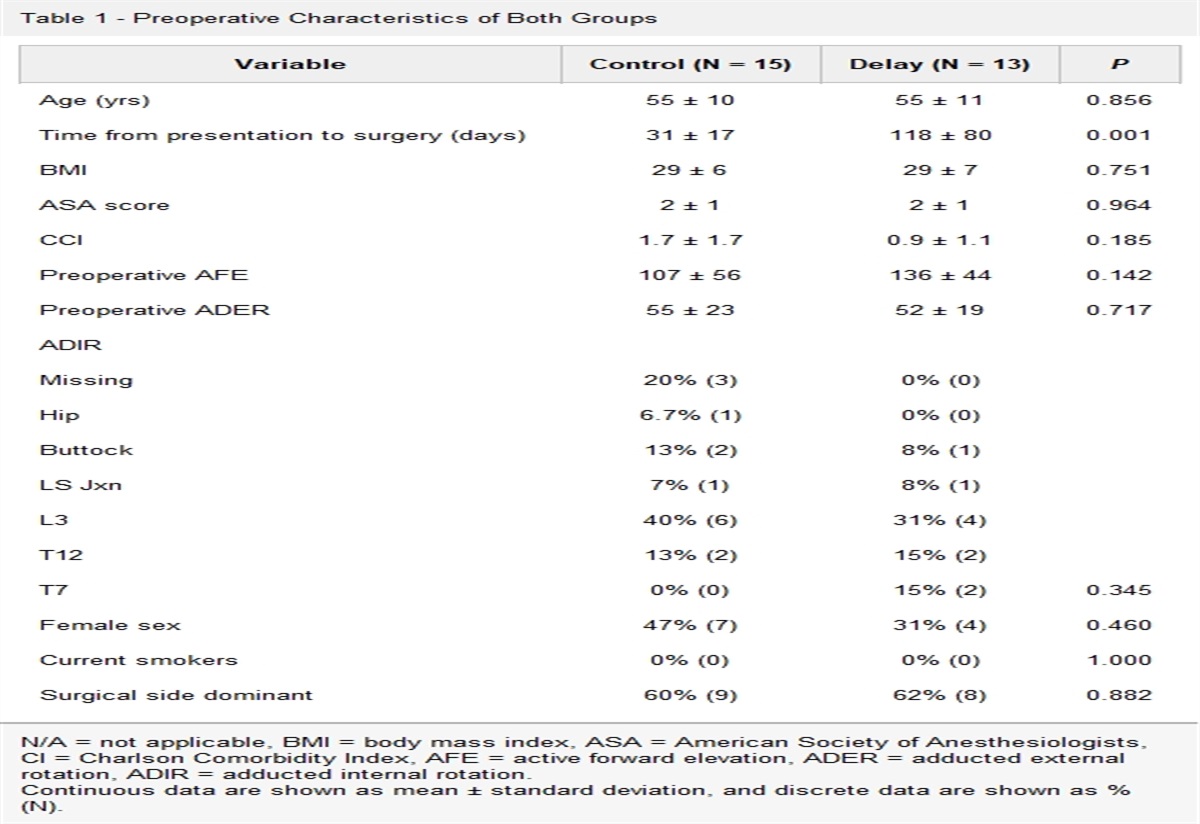
Data CollectionPatient self-identified demographic data are presented in Table 1. For patients with version abnormalities, femoral version and tibial torsion were measured by one of two attending orthopaedic surgeons, fellowship-trained in limb deformity correction, based on preoperative CT version studies using axial cuts through the hip, knee, and ankle. Femoral version was measured using the angle between the femoral neck and a line contacting the most posterior point on the medial and lateral femoral condyles. Tibial torsion was similarly measured as the angle between a line contacting the most posterior points on the medial and lateral femoral condyles and a transmalleolar axis line. This technique has been previously described by the authors.16 Patients with a version greater than the typically accepted range of 10° to 20° of anteversion were classified to have excessive femoral anteversion while those with less than this reference range were identified to have relative excessive femoral retroversion. Similarly, a reference range of 20° to 30° of external tibial torsion was used, and those with tibial torsion exceeding this range were determined to have excessive external tibial torsion.
Table 1 - Cohort Demographics Sample Characteristic Rotational Deformity Control P Value N (%) N (%) Sex P = 0.752 Male 8 (38.1) 14 (42.4) Female 13 (61.9) 19 (57.6) Race P = 0.009 White 13 (61.9) 17 (51.5) Hispanic 3 (14.3) 0 (0.00) Other 2 (9.5) 2 (6.10) Black or African American 1 (4.8) 0 (0.00) Asian or Pacific Islander 2 (9.5) 14 (42.4) Median (IQR) Median (IQR) Age, yr 26 (22-36) 31 (23-33) P = 0.411IQR = interquartile range.
The primary outcome measure was the LD-SRS survey and PROMIS survey scores. Preoperative total scores and subscores are presented in Table 2.
Table 2 - LD-SRS and PROMIS Scores by Subgroup Survey Rotational DeformityPROMIS = patient-reported outcomes measurement information system. Bold represents statistically significant data.
To determine the difference between the LD-SRS and PROMIS scores between both groups, a two-sample t-test with equal variances was used. Interval data were expressed using mean values and standard deviation. A Shapiro-Wilk test was used to assess the normality of age distribution for both groups. A chi square test was used for a sex comparison between the two groups (given that there were more than five subjects in each group), and a Fisher exact test was used to compare self-reported race between the version abnormality and control groups (given that there were less than five subjects in some of the groups). Statistical analysis was performed using Microsoft Excel 2019 Statistical Analysis Toolpak, StataCorp Stata/IC 13.1 for Mac, DATAtab Team, and Astatsa (2016, Navendu Vasavada).
Results DemographicsTable 1 presents the cohort demographics. A total of 54 subjects were evaluated, 21 patients with femoral version abnormalities and 33 healthy control subjects. Age was not normally distributed among groups and, therefore, is presented as a median and interquartile range. There were eight male patients (38.1%) in the version abnormality group compared with 14 (42.4%) in the control group (P = 0.752). A higher percentage of patients identified as Asian/Pacific Islanders in the control group while a higher percentage of patients identified as White in the version abnormality group (P = 0.009).
Rotational Deformity GroupIn the rotational deformity group, 13 of the 21 patients presented with excessive femoral anteversion while eight presented with excessive femoral retroversion (Figure 1). The average femoral version of the anteversion group was 36° ± 7° (20° to 47°). The average femoral version of the retroversion group was −9° ± 14° (−42° to 5°). Eight of the 21 cases were indicated for concomitant external tibial torsion correction with an average tibial version of 46° ± 7° (38° to 60°). Nine of 21 patients in this cohort were indicated for concomitant hip or knee arthroscopy at the time of derotation to address intra-articular pathology that was thought to be secondary to the bony deformity.
 Figure 1:
Figure 1: Photographs showing preoperative AP (A) and PA (B) clinical imaging of a representative patient with excessive bilateral femoral anteversion and external tibial torsion on the right side. Radiographs showing a CT version of the study with cuts through the hips (C), knees (D) and ankles (E and F) indicating 36° femoral anteversion and 38° tibial torsion on the right and 40° femoral anteversion and 27° tibial torsion on the left.
PROM ComparisonsAcross all total and subscore categories for the LD-SRS survey and the PROMIS survey, patients with rotational deformities reported markedly worse scores than healthy control subjects (Table 2).
For the LD-SRS survey, patients with femoral version abnormalities reported statistically significantly worse scores than the asymptomatic control cohort for Total (3.46 ± 0.66 vs. 4.58 ± 0.37, P < 0.001), Function/Activity (3.48 ± 0.83 vs. 4.44 ± 0.4, P < 0.001), Mental Health (3.41 ± 0.96 vs. 4.3 ± 0.73, P < 0.001), Pain (3.55 ± 0.9 vs. 4.81 ± 0.31, P < 0.001), and Self-Image/Appearance (3.37 ± 0.79 vs. 4.75 ± 0.43, P < 0.001). This statistically significant difference in reported outcomes was similarly mirrored in the PROMIS survey scores. Patients with femoral version abnormalities reported significantly worse scores compared with the control cohort in the domains of Physical Function (41.6 ± 7.58 vs. 60.0 ± 7.28, P < 0.001), Pain Intensity (45.85 ± 8.04 vs. 33.7 ± 4.89, P < 0.001), Pain Interference (56.78 ± 9.63 vs. 42.8 ± 6.6, P < 0.001), Global Mental Health (47.97 ± 9.68 vs. 55.3 ± 7.81, P = 0.004), and Global Physical Health (45.23 ± 7.49 vs. 58.2 ± 7.07, P < 0.001).
DiscussionThe primary goal of this study was to establish quality-of-life deficit between patients with femoral version abnormalities and healthy control subjects using preoperative LD-SRS and PROMIS scores. Notably, it was found that patients with femoral version abnormalities reported markedly worse preoperative scores across all domains in both the LD-SRS and the PROMIS surveys. It has previously been reported that lower limb deformities in pediatric and adolescent patients can have debilitating effects on patient-reported quality of life.17,18 Our data expand on these findings, demonstrating that for individuals with severe femoral version abnormalities, such quality-of-life detriments may persist into adulthood.
Capturing the Patient ExperienceFabricant et al13 previously described the value of a limb deformity–specific questionnaire for evaluating patient-reported outcomes. Indeed, individuals with femoral version abnormalities may present with a variety of reports ranging from pain to gait disturbance to cosmetic concerns. Although more widely used PROMs, such as the PROMIS domains, have an intrinsic value in their widespread usage and recognition, they may lack the specificity to capture the patient experience regarding specific limb deformities such as excessive femoral version. In comparison, the LD-SRS survey includes specific domains, such as the Self-Image/Appearance subscore, designed to precisely capture this unique limb-deformity experience. One notable strength of this study is the utilization of both the LD-SRS and the PROMIS surveys. The combined suite of these preoperative questionnaires allowed for limb deformity–specific and generalized PROM responses capturing the range of patient experiences with excessive femoral version abnormalities. Bernstein et al19 explored the relationship between PROM scores on the PROMIS questionnaire compared with the SRS domains. They reported a strong correlation between the PROMIS Physical Function/Mobility and Pain Interference domains to the SRS Function/Activity and Pain domains, respectively. Similarly, we found that both the PROMIS Function and LD-SRS Function/Activity scores were worse in the version abnormality group compared with the control group. This increases our confidence in using the LD-SRS and PROMIS surveys in combination to capture the quality-of-life experience for patients presenting with femoral version abnormalities.
Clinical Decision MakingShared decision making and the utilization of clinically relevant PROMs have been a major focus of recent orthopaedic research.20–22 Kim et al23 reported the value of using preoperative patient-reported outcome surveys to better evaluate surgical outcomes. They found that PROM surveys can effectively screen for social, behavioral, or functional factors preoperatively that may place patients at higher risk of failure. Moreover, Jayakumar and Bozic20 described how tools that incorporate PROMs in the preoperative planning period for patients indicated for total joint arthroplasty may help identify areas of particular concern for a patient and aid in surgical planning and postoperative care.
The LD-SRS and PROMIS surveys may hold a similar value as clinical decision-making tools, providing surgeons with a patient-reported threshold that can help support surgical decision making. The development of such tools and the creation of actionable thresholds based on PROMs help empower the patient in shared decision-making models.24,25 The results of this investigation are an important first step in validating the combined usage of the LD-SRS and PROMIS surveys to accurately capture the patient-reported quality-of-life deficit for individuals with excessive femoral version.
LimitationsThere are limitations to this study. First, because this was a retrospective analysis of previously collected data, no previous statistical analysis could be done. Second, it is important to mention that eight of 21 of the femoral rotational deformities presented with varying degrees of ipsilateral tibial torsion. Our inclusion criteria specifically queried patients who were indicated for femoral derotational osteotomies; however, most of these patients also presented with some degree of a tibial version abnormality. It is impossible to determine whether tibial or femoral contributions are more responsible for the reported deficit in the patient-reported quality-of-life scores. The PROM scores likely reflect a combination of both tibial and femoral implants, and thus, it is important for surgeons evaluating patients with version abnormalities to assess both the femur and the tibia. In addition, statistical comparisons between the version abnormality and control groups showed a notable difference in individuals' racial self-identification. Although this statistical factor does not confound any findings from the study, it is something that may be controlled for through larger sampling in future studies.
The most important limitation to discuss is due to the retrospective nature of this study, the patients in the rotational deformity cohort were already indicated for surgery. Thus, this cohort represents the patients with the most severe version abnormalities indicated for surgical intervention. Indeed, this introduces a level of bias in that those individuals indicated for surgery likely will report worse quality of life than healthy control subjects. The question remains as to whether patients with notable version abnormalities who have not presented for clinical evaluation would also report worse quality of life than control subjects with normal version. However, this question is extremely difficult to answer without obtaining CT version studies on asymptomatic adults. We used available data to capture patient-reported quality of life measures in those patients who did present for evaluation and demonstrated deficits in the rotational deformity group as compared with the control group. Notably, the version of the control group is unknown and assumed to be within the normal range given the lack of lower extremity reports, but this is another limitation of this study because we could not control for version of the control group. It is unclear how this data may apply to patients with less severe version abnormalities and whether these patients may also have deficits in patient-reported quality-of-life scores.
Future DirectionsFollowing the results of this study, an important next step will be the collection of postoperative LD-SRS and PROMIS surveys to evaluate the success of surgical intervention for version abnormalities. A prospective study should also be conducted with a larger number of patients and wider range of deformity to determine whether the severity of version abnormality correlates with LD-SRS and PROMIS scores.
ConclusionPatients with excessive femoral version abnormalities report lower quality of life across all domains measured in the LD-SRS and PROMIS questionnaires. This study serves to describe the quality-of-life deficit experienced by patients with femoral version abnormalities and to further validate that the LD-SRS and PROMIS surveys as powerful tools that can capture this quality-of-life deficit.
References 1. Gugenheim JJ, Probe RA, Brinker MR: The effects of femoral shaft malrotation on lower extremity anatomy. J Orthop Trauma 2004;18:658-664. 2. Karaman O, Ayhan E, Kesmezacar H, Seker A, Unlu MC, Aydingoz O: Rotational malalignment after closed intramedullary nailing of femoral shaft fractures and its influence on daily life. Eur J Orthop Surg Traumatol 2014;24:1243-1247. 3. Gruskay JA, Fragomen AT, Rozbruch SR: Idiopathic rotational abnormalities of the lower extremities in children and adults. JBJS Rev 2019;7:e3. 4. Tönnis D, Heinecke A: Current concepts review - acetabular and femoral anteversion: Relationship with osteoarthritis of the hip. J Bone Joint Surg 1999;81:1747-1770. 5. Terjesen T, Benum P, Anda S, Svenningsen S: Increased femoral anteversion and osteoarthritis of the hip joint. Acta Orthop Scand 1982;53:571-575. 6. Moya L, Buly R, Henn F, Kelly B, Ma Y, Molisani D: Femoral retroversion in patients with femoroacetabular impingement: A cofactor in the development of hip osteoarthritis. Orthop Proc 2010;92:526. 7. Buly RL, Sosa BR, Poultsides LA, Caldwell E, Rozbruch SR: Femoral derotation osteotomy in adults for version abnormalities. J Am Acad Orthop Surg 2018;26:e416-e425. 8. Dickschas J, Harrer J, Reuter B, Schwitulla J, Strecker W: Torsional osteotomies of the femur. J Orthop Res 2015;33:318-324. 9. Albersheim M, Noonan B, Chau M, Cooper T, Tompkins M: Rotational osteotomy for femoral version/tibial torsion. Curr Rev Musculoskelet Med 2022;15:667-672. 10. Nelitz M: Femoral derotational osteotomies. Curr Rev Musculoskelet Med 2018;11:272-279. 11. Heath MR, Shin TJ, Mehta R, et al.: Patients with lower limb deformity report worse quality of life than control subjects regardless of degree of deformity. J Am Acad Orthop Surgeons Glob Res Rev 2021;5:e21.00182. 12. Billig JI, Sears ED, Travis BN, Waljee JF: Patient-reported outcomes: Understanding surgical efficacy and quality from the patient's perspective. Ann Surg Oncol 2020;27:56-64. 13. Fabricant PD, Borst EW, Green SA, Marx RG, Fragomen AT, Rozbruch S: Validation of a modified Scoliosis Research Society instrument for patients with limb deformity: The limb deformity-Scoliosis Research Society (LD-SRS) score. J Limb Lengthening Reconstr 2016;2:86. 14. Cella D, Yount S, Rothrock N, et al.: The patient-reported outcomes measurement information System (PROMIS): Progress of an NIH roadmap cooperative group during its first two years. Med Care 2007;45:S3-S11. 15. Raad M, Jain A, Huang M, et al.: Validity and responsiveness of PROMIS in adult spinal deformity: The need for a self-image domain. Spine J 2019;19:50-55. 16. Ellsworth BK, Hoellwarth JS, Rozbruch SR: Percutaneous femoral derotational osteotomy in the skeletally immature patient. JBJS Essent Surg Tech 2022;12:e22.00003. 17. Cooper A, Chhina H, Klassen A, Kopec J, Park S, Fortes C: Quality of life of children with lower limb deformities: A systematic review of patient-reported outcomes and development of a preliminary conceptual framework. J Limb Lengthening Reconstr 2017;3:19. 18. Montpetit K, Hamdy RC, Dahan-Oliel N, Zhang X, Narayanan UG: Measurement of health-related quality of life in children undergoing external fixator treatment for lower limb deformities. J Pediatr Orthop 2009;29:920-926. 19. Bernstein DN, Papuga MO, Sanders JO, Rubery PT, Menga EN, Mesfin A: Evaluating the correlation and performance of PROMIS to SRS questionnaires in adult and pediatric spinal deformity patients. Spine Deform 2019;7:118-124. 20. Jayakumar P, Bozic KJ: Advanced decision-making using patient-reported outcome measures in total joint replacement. J Orthop Res 2020;38:1414-1422. 21. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ: John charnley award: Preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res 2016;474:321-329. 22. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ: Can preoperative patient-reported outcome measures Be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res 2017;475:149-157. 23. Kim S, Duncan PW, Groban L, Segal H, Abbott RM, Williamson JD: Patient-reported outcome measures (PROM) as A preoperative assessment tool. J Anesth Perioper Med 2017;4:274-281. 24. Bingham CO, Noonan VK, Auger C, Feldman DE, Ahmed S, Bartlett SJ: Montreal Accord on patient-reported outcomes (pros) use series – paper 4: Patient-reported outcomes can inform clinical decision making in Chronic Care. J Clin Epidemiol 2017;89:136-141. 25. Price A, Smith J, Dakin H, et al.: The arthroplasty candidacy help engine tool to select candidates for hip and knee replacement surgery: Development and economic modelling. Health Technol Assess 2019;23:1-216.
留言 (0)