
記住我
Lateral compression type 1 (LC-1) pelvic ring injuries account for more than 60% of all pelvic ring injuries and most demonstrate minimal displacement and may be treated nonsurgically with predictable outcome.1–10 The practice of obtaining plain radiographs after mobilization from bed has been widely used to assess for fracture displacement, which may warrant alteration of the proposed treatment plan.11 However, clear evidence suggesting utility of these radiographs in changing treatment plans or outcomes is lacking. Although some recent authors have suggested limited value of these postmobilization radiographs, specific variables remain understudied.11 Practice patterns, clinical and radiographic indications for postmobilization radiography, and potential benefits have not been described. Some of the detriments to obtaining unnecessary imaging include added expense to the patient and healthcare system, unnecessary radiation exposure, and prolonged hospital stay.11–13
The purposes of this project were to describe patients with LC-1 pelvic injuries, to characterize fracture patterns, and to determine whether postmobilization radiographs affected management. Final fracture alignment was also assessed. Our hypothesis was that the practice of obtaining postmobilization radiographs would increase over time, although no associations of postmobilization radiography with treatment or radiographic outcome would be realized.
MethodsBetween 2015 and 2019, 409 patients with LC-1 pelvis ring injuries were identified from the trauma registry of an urban level 1 trauma center.14,15 Half of the patients from each of these years were randomly selected, and further chart review was performed for those 178 patients after Institutional Review Board approval. Patients younger than 18 years were excluded (n = 6). Sixteen patients had radiography and/or care initiated at an outside hospital and thus were excluded. This resulted in a final study population of 156 patients. Demographic, injury, and treatment data were collected.
Initial fracture displacement and change in displacement were measured for all 156 patients using anterior-posterior (AP) pelvis radiographs obtained at the time of presentation and compared with all radiographs obtained subsequently. These displacements were classified into four categories: < 5 millimeters (mm), 5 to 10 mm, 10 to 15 mm, and > 15 mm. Measurements were taken using the hospital's imaging software distance tool, and the sum of the areas of fracture displacement on the right and left sides were used in cases of multiple fractures or comminution. Attending physicians developed treatment plans for surgical or nonsurgical care at their own discretion. Whether postmobilization radiographs were taken was determined through chart review, and those physicians who obtained postmobilization radiographs documented their treatment plan after obtaining and reviewing these images. Postmobilization radiographs were obtained after the patient mobilized from bed, during the inpatient stay. All patients treated nonsurgically were permitted progressive weight-bearing as tolerated. All patients treated surgically underwent percutaneous fixation of the posterior pelvic ring and percutaneous internal fixation or external fixation of the anterior pelvic ring.
Statistical AnalysisData were analyzed using the Statistical Package for Social Sciences version 28 (IBM SPSS). Variables was assessed using Student T-test for continuous variables and Pearson Chi-square Test for categorical variables. Multivariate binary logistic regression was performed to account for possible confounders; variables with univariate P < 0.20 were included in the analysis.
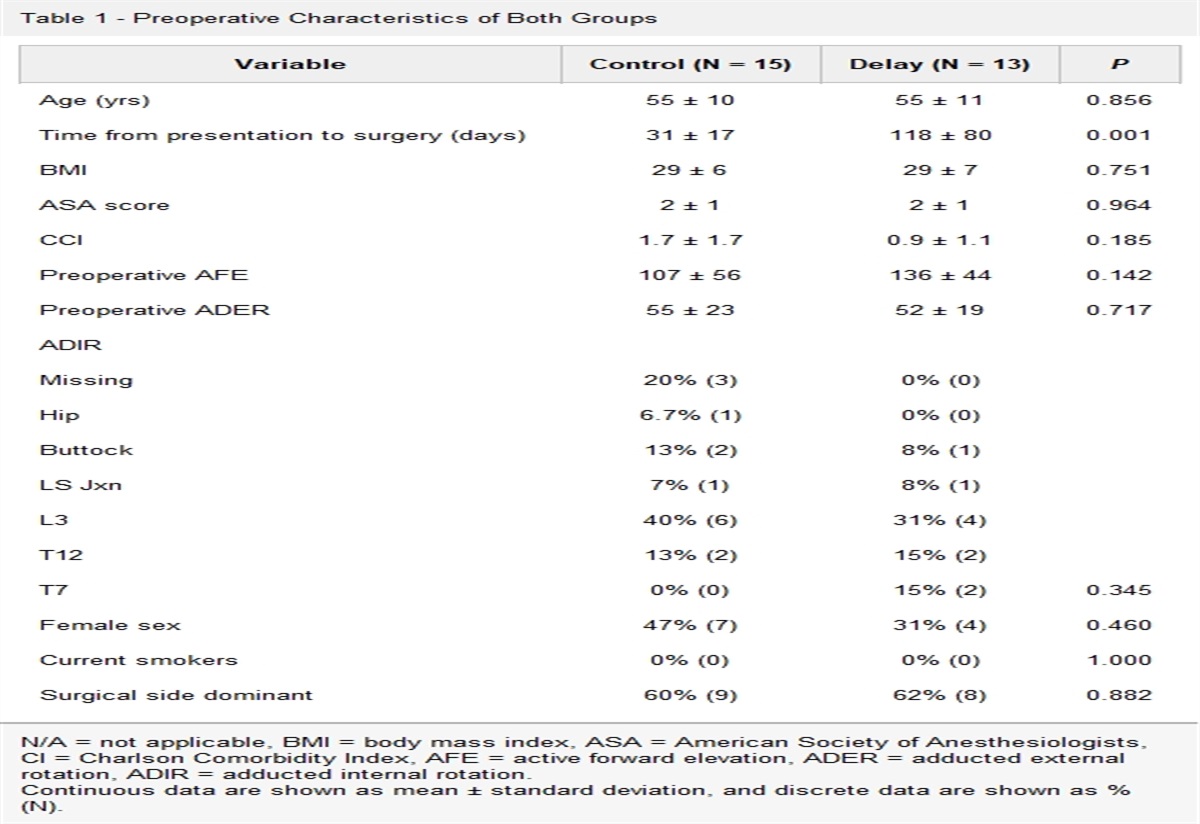
ResultsOf the 156 patients reviewed, 98 (62.8%) were women and 58 (37.2%) were men (Table 1). The mean age of all patients was 58.7 years, with the mean age of those treated surgically 44.8 years versus 60.1 for nonsurgical care (P < 0.0001). Seventy-six (48.1%) of all patients were overweight or obese with a BMI of 25 or higher, with no differences in mean BMI between the treatment groups. The most common mechanism of injury was fall from stand (32.0%), followed by motor vehicle collision (24.4%) and fall from height (20.5%). None of the patients treated surgically had a fall from stand (P < 0.001).
Table 1 - Patient Demographics Including Age, Sex, Body Mass Index, and Mechanism of Injury Total (n = 156) Nonsurgical (n = 141) Surgical (n = 15) P Mean age (yrs) 58.7 60.1 44.8 <0.0001 Male 58 (37.2%) 50 (35.5%) 8 (53.3%) 0.005 Female 98 (62.8%) 91 (64.5%) 7 (46.7%) Mean BMI 26.4 26.2 28.3 0.15 Mechanism of injury Fall from stand 50 (32.0%) 50 (35.5%) 0 <0.001 Fall from height 32 (20.5%) 26 (18.4%) 6 (40.0%) Motor vehicle collision 38 (24.4%) 33 (23.4%) 5 (33.3%) Pedestrian vs vehicle 15 (9.6%) 14 (9.9%) 1 (6.7%) Motorcycle crash 10 (6.4%) 9 (6.4%) 1 (6.7%) Bicycle 7 (4.5%) 6 (4.3%) 1 (6.7%) Crush 1 (0.6%) 0 1 (6.7%) Other 3 (1.9%) 3 (2.1%) 0Patients treated surgically and nonsurgically are compared. Data are expressed as total number and as percentage of that column, unless otherwise specified.
Locations of the pelvis and sacrum fractures are shown in Table 2. Overall, 15 patients were treated surgically (9.6%). Unilateral and bilateral pubic ramus fractures had similar distributions among the surgical and nonsurgical groups. However, a larger percentage of the patients treated surgically had zone 2 sacrum fractures (46.5%, P = 0.03).16 Most patients treated surgically had complete sacral fractures (86.7% versus 45.4%, P = 0.001). Of those with complete sacral fractures, 43 (27.6%) were comminuted, and 9 (60%) were treated surgically.
Table 2 - Fracture Characteristics of Pubic Ramus and Sacral Fractures are Shown for all Patients and Compared With Those Who had Postmobilization Radiographs Total (n = 156) Postmobilization radiograph (n = 33) Nonsurgical (n = 141) Surgical (n = 15) P Rami fractures Bilateral 24 (15.4%) 3 (9.1%) 21 (14.8%) 3 (20.0%) 0.62 Unilateral 132 (84.6%) 30 (90.9%) 120 (85.1%) 12 (80.0%) 0.84 1 33 (21.2%) 7 (21.2%) 31 (22.0%) 2 (13.3%) 2 93 (59.6%) 21 (63.6%) 84 (59.6%) 9 (60.0%) 3 19 (12.2%) 3 (9.1%) 16 (11.4%) 3 (20.0%) 4 11 (7.1%) 2 (6.1%) 10 (7.1%) 4 (26.7%) Sacral fracture Zone 1 107 (68.6%) 22 (66.7%) 100 (70.9%) 7 (46.5%) 0.86 Zone 2 46 (29.5%) 10 (30.3%) 39 (27.7%) 7 (46.5%) 0.78 Zone 3 3 (1.9%) 1 (3.0%) 2 (1.4%) 1 (6.7%) 0.72 Partial 79 (50.6%) 18 (54.6%) 77 (54.6%) 2 (13.3%) 1.0 Complete 77 (49.6%) 15 (45.4%) 64 (45.4%) 13 (86.7%) Comminuted 43 (27.6%) 9 (27.3%) 34 (24.1%) 9 (60.0%) 0.82 Non-comminuted 113 (72.4%) 24 (72.7%) 107 (75.9%) 6 (40.0%)P values compare the patients treated nonsurgically with those who had postmobilization radiography.
Initial fracture displacements are shown in Table 3, with groups of <5 mm, 5 to 10 mm, and >10 mm. None of the patients had initial displacements of more than 13 mm. No differences in initial fracture displacement were noted between surgical and nonsurgical groups. Measurements of any further change in alignment were completed after the fractures had healed. Fractures treated surgically were more likely to experience subsequent change in fracture alignment (66.7% versus 26.2%, P = 0.001), although 90% of those with displacement after surgery were <5 mm.
Table 3 - Initial Fracture Displacement and Change in Fracture Alignment Noted at the Time of Union are Shown for Patients Treated Surgically and Nonsurgically Total (n = 156) Postmobilization radiograph (n = 33) Nonsurgical (n = 141) Surgical (n = 15) Initial displacement <5 mm 103 (66.0%) 26 (78.8%) 95 (67.4%) 8 (53.3%) 5-10 mm 42 (26.9%) 7 (21.2%) 37 (26.2%) 5 (33.3%) >10 mm 11 (7.1%) 0 9 (6.4%) 2 (13.3%) Change in alignment Yes 46 (30.1%) 9 (27.3%) 37 (26.2%) 10 (66.7%) <5 mm 41 (26.3%) 8 (24.2%) 32 (22.7%) 9 (60.0%) 5-10 mm 5 (3.2%) 1 (3.0%) 4 (2.8%) 1 (6.7%) >10 mm 1 (0.6%) 0 1 (0.7%) 0 No 109 (69.9%) 28 (72.7%) 104 (73.8%) 5 (33.3%)Thirty-three patients of 156 (21.2%) had postmobilization radiographs. None of these patients were treated surgically. The patients who had postmobilization radiographs were no different from the others in the nonsurgical group regarding demographic variables or BMI. Of those patients who had a postmobilization radiograph, the fracture patterns were no different from those who had no additional radiograph (Table 2). The amount of initial fracture displacement, number of ramus fractures, location of sacrum fracture, and sacrum fracture characteristics were no different from the other patients treated nonsurgically.
Regarding the practice of obtaining postmobilization radiographs, only one of these was obtained in 2015 of 43 patients (2.3%), whereas 67% of patients in 2019 had a postmobilization radiograph. Figure 1 shows the increase in the frequency of postmobilization radiographs over the 5-year study period. Yet, no changes in patient management occurred because of the findings on the postmobilization radiographs. Furthermore, the final fracture alignment of those patients was no different than the other patients treated nonsurgically for LC-1 fracture (Table 3). Although 9 (27.3%) of the patients with postmobilization radiographs had some change in fracture alignment, one had 6 mm of displacement, and the other eight had less than 5 mm of displacement.
 Figure 1:
Figure 1: Chart showing the percentage of LC-1 pelvis ring fractures who received postmobilization radiographs depicted by the year of study from 2015 to 2019.
DiscussionThe utility of postmobilization plain radiographs in treatment decision-making for pelvis ring injury has not been substantiated. Our purposes were to describe patients with LC-1 pelvic injuries and to characterize fracture patterns. Our hypotheses were (1) the practice of obtaining postmobilization radiographs would increase over time and (2) no associations of postmobilization radiography with treatment or radiographic outcome would be realized.
Over the 5 years of study, substantial increase in frequency of obtaining postmobilization radiographs was noted. By 2019, two-thirds of patients had a radiograph after they mobilized from bed, with no change in the demographic and injury features of these patients when compared with the remainder of the population. Other authors have suggested that the amount of radiography obtained over time has increased and have questioned whether this practice has been associated with a commensurate change (and improvement) in management and outcomes.11–13,17 It is likely that substantial variability exists in current practices regarding the type and timing of imaging obtained.12,13,18,19 Specific to LC-1 fractures, some surgeons may routinely obtain these radiographs, whereas others never obtain them.11 Furthermore, indications for surgical intervention have also evolved over time to become more aggressive about performing surgery for the reduction and/or fixation of LC-1 fractures.11,19–23
The patients who had postmobilization radiographs were no different in demographic and mechanism features from the patients who did not have these radiographs. Fracture locations and patterns were also no different between these two groups of patients who were treated nonsurgically. This suggests substantial variability in preferences for diagnostic imaging.11–13 Although the facility and professional costs of an anterior-posterior pelvis radiograph are small, relative to the entire cost of the episode of care, when these costs are multiplied by the large number of patients with LC-1 fracture treated annually, the total costs are substantial.11,12 The detriments of radiation exposure and of prolonged hospital stay must also be considered.11
We were unable to identify any changes in the management of the pelvic ring injury based on the postmobilization radiography findings. Specifically, no change in mobility from bed, weight-bearing recommendations, positional restrictions, or other activity advancement was seen. Last, the final alignment on plain radiography was not substantially different among patients who had a postmobilization radiograph, compared with those who did not. Winston et al11 recently described a series of patients with planned nonsurgical management of pelvic ring injuries, and none of them had a change in the management plan based on postmobilization radiographs. However, they included all pelvis fracture patterns, and no details were provided about the locations and displacements of fractures in their series.
We propose that indication for routine postmobilization radiography of patients with LC-1 injuries does not exist. Initially purported to identify those patients with substantial displacement who would warrant offering surgery for reduction and fixation, none of our patients experienced any change in alignment felt to influence the final fracture alignment or other outcome. It is possible that patients with LC-1 injuries and a planned nonsurgical course will have difficulty mobilizing from bed.4,8,23–25 In such cases surgery has been proposed to provide stability and thus to afford pain relief and to improve mobility from bed.5,11,19,23,26 Progressing to surgery without obtaining postmobilization radiography is a reasonable option, although some patients may elect to continue with a nonsurgical treatment plan.
Future directions include further exploration into the vast variability in the assessment and treatment of LC-1 fractures. Our study group was treated infrequently with surgery. Yet, initial fracture pattern features, demographical variables, mechanism of injury, and associated injuries are among the relative indications surgeons use in developing treatment recommendations.9,19,25 Stress radiographs under anesthesia in the operating room or by lateral positioning in an awake patient have also been proposed to disclose instability of the pelvis.11,27–32 However, the magnitude and location of mobility within the pelvic ring which warrants a recommendation for surgery are also not agreed upon.21–23,33,34 In fact, most senior surgeons do not routinely even obtain any stress radiographs for LC-1 fractures.9
Limitations of the current project include a small number of patients who had postmobilization radiography. The frequency of these images increased vastly over time. Yet, no specific indications for obtaining postmobilization exist within our system, demonstrating variability among attending physician practices. However, the group with postmobilization radiographs was similar to the nonsurgical patients in demographic and injury features, and their radiographic outcomes were also similar, suggesting that this sample is representative of the entire group. Another limitation is the lack of any functional outcomes data or pain medication usage during the treatment course or at the final follow-up. We further do not have data on the length of hospital stay. Despite that, the conclusion regarding lack of utility of routine postmobilization radiography seems reasonable.
ConclusionsIn conclusion, the practice of obtaining postmobilization plain radiography of the pelvis after initial nonsurgical management of LC-1 pelvis ring injury does not seem warranted. None of our patients had a change in the treatment plan after postmobilization radiography, and no differences in final fracture alignment were noted when compared with the group of patients treated nonsurgically without this additional imaging. Yet, the frequency of the radiographs increased substantially over time. Opportunity exists to provide less expensive and more efficient care with less radiation exposure for patients by eliminating this practice.
References 1. Barnfield S, Ingram J, Halliday R, et al.: Tulip: A randomised controlled trial of surgical versus non-surgical treatment of lateral compression injuries of the pelvis with complete sacral fractures (LC1) in the non-fragility fracture patient-a feasibility study protocol. BMJ Open 2020;10:e036588. 2. Bruce B, Reilly M, Sims S: OTA highlight paper predicting future displacement of nonoperatively managed lateral compression sacral fractures: Can it be done? J Orthop Trauma 2011;25:523-527. 3. Gaski GE, Manson TT, Castillo RC, Slobogean GP, OʼToole RV: Nonoperative treatment of intermediate severity lateral compression type 1 pelvic ring injuries with minimally displaced complete sacral fracture. J Orthop Trauma 2014;28:674-680. 4. Hagen J, Castillo R, Dubina A, Gaski G, Manson TT, O'Toole RV: Does surgical stabilization of lateral compression-type pelvic ring fractures decrease patients' pain, reduce narcotic use, and improve mobilization? Clin Orthop Relat Res 2016;474:1422-1429. 5. Kursumovic K, Hadeed M, Bassett J, Parry JA, Bates P, Acharya MR: Lateral compression type 1 (LC1) pelvic ring injuries: A spectrum of fracture types and treatment algorithms. Eur J Orthop Surg Traumatol 2021;31:841-854. 6. Mullis BH, Agel J, Jones C, et al.: Unilateral sacral fractures demonstrate slow recovery of patient reported outcomes irrespective of treatment. J Orthop Trauma 2022;36:179-183. 7. Sembler Soles GL, Lien J, Tornetta P 3rd: Nonoperative immediate weightbearing of minimally displaced lateral compression sacral fractures does not result in displacement. J Orthop Trauma 2012;26:563-567. 8. Slobogean GP, Gaski G, Nascone J, et al.: A prospective clinical trial comparing surgical fixation versus nonoperative management of minimally displaced complete lateral compression pelvis fractures. J Orthop Trauma 2021;35:592-598. 9. Vallier HA, Lowe JA, Agel J, et al.: Surgery for unilateral sacral fractures: Are the indications clear? J Orthop Trauma 2019;33:619-625. 10. Whiting PS, Auston D, Avilucea FR, et al.: Negative stress examination under anesthesia reliably predicts pelvic ring union without displacement. J Orthop Trauma 2017;31:189-193. 11. Winston BA, Sarker M, Putnam D, Gehling P, Eagleton C, Friess D: The utility of obtaining postmobilization imaging in nonsurgical pelvic ring injuries. J Am Acad Orthop Surg 2020;28:556-561. 12. Teo TL, Schaeffer EK, Mulpuri K, et al.: Need for higher quality evidence to determine the utility of postoperative radiography. J Am Acad Orthop Surg Glob Res Rev 2018;2:e026. 13. Teo T, Schaeffer E, Cooper A, Mulpuri K: Do immediate postoperative radiographs change patient management after fracture fixation? A systematic review. J Orthop Trauma 2018;32:211-215. 14. Burgess AR, Eastridge BJ, Young JW, et al.: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856. 15. Young JW, Burgess AR, Brumback RJ, Poka A: Pelvic fractures: Value of plain radiography in early assessment and management. Radiology 1986;160:445-451. 16. Denis F, Davis S, Comfort T: Sacral fractures: An important problem. Retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81. 17. Paydar S, Ahmadi A, Dalfardi B, Shakibafard A, Abbasi H, Bolandparvaz S: Clinical and economic effects of selective radiological evaluation of high-energy trauma patients: A prospective experience of a level 1 busy trauma centre. Emerg Med J 2015;32:535-538. 18. Lefaivre KA, Padalecki JR, Starr AJ: What constitutes a young and burgess lateral compression-I (ota 61-B2) pelvic ring disruption? A description of computed tomography-based fracture anatomy and associated injuries. J Orthop Trauma 2009;23:16-21. 19. Tejwani N, Stevens NM, Ganta A: High-energy lateral compression type 1 injuries of the pelvis: A spectrum of injury. J Am Acad Orthop Surg 2020;28:157-165. 20. Beckmann JT, Presson AP, Curtis SH, et al.: Operative agreement on lateral compression-1 pelvis fractures. A survey of 111 OTA members. J Orthop Trauma 2014;28:681-685. 21. Beckmann J, Haller JM, Beebe M, et al.: Validated radiographic scoring system for lateral compression type 1 pelvis fractures. J Orthop Trauma 2020;34:70-76. 22. Hadeed MM, Tucker NJ, Heare A, Mauffrey C, Parry JA: Rami comminution is associated with displacement of minimally displaced lateral compression type 1 injuries on lateral stress radiographs. J Orthop Trauma 2022;36:489-493. 23. Parry JA, Tucker NJ: Moving forward with the management of minimally displaced lateral compression pelvic ring injuries. Eur J orthopaedic Surg Traumatol orthopedie traumatologie 2022;32:1223-1224. 24. Marchand LS, Working ZM, Rane AA, et al.: Unstable pelvic ring injuries: How soon can patients safely bear weight? J Orthop Trauma 2019;33:71-77. 25. Tornetta P III, Lowe JA, Agel J, et al.: Does operative intervention provide early pain relief for patients with unilateral sacral fractures and minimal or no displacement? J Orthop Trauma 2019;33:614-618. 26. Barei DP, Shafer BL, Beingessner DM, Gardner MJ, Nork SE, Routt MLC: The impact of open reduction internal fixation on acute pain management in unstable pelvic ring injuries. J Trauma 2010;68:949-953. 27. Avilucea FR, Archdeacon MT, Collinge CA, Sciadini M, Sagi HC, Mir HR: Fixation strategy using sequential intraoperative examination under anesthesia for unstable lateral compression pelvic ring injuries reliably predicts union with minimal displacement. J Bone Joint Surg Am 2018;100:1503-1508. 28. Parry JA, Salameh M, Maher MH, Stacey SC, Mauffrey C: The lateral stress radiograph identifies occult instability of lateral compression pelvic ring injuries without sedation. J Orthop Trauma 2020;34:567-571. 29. Parry JA, Salameh M, Funk A, Heare A, Stacey SC, Mauffrey C: Mobilization versus displacement on lateral stress radiographs for determining operative fixation of minimally displaced lateral compression type I (LC1) pelvic ring injuries. Int Orthop 2021;45:1625-1631. 30. Parry JA, Hadeed MM, Strage KE, Heare A, Stacey SC, Mauffrey C: Lateral stress radiographs of lateral compression type 1 pelvic injuries, with the injured side down or up, reliably measure occult instability. J Orthop Trauma 2022;36:494-497. 31. Sagi HC, Militano U, Caron T, Lindvall E: A comprehensive analysis with minimum 1-year follow-up of vertically unstable transforaminal sacral fractures treated with triangular osteosynthesis. J Orthop Trauma 2009;23:313-319. 32. Tosounidis T, Kanakaris N, Nikolaou V, Tan B, Giannoudis PV: Assessment of lateral compression type 1 pelvic ring injuries by intraoperative manipulation: Which fracture pattern is unstable? Int Orthop 2012;36:2553-2558. 33. Carney JJ, Nguyen A, Alluri RK, Lee AK, Marecek GS: A survey to assess agreement between pelvic surgeons on the outcome of examination under anesthesia for lateral compression pelvic fractures. J Orthop Trauma 2020;34:e304-e308. 34. Jacobs R, Kleweno C, Wallace S, et al.: Validation of relative motion measurement method of lateral compression pelvic fractures during examination under anesthesia. J Orthop Trauma 2021;35:e289-e292.
留言 (0)