
記住我
In the past decade, the average hospital stay for common orthopaedic procedures has decreased substantially, leading to a national trend for standard inpatient procedures to be performed in the outpatient setting.1–3 This pattern is seen for total shoulder arthroplasty (TSA) as there has been a 107% increase in the number of ambulatory TSAs performed between 2010 and 2014 in the United States.4 The potential for cost savings in ambulatory procedures is likely the principal driver for this national trend, given that outpatient and inpatient TSAs have been demonstrated to have equivalent postoperative complication rates for appropriately selected patients.1–3
Cost containment is a central issue in the current healthcare environment. In an era of bundled payments, reducing postoperative resource utilization for postoperative hospitalization, readmission, and revision surgery is paramount for limiting costs associated with orthopaedic care.5,6 Although outpatient TSA may be less expensive for the initial procedure and during the short-term postoperative period, more work is needed to characterize differences in long-term postoperative outcomes between inpatient and outpatient TSAs as well as their associated levels of healthcare utilization.1,4,7–11
The primary purpose of this study was to compare outpatient and inpatient TSAs for 90-day postoperative medical complications, emergency department (ED) visits, and readmissions, as well as 2 and 5-year surgical outcomes. A secondary objective was to quantify hospital reimbursements for outpatient and inpatient TSAs at the 30-day, 90-day, and 1-year postoperative intervals. We hypothesized that ambulatory TSA would be less expensive than inpatient TSA and have equivalent postoperative complications.
Materials and Methods DatabaseA retrospective analysis was conducted using the Mariner data set of the PearlDiver Patients Records Database (www.pearldiverinc.com). The Mariner data set includes all payer's claims data from more than 150 million patients from January 2010 to April 2021. The data set is different than other administrative claims databases in that it identifies patients based on distinct patient identifiers. This permits longitudinal tracking of patients and their outcomes as well as minimizes loss to follow-up based on changes in insurance type. PearlDiver only releases deidentified patient information, deeming this study exempt from institutional review board approval.
Patient SelectionAdult patients 18 years and older who underwent an anatomic TSA or reverse TSA for osteoarthritis from 2010 to 2020 were identified using Current Procedural Terminology code 23472. Only elective TSA procedures were included; thus, patients who underwent TSA for fracture and malignancy were excluded using International Classification of Diseases (ICD) diagnosis codes. These elective TSA patients were further stratified based on surgical setting (outpatient versus inpatient). In total, 182,700 patients were included, of which 8752 underwent outpatient TSA and 173,948 underwent inpatient TSA. This study observed 5-year outcomes, and thus, only patients who underwent elective TSA with 5-year active follow-up were included (55,283 TSA patients).
OutcomesThe primary outcomes for this study included the incidence of various 90-day medical complications, readmissions rates, and ED visits. 90-day medical complications included surgical site infection, postoperative renal failure, postoperative anemia, atrial fibrillation (afib), arrhythmia without afib, bleeding complications, blood transfusion, pneumonia, stroke, death, deep vein thrombosis, heart failure, pulmonary embolism, respiratory failure, and sepsis. To determine the readmission rate, the PearlDiver database searches for member inpatient records occurring after the index procedure within a specified end point (90 days for our study). It then provides a breakdown for the 90-day readmissions based on the primary ICD diagnosis codes. These ICD codes were further stratified into joint-specific and non–joint-specific readmission rates. Other outcomes included long-term surgical complications within 2 and 5 years of TSA as well as 30-day, 90-day, and 1-year average reimbursements. Total reimbursements at each postoperative time interval included reimbursement for the index surgery and any reimbursements within the specified postoperative interval after the index surgery. Reimbursements are defined as payment received by healthcare providers, hospitals, or other healthcare facilities for providing a medical service.
Propensity Score MatchingPropensity matching of patients who had an outpatient TSA and those who had an inpatient TSA was conducted to control for measured covariates and to mitigate potential confounders. The propensity score was based on the conditional probability of having undergone an outpatient or inpatient TSA based on age, Charlson Comorbidity Index, obesity status, and smoking status. These potential predictor variables were selected based on prior work assessing risk factors of failure of TSA.12,13 Matching was conducted using a 1:2 nearest neighbor matching ratio by univariate analysis. This was done using demographics collected at the time of TSA among the outpatient and inpatient cohorts. Propensity score matching was conducted using R software provided by PearlDiver.
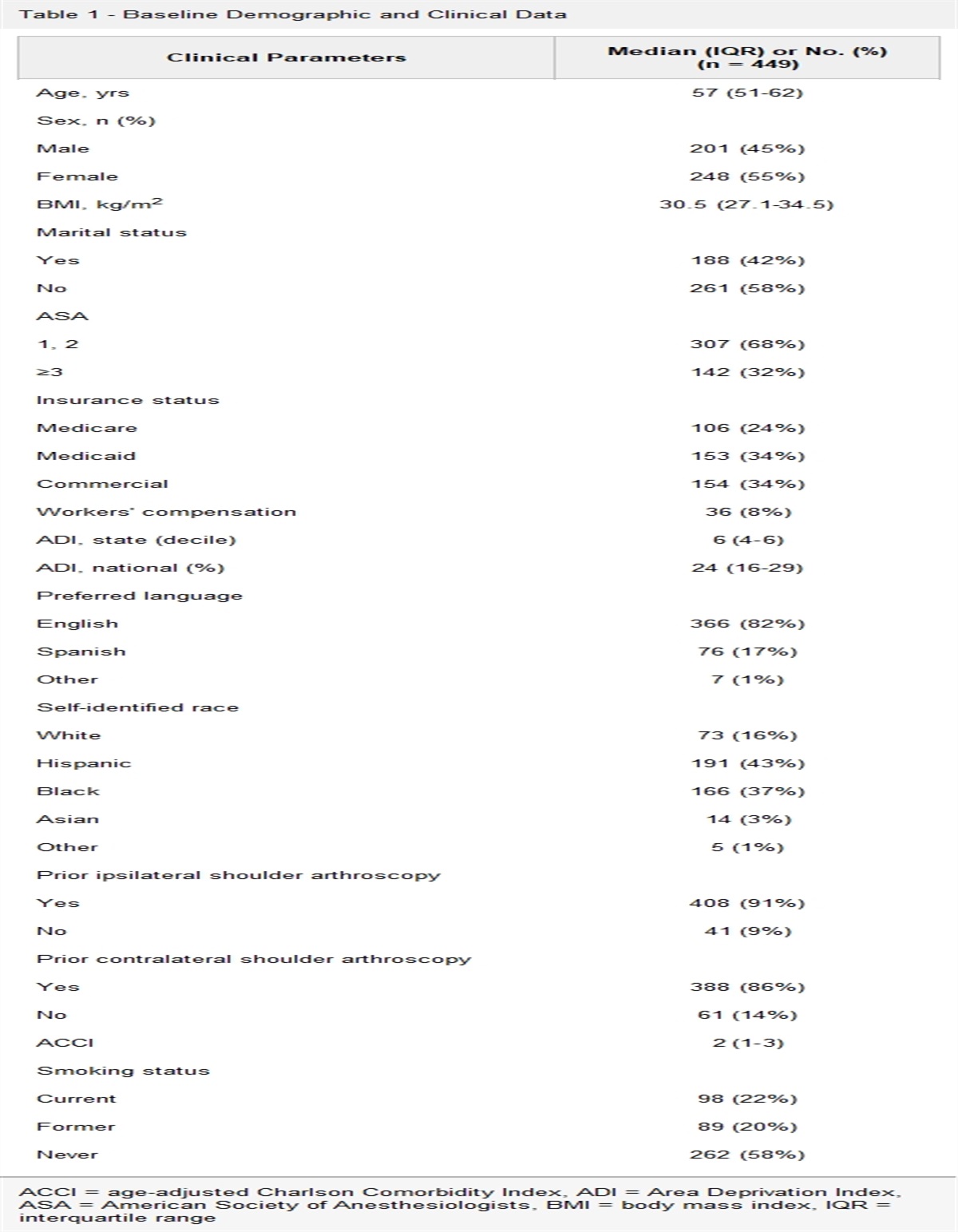
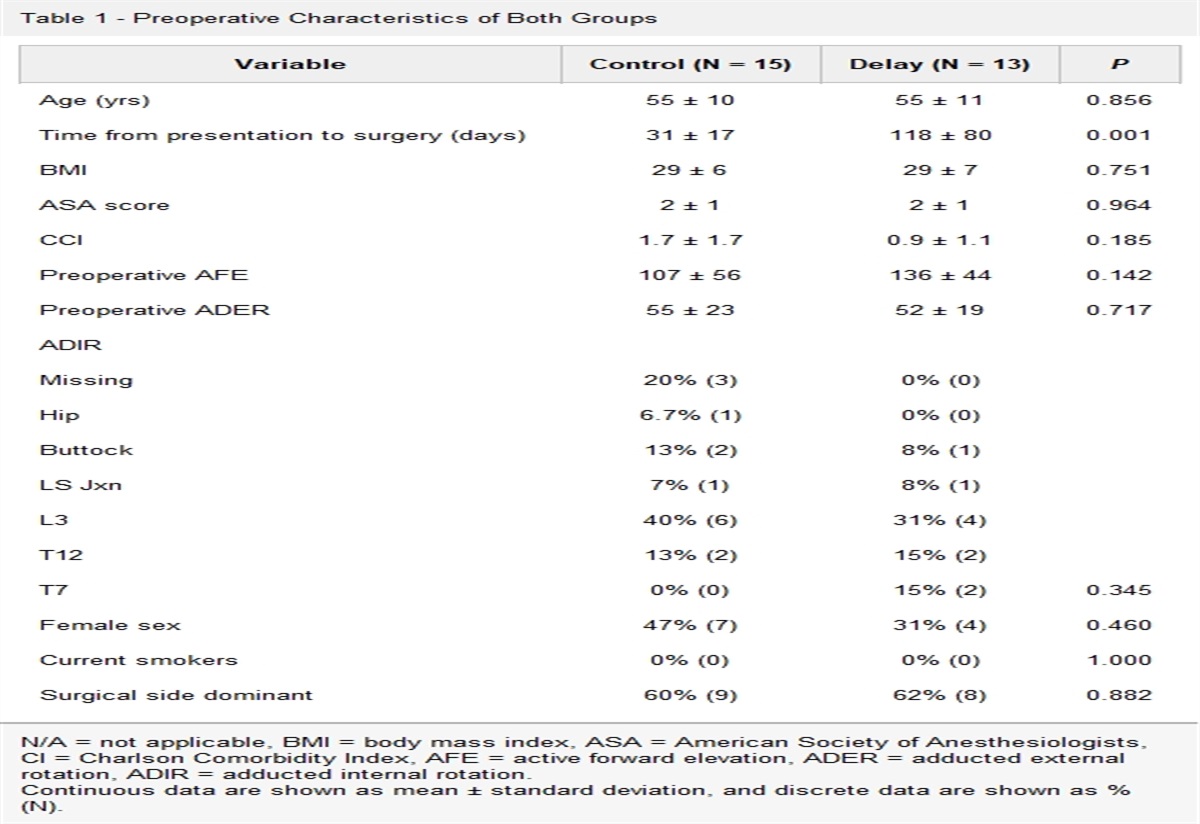
After matching, a total of 4831 patients were included in our final cohort. Of these patients, 1613 (33.4%) underwent outpatient TSA and 3218 (66.6%) underwent inpatient TSA (Table 1). No significant differences were observed in demographics and comorbidities between patients undergoing outpatient and inpatient surgery (Table 1).
Table 1 - Demographic Information for Outpatient TSA and Inpatient TSA Category Total Outpatient Inpatient No. No. % No. % P Value Total 4831 1613 — 3218 — — Age 1.000 <40 23 8 0.50 15 0.47 — 40-50 207 70 4.34 137 4.26 — 50-60 1102 368 22.81 734 22.81 — 60-70 2077 693 42.96 1384 43.01 — 70-80 1422 474 29.39 948 29.46 — CCI 0 1820 607 37.63 1213 37.69 1.000 1 1218 406 25.17 812 25.23 — 2 768 256 15.87 512 15.91 — 3 469 157 9.73 312 9.70 — >3 556 187 11.59 369 11.47 — Sex Male 2357 787 48.79 1570 48.79 0.998 Female 2474 826 51.21 1648 51.21 0.998 Obesity (BMI > 30) 1261 422 26.16 839 26.07 0.995 Smoking 1065 356 22.07 709 22.03 0.976BMI = body mass index, CCI = Charlson Comorbidity Index, TSA = total shoulder arthroplasty.
Data on patient demographics, complications, readmissions, and reimbursements of the matched cohorts were analyzed with univariate analysis using R software provided by PearlDiver. Univariate analysis was conducted using chi square tests, Fisher exact tests, and Student t-tests where appropriate. Significance was set at P < 0.05.
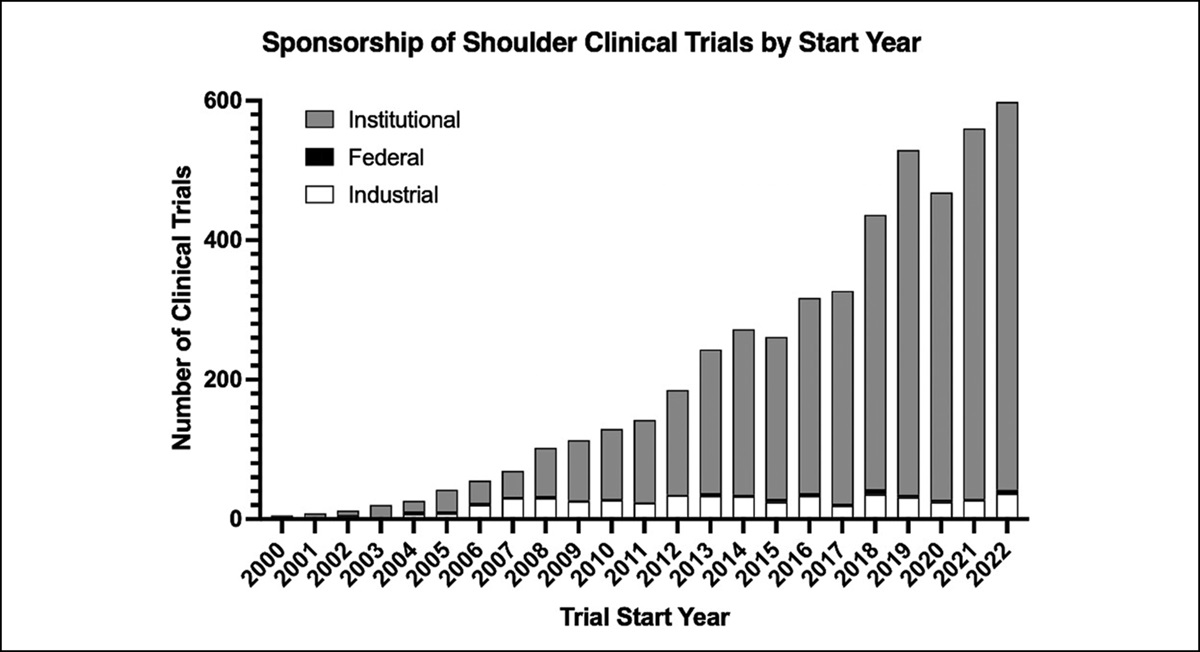
Results Trends in Utilization of Outpatient TSAOf the 182,700 patients who underwent TSA, 8752 (4.8%) underwent outpatient TSA. The percentage of utilization of outpatient TSA increased by 358% from 2.2% in 2010 to 10.2% in 2020 (Table 2 and Figure 1).
Table 2 - The Change in Utilization of Outpatient TSA From 2010 to 2020 Year Total Outpatient No. No. % 2010 9613 213 2.22 2011 10,739 240 2.23 2012 12,378 284 2.29 2013 14,042 326 2.32 2014 15,809 449 2.84 2015 16,272 569 3.50 2016 17,361 639 3.68 2017 18,398 858 4.66 2018 20,905 1219 5.83 2019 24,358 1637 6.72 2020 22,825 2318 10.16TSA = total shoulder arthroplasty.
 Figure 1:
Figure 1: Graph showing change in utilization of outpatient TSA from 2010 to 2020. TSA = total shoulder arthroplasty.
Postoperative ComplicationsCompared with patients undergoing inpatient TSA, those undergoing outpatient TSA had significantly less risk of 90-day postoperative anemia (1.36% vs. 2.77%, P = 0.002), renal failure (0.93% vs. 1.74%, P = 0.017), afib (4.65% vs. 6.96%, P = 0.002), pneumonia (0.87% vs. 2.24%, P < 0.001), respiratory complication (0.56% vs. 1.18%, P = 0.038), and urinary tract infection (UTI) (2.73% vs. 3.92%, P = 0.035) (Table 3).
Table 3 - Ninety-Day Postoperative Complications for Outpatient TSA and Inpatient TSA Category Total Outpatient Inpatient No. No. % No. % P Value 4831 1613 — 3218 — — SSI 67 18 1.12 49 1.52 0.254 Renal failure 71 15 0.93 56 1.74 0.017 Anemia 111 22 1.36 89 2.77 0.002 Arrhythmia w/afib 299 75 4.65 224 6.96 0.002 Arrhythmia w/o afib 137 42 2.60 95 2.95 0.492 Bleeding complication — <11 0.50 14 0.44 0.767 Blood transfusion 56 21 1.30 35 1.09 0.512 Pneumonia 86 14 0.87 72 2.24 <0.001 Stroke — <11 0.62 28 0.87 0.353 Death — <11 0.06 <11 0.09 0.722 DVT 46 11 0.68 35 1.09 0.171 Heart failure 128 36 2.23 92 2.86 0.201 PE — <11 0.68 30 0.93 0.371 Respiratory complication — <11 0.56 38 1.18 0.038 UTI 170 44 2.73 126 3.92 0.035 Sepsis — <11 0.50 33 1.03 0.058afib = atrial fibrillation, DVT = deep vein thrombosis, PE = pulmonary embolism, SSI = surgical site infection, TSA = total shoulder arthroplasty, UTI = urinary tract infection, w/ = with.
Significance at P < 0.05 has been presented in bold; <11: PearlDiver does not report values <11.
Compared with patients undergoing inpatient TSA, those undergoing outpatient TSA were at higher risk of an ED visit (11.16% vs. 8.48%) or readmission (5.33% vs. 2.08%) within 90 days of the procedure (Table 4). Notably, outpatient TSA patients had higher rates of readmission for both joint-related reasons and non–joint-related reasons relative to inpatient TSA patients.
Table 4 - Healthcare Utilization and Reimbursements for Outpatient TSA and Inpatient TSA Category Total Outpatient Inpatient No. No. % No. % P Value 4831 1613 — 3218 — — ED visits 453 180 11.16 273 8.48 0.003 Total readmissions 169 86 5.33 67 2.08 <0.001 Joint readmissions 146 52 3.22 18 0.56 <0.001 Non-joint Readmissions 136 34 2.11 49 1.52 <0.001 Reimbursement 30-d reimbursements $15,865.48 $5532.17 — $10,333.31 — P < 0.001 90-d reimbursements $19,845.57 $7610.45 — $12,235.12 — P < 0.001 1-yr reimbursements $37,525.14 $16,941.34 — $20,583.80 — P < 0.001ED = emergency department, TSA = total shoulder arthroplasty.
Significance at P < 0.05 presented in bold.
On average, outpatient TSA was reimbursed significantly less than inpatient TSA at the 30-day, 90-day, and 1-year postoperative intervals (P < 0.001 for all; Table 4). Notably, the reduction in reimbursements for outpatient TSA relative to inpatient TSA decreased over time: 46.5% reduction in reimbursements at 30 days, 37.8% at 90 days, and 17.7% at 1 year.
Surgical OutcomesCompared with patients undergoing inpatient TSA, those undergoing outpatient TSA had significantly less risk of aseptic loosening at the 2-year postoperative interval (1.30% vs. 2.24%, P = 0.026) and periprosthetic joint infection (PJI) at the 5-year postoperative interval (2.23% vs. 3.42%, P = 0.023) (Table 5). No significant differences were observed in 2 or 5-year all-cause revision rates between the inpatient and outpatient cohorts (P > 0.05; Table 5).
Table 5 - Two and 5-Year Surgical Outcomes for Outpatient TSA and Inpatient TSA Category Total Outpatient Inpatient No. No. % No. % P Value 4831 1613 — 3218 — — 2-yr All-cause revision 128 36 2.23 92 2.86 0.201 PJI 100 25 1.55 75 2.33 0.073 Aseptic loosening 93 21 1.30 72 2.24 0.026 MUA 27 11 0.68 16 0.50 0.417 5-yr All-cause revision 169 49 3.04 120 3.73 0.218 PJI 146 36 2.23 110 3.42 0.023 Aseptic loosening 136 35 2.17 101 3.14 0.055 MUA 28 11 0.68 17 0.53 0.507MUA = manipulation under anesthesia, PJI = periprosthetic joint infection, TSA = total shoulder arthroplasty.
Significance at P < 0.05 presented in bold.
Understanding postoperative adverse events associated with ambulatory procedures is critical for surgical decision making between outpatient versus inpatient surgeries. This study demonstrated patients undergoing outpatient TSA to be at less risk for 90-day medical complications, 2-year aseptic loosening, and 5-year PJI compared with patients undergoing inpatient TSA. However, outpatient TSA patients had higher rates of 90-day readmission and ED visits relative to inpatient TSA patients. Reimbursements for surgical care for outpatient TSA was markedly less expensive at all postoperative intervals assessed.
With the increasing utilization of TSA in the United States, transitioning these procedures to the ambulatory setting for appropriate patients may reduce healthcare costs without compromising clinical care.14–17 Inpatient TSA is currently reported to have a hospital stay ranging from 1.1 to 2.2 days, making the trend toward ambulatory TSA a natural transition.1,2,18,19 The financial implications of this trend have been touched on only minimally in prior literature, with Cancienne et al4 demonstrating an average of $3614 decrease in 30-day total costs for 706 ambulatory TSAs performed between 2010 and 2014.4 The results of our investigation advance existing knowledge by reporting long-term surgical outcomes up to 5 years postoperation, as well as metrics of healthcare utilization such as readmissions and ED visits.
Our results are in line with previous studies reporting equivalent or better outcomes and complication rates after ambulatory TSA and inpatient TSA.1,4,7–9 Cancienne et al4 found that TSA patients were more likely to require blood transfusion or develop a UTI within 90 days of inpatient surgery, compared with outpatient surgery. This is consistent with our finding that outpatient procedures were associated with markedly lower postoperative medical complications, including pneumonia, UTI, anemia, arrhythmia, respiratory complications, and renal failure. In the inpatient TSA group, increased risk of infectious complications, such as UTI and pneumonia, as well as respiratory complications, such as atelectasis, may be because of nosocomial risks inherent to inpatient hospitalization. It is important to note that both our study and that by Cancienne et al were conducted retrospectively in patients who were already selected for outpatient or inpatient surgery based on preoperative medical and surgical criteria. Although these criteria for selection of outpatient TSA are not yet standardized, patients selected for outpatient TSA typically have less comorbidities and less severe shoulder impairment.20–22 Although our study matched rigorously for baseline comorbidities, we were unable to match for preoperative surgical characteristics, leaving room for differences between our inpatient and outpatient cohorts. Despite this, we are still able to conclude that, on a national scale, current surgical selection of outpatient versus inpatient TSA has led to patients undergoing outpatient TSA to have at least as good if not better complication rates and outcomes compared with those undergoing inpatient TSA.1
Regarding surgical complications, our study demonstrated lower risk of 2-year aseptic loosening and 5-year PJI for outpatient TSA cases, relative to matched inpatient TSA cases. Similar to our analysis of postoperative medical complications, this difference in surgical complications may be due to a combination of aggressive early mobilization and less risk of nosocomial infections inherent to inpatient hospitalization, respectively, and outpatient selection for younger patients with less comorbidities.23,24 Our findings are supported by prior literature reporting lower surgical complications at 1 year for ambulatory TSA compared with inpatient TSA.10 However, there is currently a paucity of evidence on differences in long-term complications between TSA performed in the two settings. Similar results have been reported in outpatient versus inpatient total knee arthroplasty (TKA), as Kolisek et al25 found comparable 2-year complication rates between 64 patients undergoing inpatient TKA and 64 matched patients undergoing outpatient TKA at a single medical center. In the study by Kolisek et al25 on TKA, two cases in the inpatient cohort developed joint infections compared with zero in the outpatient cohort, although this difference was not statistically significant. Notably, our study did find a notable increase of PJI at the 5-year postoperative interval for TSA.
Regarding healthcare utilization, our study found increased risks of 90-day readmissions and ED visits for the outpatient TSA cohort compared with the inpatient cohort. Furthermore, we found that risks of readmission for joint-related reasons and non–joint-related reasons were both increased in the outpatient cohort relative to the inpatient cohort. Current evidence on the risk of readmission in outpatient versus inpatient TSA is inconclusive.4,7–9,11 Similar to our results, Harris et al11 found higher all-cause, 30-day readmission rates after outpatient TSA relative to inpatient TSA. However, in contrast to our findings, Harris et al11 found equivalent rates of 30-day readmission for surgical reasons between the two groups, whereas we demonstrate that outpatient cases exhibited higher rates of readmission for surgical reasons within 90 days of procedure. Other studies, including the study by Cancienne et al, have previously demonstrated equivalent rates of all-cause readmission between inpatient and outpatient TSA cohorts, in contrast to our findings and the findings by Harris et al.4,7–9 No previous studies have assessed the associated risk of ED visits with outpatient surgery, which is another key driver of increased healthcare costs in the US healthcare system.26–29
The higher healthcare utilization, through more ED visits and readmissions, does influence the cost of care and is paramount for accurate estimation of bundled payments.29
留言 (0)