
記住我
The United States is in the midst of an opioid epidemic, recognized as a nationwide public health crisis.1 Between 2000 and 2017, accidental deaths due to opioid use increased from 2.2 to 13.2 deaths per 100,000 people.2 In particular, orthopaedic surgeons prescribe opioids at high rates.2,3 There have been multiple studies that have investigated risk factors of opioid use after orthopaedic procedures, such as anterior cruciate ligament reconstruction,4 meniscal surgery,5 and hip/knee arthroplasty.6
Total shoulder arthroplasty (TSA) is a common orthopaedic procedure, with several advancements over the years.7 It is generally done on patients with osteoarthritis and inflammatory arthropathy of the shoulder while reverse TSA (rTSA) has become increasingly popular in patients with cuff-tear arthropathy.7 The incidence of revision TSA has been increasing because of the increased incidence of primary TSA and the implementation of TSA in younger patients.8 Revision rates have been estimated to be approximately 11% for TSA,9 with reasons for TSA failure being implant loosening, instability, and periprosthetic fractures.10 Pain control is an important consideration for these patients, and it is important to study the risk factors that can lead to prolonged postoperative opioid use.
The purpose of this study was to determine which preoperative factors are associated with prolonged opioid use after revision TSA. We hypothesized that multiple preexisting patient-related risk factors would be associated with prolonged opioid use after revision TSA.
Methods PearlDiver DatabaseThe M157 Ortho PearlDiver database (www.pearldiverinc.com), which contains records from over 157 million patients between 2010 and 2021, was used for this study. Both International Classification of Diseases (ICD) Ninth and 10th Revision diagnosis codes and as Current Procedural Terminology (CPT) codes were used. All information in the database is deidentified and was queried to identify patients who underwent revision TSA, which includes both revision anatomic TSA and rTSA. Patients undergoing revision TSA were identified using CPT codes 23473 and 23474. In addition, any patients who underwent TSA (CPT 23472) on the same day as an explant (CPT 23334 or 23335) were identified and included in the population.
Risk FactorsProlonged opioid use was defined as using opioids for longer than 1 month postoperatively. Age, Charlson Comorbidity Index, sex, depression, anxiety, substance use disorder (alcohol, opioid, cannabis, sedatives, hypnotics, anxiolytics, cocaine, stimulants, hallucinogens, inhalants, and psychoactive substances), opioid use between 12 months to 1 week of surgery, tobacco use, hypertension, diabetes mellitus, chronic obstructive pulmonary disease (COPD), osteoporosis, previous myocardial infarction (MI), and chronic ischemic heart disease (without an MI) were assessed. Patients with a preoperative diagnosis of depression, anxiety, substance use disorder, myocardial infarction, osteoporosis, chronic ischemic heart disease without prior myocardial infarction, hypertension, diabetes mellitus, COPD, and tobacco use were identified using the ICD codes provided in Appendix Table IA-J (https://links.lww.com/JG9/A310).
Postoperative Opioid PrescriptionsMultiple formulations of hydrocodone, oxycodone, morphine, and tramadol were included in the queries. All patients who received a prescription of these medications within 3 months after their surgery were identified. Patients were stratified based on the timing of their prescriptions. The same opioid formulations were included in our query of preoperative opioid use. Patients with an opioid prescription within 3 months to 1 week before their surgery were identified and placed into the opioid-familiar group. All other patients in the population were placed into the opioid-naïve group.
Data AnalysisDemographic variables and comorbidities were tabulated and reported. Multivariable logistic regression was used to independently analyze patient demographics and comorbid conditions. Odds ratios (OR) and their associated 95% confidence intervals (CIs) were calculated for each risk factor, with P ≤ 0.05 being considered statistically significant. R software (R Foundation for Statistical Computing) embedded within PearlDiver was used for all statistical analyses.
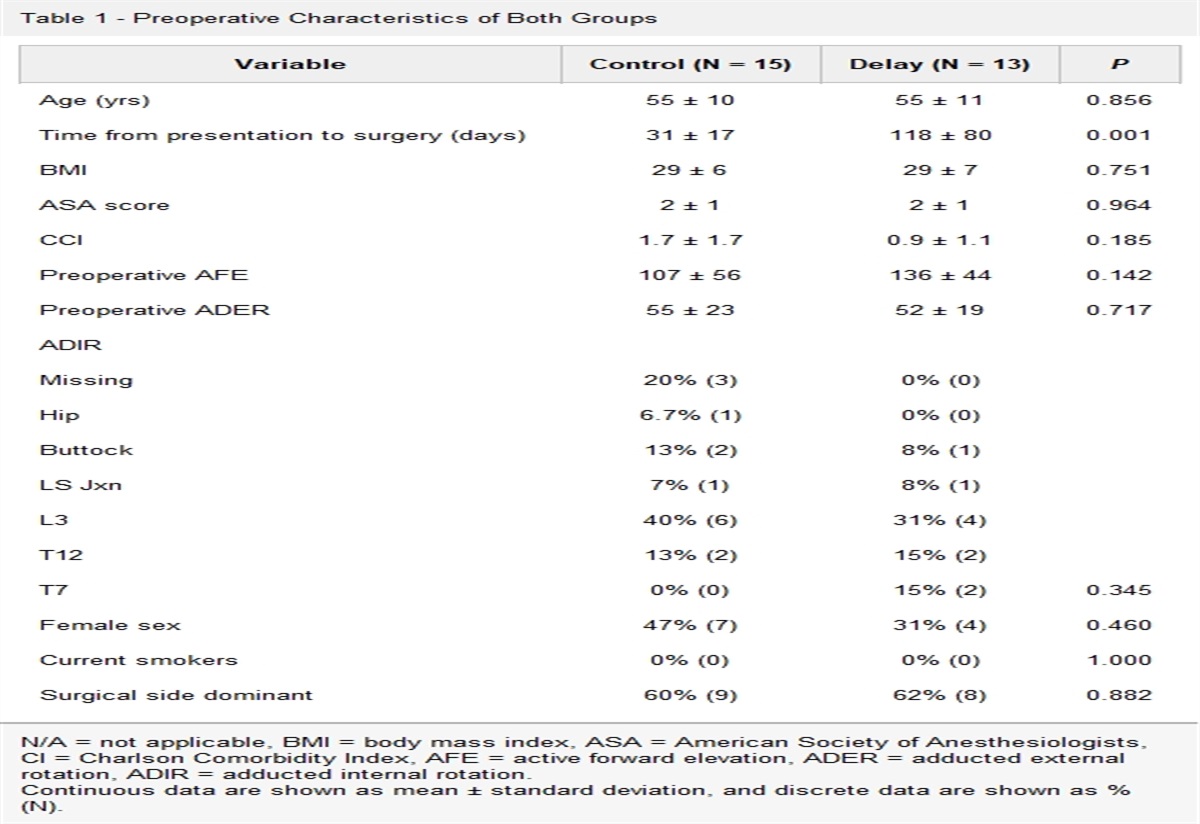
ResultsIn total, there were 14,887 patients (mean age = 67.1 years) who underwent revision TSA in our study period. Most of the patients were female (53.3%), and a large proportion were opioid-familiar (44.1%). Complete cohort demographics are presented in Table 1.
Table 1 - Revision Total Shoulder Arthroplasty Cohort Demographics (N = 14,887) N % Demographics Age (mean ± SD) 67.1 ± 9.7 Female 7929 53.3 Comorbidities CCI (mean ± SD) 2.4 ± 2.5 Anxiety 5448 36.6 Depression 6215 41.7 Substance use disorder 4131 27.7 Tobacco use 3284 22.1 Hypertension 11,588 77.8 Diabetes mellitus 4961 33.3 COPD 1894 12.7 Osteoporosis 2868 19.3 Chronic ischemic heart disease 411 2.8 Previous MI 1398 9.4 Opioid familiar 6562 44.1 Male 2892 44.1 Female 3670 55.9 Reason for revision Infection/inflammation 1726 11.6 Loosening 1891 12.7 Fracture 677 4.5 Other 11,312 76.0CCI = Charlson Comorbidity Index, COPD = chronic obstructive pulmonary disease, MI = myocardial infarction, SD = standard deviation
Stratifying revision TSA patients by opioid familiarity, the patients who had opioid prescriptions within 3 months to 1 week of surgery substantially required more postoperative opioids compared with those who did not at all time points recorded (Figure 1).
 Figure 1:
Figure 1: Graph showing percentage of patients using opioids. Blue line represents the percentage of opioid-familiar patients who continued using opioids up to 3 months postoperatively Orange line represents the percentage of opioid-naïve patients who continued using opioids up to 3 months postoperatively.
On multivariable analysis, multiple preexisting patient-related risk factors were associated with prolonged opioid use after revision TSA. Three months after revision TSA, older age (OR 0.96, CI 0.96 to 0.97) and male sex (OR = 0.90, CI 0.81 to 0.99) were associated with a decreased risk of prolonged postoperative opioid usage. Patients with preexisting depression (OR = 1.21, CI 1.08 to 1.35), substance use disorder (OR = 1.47, CI 1.29 to 1.68), opioid use (OR = 16.25, CI 14.27 to 18.57), and chronic obstructive pulmonary disorder (OR = 1.24, CI 1.07 to 1.42) were at an increased risk of prolonged postoperative opioid use (Table 2).
Table 2 - Risk Factors of Prolonged Opioid Use Opioid Use Duration After Surgery Variable Odds Ratio (95% Confidence Interval) Up to 1 month Age 0.97 (0.97–0.98) Charlson Comorbidity Index 0.98 (0.96–0.99) Male sex 0.93 (0.86–1.00) Depression 0.96 (0.88–1.05) Anxiety 0.95 (0.88–1.04) Substance use disorder 1.06 (0.95–1.18) Opioid familiar 5.62 (5.23–6.05) Tobacco use 0.94 (0.84–1.05) Hypertension 0.99 (0.90–1.08) Diabetes mellitus 0.98 (0.90–1.06) Chronic obstructive pulmonary disease 1.09 (0.97–1.22) Osteoporosis 1.02 (0.93–1.12) Previous myocardial infarction 1.02 (0.90–1.16) Chronic ischemic heart disease 1.03 (0.82–1.28) Up to 2 months Age 0.96 (0.96–0.97) Charlson Comorbidity Index 0.99 (0.97–1.01) Male sex 0.86 (0.78–0.94) Depression 1.15 (1.04–1.27) Anxiety 0.99 (0.90–1.10) Substance use disorder 1.36 (1.20–1.53) Opioid familiar 11.60 (10.52–12.81) Tobacco use 0.99 (0.87–1.13) Hypertension 1.05 (0.93–1.17) Diabetes mellitus 1.09 (0.98–1.20) Chronic obstructive pulmonary disease 1.15 (1.01–1.32) Osteoporosis 0.99 (0.88–1.11) Previous myocardial infarction 1.09 (0.93–1.26) Chronic ischemic heart disease 1.12 (0.86–1.46) Up to 3 months Age 0.96 (0.96–0.97) Charlson Comorbidity Index 0.99 (0.97–1.01) Male sex 0.90 (0.81–0.99) Depression 1.21 (1.08–1.35) Anxiety 1.05 (0.94–1.18) Substance use disorder 1.47 (1.29–1.68) Opioid familiar 16.25 (14.27–18.57) Tobacco use 0.91 (0.79–1.05) Hypertension 1.03 (0.91–1.17) Diabetes mellitus 1.09 (0.97–1.21) Chronic obstructive pulmonary disease 1.24 (1.07–1.42) Osteoporosis 1.04 (0.91–1.17) Previous myocardial infarction 1.11 (0.94–1.31) Chronic ischemic heart disease 1.09 (0.81–1.46)Our study found that younger age, female sex, depression, substance use disorder, opioid familiarity, and COPD were associated with prolonged opioid use after revision TSA. Previous studies assessed the risk factors of prolonged opioid use after primary TSA,11,12 but the literature on revision TSA is limited. Khazi et al12 analyzed 12,038 primary TSA patients from the Humana database between 2007 and 2015, finding that the greatest risk factor was filling an opioid prescription 1 to 3 months before surgery. Over 40% of patients undergoing TSA received opioids 3 months before surgery. Best et al13 assessed the MarketScan database of 5,676 patients, finding that those who underwent primary TSA between 2010 and 2015 had preoperative opioid use, history of drug abuse, depression, anxiety, and surgery performed in the Western United States as risk factors of prolonged opioid use. Our study builds on the literature by analyzing revision TSA patients. Opioid familiarity remained the greatest risk factor, and 44.1% of patients were found to have preoperative opioid use. Similar to primary TSA, depression was a risk factor of prolonged opioid use after revision TSA.
In line with previous literature, male patients were seen to have a decreased risk of developing prolonged opioid use compared with female patients. In orthopaedic sports medicine literature, Rao et al found this to be true in anterior cruciate ligament reconstruction patients4 while Yang et al14 reported on this finding for adolescent idiopathic scoliosis. There are some potential explanations for why this is the case. A study by Jamison et al15 suggested that women are at a greater risk of opioid misuse because of emotional issues and affective distress while men misuse opioids because of legal and behavioral issues. Women were found to be more likely to use prescription opioids than men to cope with interpersonal stress16,17 and use them first thing in the morning.17
After surgery, not only is there physical pain, but there is also a high degree of psychological stress. Preoperative depression was found to be a risk factor of prolonged opioid use in revision TSA patients, which is in line with previous studies. Mohan et al18 performed a systematic review after spine surgery, finding both depression and anxiety as risk factors of prolonged opioid use. Helmerhorst et al found that after musculoskeletal trauma, patients who scored higher on anxiety, depression, and post-traumatic stress disorder scales were markedly more likely to use opioids after surgery, regardless of injury severity or fracture site. These findings are important because orthopaedic surgeons need to understand not only their patients' physical status but also their psychological aptitude to provide them with appropriate care.
Substance use disorder was also found to be a large risk factor of prolonged opioid use. Similar to prior research, this finding is not unique to the shoulder. In lower extremity fracture cases, Cunningham et al19 found that those who have alcohol abuse required increased perioperative opioids. Cannabis use was not definitive, as studies vary on its influence. For example, there was no increased risk seen in hip arthroscopy patients20 while lumbar spinal fusion patients had an increased risk.21
The greatest risk factor our study found for prolonged opioid use was opioid familiarity before revision TSA. This finding was expected because there has been a plethora of research showcasing how preoperative opioid use increases a patient's risk postoperatively. Armaghani et al found this in spine surgery,22 Berglund et al described this in shoulder arthroplasty patients,23 and Smith et al24 showcased this after total knee arthroplasty. Our study builds on this literature by providing additional support in revision TSA patients.
Overall, our study showcased a multitude of risk factors that have the potential to prolong opioid use after revision TSA. Previous studies have assessed risk factors of prolonged opioid use after primary TSA,12,13,25 but research is limited on revision TSA. Surgeons can use this information to tailor preoperative patient education related to the risks of prolonged opioid use after surgery in those undergoing revision TSA. Future research can be directed toward assessing a more detailed breakdown of substance use disorders to better determine which ones are associated with the greatest risk of increased opioid use.
This study was not without limitations. Owing to the inherent limitations of PearlDiver, the extracted data have the potential for coding errors. Aside from this, preoperative opioid use may be due to other health issues, which can affect outcomes. Our study was limited by the general CPT codes used, and as a result, we were unable to differentiate risk factors of individual causes of TSA revisions. In addition, the PearlDiver database only contains data from the United States and, as a result, may not be applicable globally. Next, we are unable to control for postoperative physical therapy, which may influence outcomes due to improved function. Finally, we assumed that filling opioid prescriptions indicated use; however, we cannot determine whether patients consumed the medications.
ConclusionOlder age and male sex were associated with a decreased risk of prolonged opioid use after revision TSA. Depression, substance use disorder, opioid familiarity, and COPD were associated with prolonged opioid use after revision TSA.
References 1. Lyden J, Binswanger IA: The United States opioid epidemic. Semin Perinatol 2019;43:123-131. 2. Castle JP, Jildeh TR, Buckley PJ, Abbas MJ, Mumuni S, Okoroha KR: Older, heavier, arthritic, psychiatrically disordered, and opioid-familiar patients are at risk for opioid use after medial patellofemoral ligament reconstruction. Arthrosc Sports Med Rehabil 2021;3:e2025-e2031. 3. Morris BJ, Mir HR: The opioid epidemic: Impact on orthopaedic surgery. J Am Acad Orthop Surg 2015;23:267-271. 4. Rao AG, Chan PH, Prentice HA, Paxton EW, Funahashi TT, Maletis GB: Risk factors for opioid use after anterior cruciate ligament reconstruction. Am J Sports Med 2019;47:2130-2137. 5. Jildeh TR, Taylor KA, Khalil LS, et al.: Risk factors for postoperative opioid use in arthroscopic meniscal surgery. Arthroscopy 2019;35:575-580. 6. Kim SC, Choudhry N, Franklin JM, et al.: Patterns and predictors of persistent opioid use following hip or knee arthroplasty. Osteoarthritis Cartilage 2017;25:1399-1406. 7. Sanchez-Sotelo J: Total shoulder arthroplasty. Open Orthop J 2011;5:106-114. 8. Guareschi AS, Eichinger JK, Friedman RJ: Patient outcomes after revision total shoulder arthroplasty in an inpatient vs. outpatient setting. J Shoulder Elbow Surg 2023;32:82-88. 9. Favard L: Revision of total shoulder arthroplasty. Orthop Traumatol Surg Res 2013;99:S12-S21. 10. Boddapati V, Fu MC, Schairer WW, Gulotta LV, Dines DM, Dines JS: Revision total shoulder arthroplasty is associated with increased thirty-day postoperative complications and wound infections relative to primary total shoulder arthroplasty. HSS J 2018;14:23-28. 11. Rao AG, Chan PH, Prentice HA, et al.: Risk factors for postoperative opioid use after elective shoulder arthroplasty. J Shoulder Elbow Surg 2018;27:1960-1968. 12. Khazi ZM, Lu Y, Patel BH, Cancienne JM, Werner B, Forsythe B: Risk factors for opioid use after total shoulder arthroplasty. J Shoulder Elbow Surg 2020;29:235-243. 13. Best MJ, Harris AB, Bansal A, Huish E, Srikumaran U: Predictors of long-term opioid use after elective primary total shoulder arthroplasty. Orthopedics 2021;44:58-63. 14. Yang S, Werner BC: Risk factors for prolonged postoperative opioid use after spinal fusion for adolescent idiopathic scoliosis. J Pediatr Orthop 2019;39:500-504. 15. Jamison RN, Butler SF, Budman SH, Edwards RR, Wasan AD: Gender differences in risk factors for aberrant prescription opioid use. J Pain 2010;11:312-320. 16. Serdarevic M, Striley CW, Cottler LB: Sex differences in prescription opioid use. Curr Opin Psychiatry 2017;30:238-246. 17. Back SE, Lawson KM, Singleton LM, Brady KT: Characteristics and correlates of men and women with prescription opioid dependence. Addict Behav 2011;36:829-834. 18. Mohan S, Lynch CP, Cha EDK, et al.: Baseline risk factors for prolonged opioid use following spine surgery: Systematic review and meta-analysis. World Neurosurg 2022;159:179-188.e2. 19. Cunningham DJ, LaRose MA, Gage MJ: Impact of substance use and abuse on opioid demand in lower extremity fracture surgery. J Orthop Trauma 2021;35:e171-e176. 20. Wood JT, Sambandam S, Wukich DK, McCrum CL: Self-reported cannabis use is not associated with increased opioid use or costs after hip arthroscopy. Arthroscopy 2022;38:2227-2231.e4. 21. Moon AS, LeRoy TE, Yacoubian V, Gedman M, Aidlen JP, Rogerson A: Cannabis use is associated with increased use of prescription opioids following posterior lumbar spinal fusion surgery. Glob Spine J 2022:219256822210998. 22. Armaghani SJ, Lee DS, Bible JE, et al.: Preoperative opioid use and its association with perioperative opioid demand and postoperative opioid independence in patients undergoing spine surgery. Spine 2014;39:e1524-e1530. 23. Berglund DD, Rosas S, Kurowicki J, Horn B, Mijic D, Levy JC: Preoperative opioid use among patients undergoing shoulder arthroplasty predicts prolonged postoperative opioid use. J Am Acad Orthop Surg 2018;27:e691-e695. 24. Smith A, Smith NS, Smith LS, Yakkanti MR, Malkani AL: Does pre-operative opioid consumption influence patient satisfaction following total knee arthroplasty? J Knee Surg 2023;36:1374-1379. 25. Spencer CC, Pflederer JA, Wilson JM, Dawes AM, Gottschalk MB, Wagner ER: Opioid use following a total shoulder arthroplasty: Who requires refills and for how long? JSES Int 2021;5:346-352.
留言 (0)