
Remember me
Multidrug-resistant (MDR) bacteria, sometimes referred to as antimicrobial-resistant (AMR) bacteria, are a serious public health threat worldwide. Multidrug-resistant bacteria possess resistance to antibiotics either as a natural trait or through the acquisition of resistance over time. In other words, MDR bacteria are immune to the toxic effects of antibiotics. Therefore, infections caused by MDR organisms result in worse outcomes for patients. In 2019, MDR bacterial infections caused almost 5 million deaths globally, as estimated using a systematic analysis.1 In addition to being associated with a high mortality rate, MDR bacteria impose a significant financial burden on health-care systems. For instance, in the United States, the annual treatment cost of MDR bacterial infections was estimated to be 21–34 billion dollars.2
A large number of bacterial strains are becoming less susceptible or non-susceptible to commercially available antibiotics. The World Health Organization (WHO) has recently issued a list of critical pathogens that exhibit high resistance to antibiotics. The list is classified into 3 priority levels based on critical demand for new antibiotics, as follows: critical, high, and medium (Table 1; WHO). The decrease in the number of newly discovered antibiotics and the increasing number of resistant bacteria have urge the scientific community to search for alternatives to resolve this public health threat. Bacteriophages exhibit therapeutic potential against bacterial infections, including those caused by MDR bacteria.3 Numerous bacteriophages have been examined for their antibacterial effects against MDR bacteria in animals and humans.4
Table 1- Classification of priority pathogens based on their urgent need for new antibiotics (World Health Organization, 2017).
This review focuses on MDR strains, including gram-negative and gram-positive bacteria, and their mechanisms of antibiotic resistance. It then examines the therapeutic potential of bacteriophages against infections caused by MDR bacterial strains. It includes in vitro, in vivo, and human studies published in the last decade. In addition, it investigates the antibiofilm effect of lytic phages against biofilms produced by MDR strains.
Multidrug-resistant bacteriaOne of the critical (priority 1) organisms is Acinetobacter baumannii (A. baumannii) (Table 1). Acinetobacter baumannii is a gram-negative bacillus primarily associated with health care-acquired infections.5 In recent years, MDR A. baumannii has attracted global attention owing to its ability to resist most first-line antibiotics.5Acinetobacter baumannii is defined as MDR when the pathogen resists at least 3 antibiotic classes (penicillins and cephalosporins, including inhibitor combinations, fluroquinolones, and aminoglycosides) and as extensively drug resistant (XDR) when it is resistant to more than 3 classes of antibiotics and to carbapenems. It is defined as pan drug-resistant (PDR) when it is resistant to all the above mentioned antibiotics, polymyxin, and tigecycline.6,7
Pseudomonas aeruginosa (P. aeruginosa) is another organism classified as critical (priority 1) by the WHO (Table 1). It is an opportunistic human pathogen that normally does not cause infection in healthy individuals. However, it can cause life-threatening infections in immunocompromised people such as those with severe burns, organ transplants, cystic fibrosis, and cancer.8 The management of P. aeruginosa infections has become difficult due to the rise in the quantity of isolates that are resistant to antibiotics.9 Several studies have reported that clinical isolates of P. aeruginosa exhibit resistance to a substantial number of commercially available antibiotics.10-13 Extensive and pan drug resistance have also been reported.14,15 For instance, Fernandes et al16 reported several MDR P. aeruginosa isolates, including one that was resistant to all commercially available antibiotics.
Methicillin-resistant Staphylococcus aureus (MRSA) is a gram-positive coccus that is resistant to most available antibiotics.17 Most MRSA infections are health-care-associated MRSA (HA-MRSA) infections. In other words, people who have been hospitalized are at risk of MRSA infections.17 However, they can also manifest within the broader community, in which case they are referred to as community-associated MRSA.16 Community-associated MRSA infections usually spread through skin-to-skin contact in crowded places such as schools, daycare centers, and gyms.18
Mechanisms of antibiotic resistanceThe mechanisms of antibiotic resistance vary among resistant bacteria. For instance, A. baumannii avoid the toxic effects of antibiotics through several resistance mechanisms (Figure 1). First, it prevents antibiotic access into bacterial cells by reducing outer membrane permeability by down regulating the expression of porins, which results in a less permeable membrane. Second, using efflux pumps, A. baumannii pumps antibiotics out of their cells, thus preventing the toxic effects of antibiotics. Third, A. baumannii has genetic plasticity that allows rapid genetic mutations. Fourth, A. baumannii is capable of forming biofilms, which increases antibiotic tolerance.20
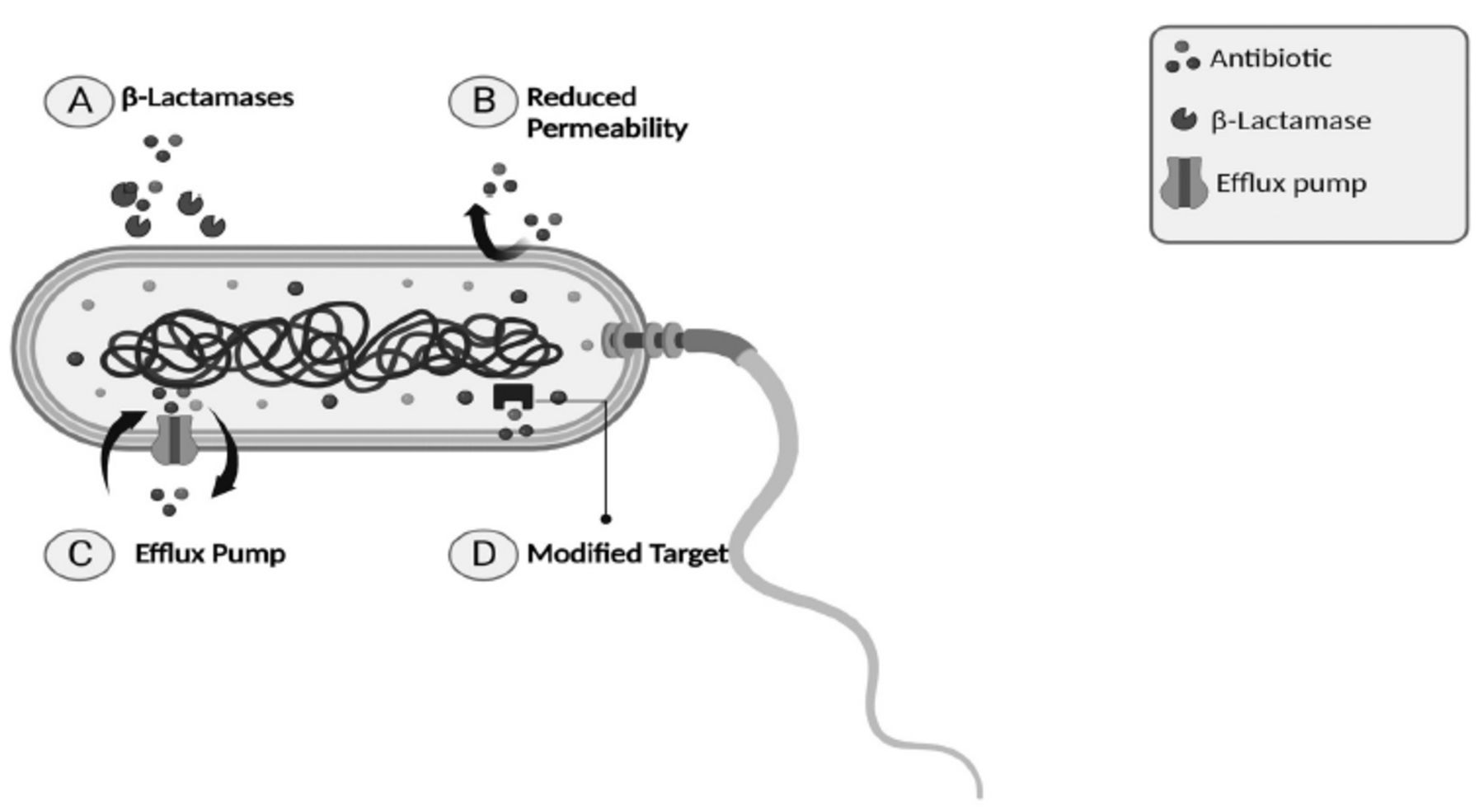 Figure 1
Figure 1 - Mechanisms of antibiotic resistance in Acinetobacter (A. baumannii). Resistance can be conferred in A. baumannii through four main mechanisms; A) producing β-Lactamases that degrade the β-lactam ring; thus, inactivating β-lactam antibiotics. B) Preventing access to antibiotics into the bacterial cell through reducing the outer membrane permeability. C) Pumping antibiotics out of the bacterial cell using efflux pumps. D) Modifying antibiotic’s target via genetic mutations; thus, antibiotic is no longer able to bind to its target.
BacteriophagesBacteriophages, often referred to as phages, are viruses that exclusively target and kill bacteria without harming human cells. For this reason, scientists have studied bacteriophages as antibacterial agents since their discovery in 1915.4,20 Bacteriophages were discovered by an English physician, Frederick Twort, when he observed for the first time cleared spots on his bacterial plates. Those clear spots were, in fact, dead bacteria lysed by the killing effects of phages. Two years later, in 1917, Felix d’Herelle published a similar observation. He suggested that these cleared spots were due to the lytic effect of phages.20
In 1919, for the first time, 4 pediatric patients with bacterial dysentery were successfully treated with bacteriophages at des Enfants-Malades hopital in Paris. Since then, phage therapy has been widely utilized, mainly in the Soviet Union and Eastern Europe.20
However, once antibiotics were discovered in the 1940s, the western world overlooked phage therapy.3 The newly discovered drug (antibiotics) was an ideal antibacterial agent until the rise of antibiotic-resistant pathogens during the 1980s.3 Since then, phages have attracted attention from the scientific community and have been rediscovered by western medicine as an alternative agent to combat antibiotic-resistant pathogens.3
Efficacy of bacteriophages against MDR bacteriaIn vitro/in vivo studies. Owing to the increasing number of MDR bacteria, researchers have reconsidered the use of phage therapy to overcome MDR organisms.1,3 The efficacy of phage therapy against resistant bacteria to most, if not all, commercially available antibiotics has been extensively studied not only in vitro and in vivo but also in humans.4,21,22
Numerous in vitro and in vivo studies have shown a potent antibacterial effect of bacteriophages against MDR bacteria, as summarized in Tables 2 and Tables 3. The efficacy of phage therapy was evaluated against various genera of MDR bacteria, including A. baumannii, which is significantly difficult to treat using standard antibiotics.5 Studies have shown that phage therapy is highly effective against MDR A. baumannii, including carbapenem- and colistin-resistant isolates.23,24 Zhou et al24 compared the therapeutic effect of 2 bacteriophages and polymyxin B against carbapenem-resistant A. baumannii. Using the Galleria mellonella larva model, the study demonstrated that phage therapy increased the survival of larvae infected with A. baumannii by up to 75%.24 By contrast, polymyxin B increased the survival of larvae infected with A. baumannii by only 25%.24 Another study assessed the killing effect of bacteriophages against colistin-resistant A. baumannii.23 The study reported a substantial decrease in the number of colistin-resistant A. baumannii after only 40 minutes of a single phage treatment.23 Phage treatment was also effective against XDR A. baumannii strains. Wang et al25 assessed the killing efficacy of ϕkm18p phage against XDR A. baumannii. The study showed that mono-phage treatment of mice infected with XDR A. baumannii significantly increased survival by up to nearly 100%.The antibacterial activity of bacteriophages against MDR P. aeruginosa was also evaluated in in vitro and in vivo studies.26 On the basis of these studies, bacteriophages have a potent killing activity against MDR P. aeruginosa. For instance, studies have tested phage cocktail against colistin-resistant P. aeruginosa.26,27 Three phages (Psu1, Psu2, and Psu3) completely lysed the bacterial cells of colistin-resistant P. aeruginosa.26 Another study investigated the antibacterial activity a lytic phage named as vB_PaeM_LS1 against clinical P. aeruginosa isolates, including MDR strains. Phage vB_PaeM_LS1 exhibited potent antibacterial activities against MDR and non-MDR P. aeruginosa isolates.27
Table 2- In vitro studies using bacteriophages or its derived enzymes against MDR bacteria.
Table 3- In vivo studies using phage therapy against MDR bacteria.
Phage therapy is effective not only against infections caused by gram-negative bacteria but also against those caused by gram-positive bacteria, such as MRSA.28-31 Numerous studies have demonstrated the therapeutic effect of bacteriophages against MRSA infections.28,30 For instance, Takemura-Uchiyama et al29 carried out a preclinical study using a mouse model of lung-derived septicemia to evaluate the efficacy of phage S13¢ against hospital-acquired MRSA isolates. In mice infected with MRSA, phage S13¢ was intraperitoneally administered 6 hours (h) after infection.29 The study showed that phage S13¢ rescued the mice infected with a lethal dose of MRSA.29 The phage-treated mice had significantly higher survival rates than the untreated mice on day 5 (67% vs. 10%).29 These results suggest that S13¢ is capable of rescuing mice from a lethal dose of MRSA.29 However, phage S13¢ was administrated at an early stage of lung infection in mice, 6 h post infection. This raises a question whether phage administration at a later stage of infection would obtain a similar outcome. More studies are needed to address this question.
Although bacteriophages are effective for killing MDR strains, bacteriophages are large structures that are likely to induce harmful immune responses.32 To overcome this challenge, instead of using intact phages, part of the phage components can be utilized as an antibacterial agent. For instance, endolysins are phage-encoded enzymes that digest the cell wall of either gram-positive or gram-negative bacteria.33 However, the killing efficacy of endolysins is more effective in gram-positive bacteria because the peptidoglycan layer is exposed.33 In gram-negative bacteria, the peptidoglycan layer is surrounded by an outer membrane layer, which reduces the accessibility of the targets of many endolysins.33 One approach to increase the therapeutic effect of endolysins is by using them in combination with antibiotics. Blasco et al33 assessed the therapeutic effects of endolysin ElyA1 and colistin against MDR A. baumannii. The researchers demonstrated that the combination of endolycin ElyA1 and colistin increased the survival of larvae infected with MDR A. baumannii and decreased the bacterial load in the skin and lungs of mice infected with MDR A. baumannii.33 However, the combination therapy of endolycin ElyA1 and colistin had no antimicrobial effects on colistin-resistant A. baumanni isolates. This is probably due to the enzyme’s failure to reach the peptidoglycan layer.34 Thus, endolysins alone may not be the suitable choice to tackle MDR bacteria.
Human studiesIn addition to the in vitro and in vivo studies of the efficacy of bacteriophages against bacterial isolates, studies have also been carried out to test the effectiveness of phage therapy in humans. Over the last decade, numerous case reports and clinical trials of phage therapy have been carried out, as summarized by Liu et al.22 Most clinical studies of phage therapy utilized a combination treatment of bacteriophages and antibiotics to target various pathogens, including MDR isolates.22 The available literature data have shown that bacteriophages are potent therapeutics in treating various bacterial infections such as bacteremia, urinary tract infections (UTIs), surgical site infections (SSIs), diabetic foot ulcers, brain infections, corneal abscesses, lung transplant-related infections, aortic graft infections, pancreatitis, otitis, burn wounds, and diarrheal diseases.22,39
The most important question is whether the potent efficacy of bacteriophages against MDR bacteria that been shown in in vitro and in vivo models applies in humans. According to the published data, the use of bacteriophages in humans indicated a potent therapeutic effect against infections with various MDR isolates, including but not limited to, A. baumannii, P. aeruginosa, MRSA, and Klebsiella pneumoniae (K. pneumoniae) (Table 4). A phage cocktail approach seems to be the most effective way to overcome MDR pathogens, as shown by several human studies (Table 4). For instance, LaVergne et al40 reported the efficacy of phage therapy in treating MDR A. baumannii. A 77-year-old patient who had undergone craniotomy had SSI with MDR A. baumannii. The isolate was resistant to all tested antibiotics. Initially, the patient was treated with a combination of 3 antibiotics: colistin, azithromycin, and rifampin. However, no clinical improvement was observed. Therefore, a phage cocktail was administered intravenously. After a total of 98 doses of bacteriophages, no signs of infection at the cranioctomy site were observed. In this study, there was no microbiological data after phage administration; thus, it cannot be concluded that phage therapy was successful.40 Further research is necessary to more thoroughly assess the effectiveness of phages.
Table 4- Case reports using phage therapy against MDR bacteria.
In another case study, Khawaldeh et al41 reported the use of phage therapy to treat a patient with UTI infection caused by P. aeruginosa. When the antibiotic treatment failed to cure the P. aeruginosa infection, a combination therapy with 6-lytic phages and antibiotics was administered. The patient was treated with the phage cocktail for 5 days, followed by meropenem and colistin for 2 days. Microbiological studies have shown that phage treatment caused a tenfold reduction of bacteria in urine. When antibiotic treatment was involved, no bacteria were detected in the urine samples. These results indicate that antibiotic treatment combined with phages completely cured UTI caused by P. aeruginosa.41
On the other hand, a few studies have reported negative outcomes associated with phage therapy.42-44 For instance, a 15-year-old diagnosed with cystic fibrosis and infected by drug-resistant mycobacterium abscessus underwent treatment with an intravenous mixture of 3 phages. On the second day of treatment, the patient exhibited diaphoresis and cutaneous flushing; nevertheless, there were no indications of fever or modifications in the results of the physical examination.43 Another study reported adverse events related to bacteriophages. Nine patients with UTI were treated with an adapted Pyo bacteriophage. All phage-treated patients had no phage-associated adverse effects except for one patient with P. aeruginosa infection. The patient had a sudden fever (38.5°C) and chills on the third day of phage therapy. Thus, the phage therapy was stopped, and cephalosporin was prescribed. The authors attributed the sudden increase in the patient’s temperature to the release of endotoxins during P. aeruginosa lysis.42 A recent study showed that of 9 patients with chronic rhinosinusitis caused by Staphylococcus aureus (S. aureus), 6 developed mild adverse effects after phage treatment, which were classified as treatment-emergent adverse effects such as diarrhea, epistaxis, oropharyngeal pain, cough, rhinalgia, and decreased blood bicarbonate levels.44
Efficacy of bacteriophages against biofilmsAnother major obstacle in treating bacterial infections is the ability of most bacteria genera, including MDR, to form biofilm structures. A biofilm is a population of microorganisms residing within a self-generated matrix composed of extracellular polymeric substances (EPSs). Extracellular polymeric substances are mainly composed of polysaccharides and proteins, lipids, and extracellular deoxyribonucleic acid. Within a biofilm, bacteria demonstrate greater protection from antibiotics and host immune defenses.50,51 A biofilm increases antibiotic resistance by up to 1000-fold.52 The significant increase in antibiotic resistance among biofilm cells is attributed to 2 factors. One factor is biofilm reducing antibiotic accessibility into biofilm cells. The biofilm matrix of EPS as a physical barrier prevents antibiotics from penetrating the EPS matrix.53 The other factor is biofilm cells that grow slowly and exhibit reduced metabolic activity; thus, the slow-growing cells are immune against antibiotics whose killing mechanisms require metabolically active cells.54
Treatment of biofilm-associated infections requires not only the inhibition of causative agents and bacteria but also the disruption of biofilm structures. One potential candidate for disrupting biofilms is bacteriophages. Bacteriophages exhibit potent activities against biofilm structures. As shown in Figure 2, bacteriophages can destroy bacterial biofilms through 2 strategies. First, bacteriophages penetrate bacterial biofilms and eradicate them. Second, endolysins and depolymerases, which are phage-derived enzymes, possess enzymatic activity against bacterial biofilms.55
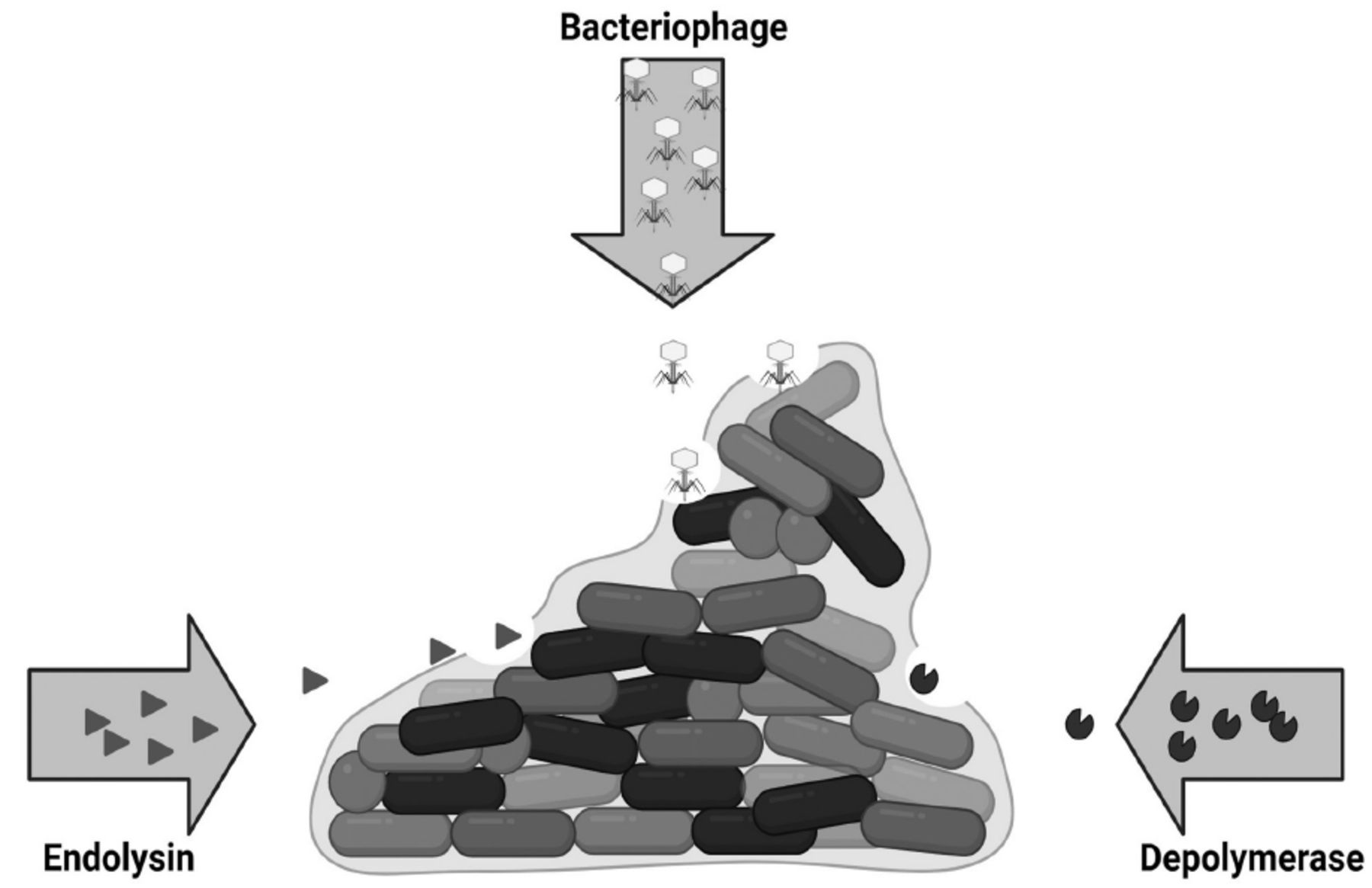 Figure 2
Figure 2 - Schematic representation of biofilm degradation by bacteriophages and its derived enzymes. Bacteriophages degrade bacterial biofilm by 3 mechanisms; (i) Phage-derived endolysins, which degrades bacterial cell walls. (ii) bacteriophages degrade bacterial cell walls and biofilm matrix. (iii) phage-derived depolymerases as free enzyme or tail spike protein degrade biofilm matrix.
Several studies have assessed the antibiofilm activity of phages against biofilm formed by MDR isolates (Table 5). Phages have shown antibiofilm effects against biofilms formed by various MDR isolates, including but not limited to MDR P. aeruginosa, MDR A. baumannii, MDR K. pneumoniae, MDR Escherichia coli, MDR S. gallinarum, and MRSA.56-61 For instance, a recent study by Adnan et al56 examined the efficacy of a bacteriophage (MA-1) against MDR P. aeruginosa biofilm. MA-1 resulted in a significant reduction of 2-fold in 24-h-old biofilms, 2.5-fold in 48-h-old biofilms, and 3.2-fold in 74-h-old biofilms developed by P. aeruginosa However, MA-1 had no effect on other P. aeruginosa isolates due to the phage’s limited host range.Further research is needed to assess the efficacy of a phage cocktail against biofilm developed by different isolates of P. aeruginosa.
Table 5- Studies of antibiofilm activity of bacteriophages on biofilms formed by MDR isolates.
Another study targeted biofilms formed by MRSA isolates with bacteriophage CSA13. A 24-h-old biofilm formed in a 96-well plate was treated with the bacteriophage CSA13. The phage eradicated 93.4% of S. aureus CCARM 3793 MRSA biofilms and 78.5% of S. aureus Newman (MSSR) biofilms. This result suggests that biofilm of MRSA strain is more susceptible to phages than that of developed by MSSR.61 However, It is important to confirm this finding with more research by comparing the susceptibility of biofilms developed by MRSA isolates versus biofilms developed by MSSA isolates.
A recent study combined bacteriophage cocktails consisting of 5 bacteriophages and antibiotics against biofilms of MDR A. baumannii. The study reported a significantly greater reduction of biofilm biomass when 24 biofilms were treated with a combined treatment (antibiotic + bacteriophage cocktail). The highest antibiofilm effect was observed when the bacteriophage cocktail was combined with trimethoprim/sulfamethoxazole, accounting for a 98.6% reduction of the biofilm biomass of A. baumannii. The study concluded that the combination of bacteriophage cocktails and some antibiotics has a synergistic effect against biofilms of MDR A. baumannii.57
Challenges of phage therapyAlthough phage therapy is a promising treatment for bacterial infections, particularly against MDR bacteria, it also comes with several challenges. One major challenge is selection of the right phage. There are 2 types of phages; lytic and temperate. Lytic phages immediately kill their bacterial hosts, while temperate, or lysogenic, phages integrate their genetic material into the host chromosome without killing their hosts. The concern of utilizing temperate phages in phage therapy is the possibility of transferring toxin or antibiotic resistant genes to their target bacterial.66,67 Another obstacle of phage therapy is the emerging of phage resistance. Similar to antibiotic resistance, bacteria are capable of developing resistance to phages. This can be achieved by a modification on bacterial cell surface.67,68 A study carried out by Le et al69 showed P. aeruginosa exhibited a mutation in galU after exposure to lytic phage. GalU is a gene necessary for the production of LPS. Administration of phage is not straightforward as well. Unlike antibiotics, phages are self-replicating organisms; meaning the concentration of a phage mixture given to a patients may not be the exact concentration they actually receive.67,68
In conclusion, MDR bacteria are a terrifying major health issue worldwide. Infections caused by MDR bacteria are difficult to treat with conventional treatments (antibiotic therapies). The available antibiotics are becoming less or even ineffective in inhibiting MDR isolates. The golden age of antibiotics appears to have come to an end, and a post-antibiotic era is about to commence. Thus, the clinical and economic impacts of MDR bacteria necessitate the search for alternative antibacterial agents. One alternative is bacteriophages. They are the most ubiquitous organisms in the universe.70 Scientific studies have demonstrated the potent efficiency of bacteriophages and bacteriophage-derived enzymes against MDR bacteria not only in in vitro models but also in in vivo models and humans, as described earlier. Besides their efficacy against MDR bacteria on planktonic form, bacteriophages have also demonstrated an antibiofilm effect against biofilms of MDR isolates (Table 5).
According to the existing literature, the most effective strategy to overcome antibiotic-resistant bacteria is by a combination treatment consisting of a phage cocktail and antibiotics (Tables 3 & 4). However, more investigations are required to evaluate the side effects of phage therapy, such as toxicity and unwanted immune response. In addition to conducting more studies on phage therapy, the scientific community should implement suitable regulations for the clinical use of phage therapy to accelerate the process of eradicating MDR bacteria.
Comments (0)