
記住我


Available online 28 November 2023, 107589
 Author links open overlay panel, , , , , , , , ABSTRACTBackground
Author links open overlay panel, , , , , , , , ABSTRACTBackgroundmyocardial adaptation to severe aortic stenosis (AS) is a complex process that involves myocardial fibrosis (MF) beyond cardiomyocyte hypertrophy. Perfusion impairment is believed to be involved in myocardial remodeling in chronic pressure overload.
Aimto describe morphological and ultrastructural myocardial changes at endomyocardial tissue sampling, possibly reflecting subendocardial ischemia, in a group of patients with severe AS referred to surgical aortic valve replacement (AVR), with no previous history of ischemic cardiomyopathy.
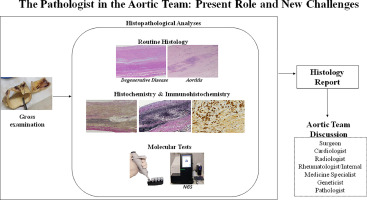
Methodsone-hundred-fifty-eight patients (73 [68-77] years, 50% women) referred for surgical AVR because of severe symptomatic AS with pre-operative clinical and imaging study and no previous history of ischemic cardiomyopathy. Intra-operative septal endomyocardial sampling was obtained in 129 patients. Tissue sections were stained with Masson´s Trichrome for MF quantification and periodic acid-Schiff (PAS) staining was performed to assess the presence of intracellular glycogen. Ultrastructure was analyzed through Transmission electron microscopy (TEM).
ResultsMF totalized a median fraction of 11.90% [6.54-19.97%] of EMB, with highly prevalent perivascular involvement (95.3%). None of the samples had histological evidence of myocardial infarction. In 58 patients (45%) we found subendocardial groups of cardiomyocytes with cytoplasmatic enlargement, vacuolization and myofiber derangement, surrounded by extensive interstitial fibrosis. These cardiomyocytes were PAS positive, PAS-diastase resistant and Alcian Blue/PAS indicative of the presence of neutral intracellular glyco-saccharides. At TEM there were signs of cardiomyocyte degeneration with sarcomere disorganization and reduction, organelle rarefaction but no signs of intracellular specific accumulation.
Conclusionalmost half of the patients with severe AS referred for surgical AVR have histological and ultrastructural signs of subendocardial cardiomyocyte ischemic insult. It might be inferred that local perfusion imbalance contributes to myocardial remodeling and fibrosis in chronic pressure overload.
Section snippetsINTRODUCTIONCalcific aortic stenosis (AS) is the most common valvular heart disease, characterized by a chronic increase in the hemodynamic load to the left ventricle (LV) [1]. LV adaptation in this setting plays an important role for the occurrence of symptoms, heart failure development and definition of prognosis [2]. Myocardial fibrosis (MF) is an important component of LV remodeling, driving the transition from hypertrophy to heart failure [3] However, the mechanisms behind this transition are not
Study population and study designWe prospectively evaluated one-hundred-fifty-eight patients undergoing surgical AVR at our tertiary center between April 2019 and January 2022 because of isolated severe symptomatic AS, defined according to European guidelines on valvular heart disease [8], with no previous history of myocardial infarction and ischemic cardiomyopathy. Detailed exclusion criteria are described at Supplementary data online, Material/Methods.
This prospective study is part of a larger correlation research protocol
Clinical and surgery related dataFrom a total of 158 patients included, median age of 73 [68-77] years, 79 (50%) of them being women, 143 were submitted to elective surgical AVR because of severe symptomatic AS. The classical echocardiographic phenotype of high gradient, normal flow, and preserved LV ejection fraction (EF) was predominant (136 patients, 86%, mean LV EF: 58.2± 9.2%), despite sub-normal mean global longitudinal strain. At preoperative CMR, non-ischemic late gadolinium enhancement (LGE) was identified in 106
DISCUSSIONThe main novel finding of our study is that a significant proportion of patients with severe symptomatic AS have histological and ultrastructural myocardial changes described in chronic ischemic conditions, such as chronic myocardial hibernation. As these occur in a cohort of patients with no previous history of ischemic cardiomyopathy, one might deduce that local perfusion impairment contributes to myocardial remodeling in chronic pressure overload.
To the best of our knowledge, we are first
LIMITATIONSAs a single observation in time this study has limitations. It represents a snapshot assessment of what has been happening in the myocardium from the beginning of aortic valve disease and we inferred functional changes from morphological assessment. As patients are referred to our institution for surgical AVR, we did not evaluate or had access to data concerning the length of time from the beginning of symptoms or clinical indication for surgery, as this could have interfered with LV adaptation
CONCLUSIONSA proportion of patients with severe AS referred for surgical AVR have signs of subendocardial cardiomyocyte ischemic insult, as assessed by histomorphology and ultrastructural myocardial changes. In chronic pressure overload from AS, cardiomyocyte adaptation and hypertrophy may elapse with local perfusion impairment, which could determine myocardial remodeling and fibrosis.
Declaration of Competing InterestNone to declare (on behalf of all authors)
ACKNOWLEDGEMENTSThe authors would like to thank to the Pathology Technicians, Maria Leonor Jacinto from Pathology Department, Hospital de Santa Cruz, Centro Hospitalar de Lisboa Ocidental, Mariana Barbosa, from Pathology Department, Hospital Fernando Fonseca, and Fernanda Silva, from Pathology Department, IPOFG, Lisboa and iNOVA4Health, Nova Medical School, Faculdade de Ciências Médicas, Universidade NOVA de Lisboa.
FUNDINGNothing to declare
AUTHOR CONTRIBUTION STATEMENTAll authors have contributed to this manuscript, reviewed, and approved the current form of the manuscript. JA was specifically responsible for manuscript conceptualization. SM RRS and PL were responsible for data collection, analysis and first manuscript edition. RT, SR and AF provided complete pathology assessment. NC, SR and AF specifically made the first revision and editing.
REFERENCES (31)J Ausma et al.Chronic ischemic viable myocardium in man: Aspects of dedifferentiationCardiovasc Pathol
(1995)
D Natarajan et al.Aortic stenosis - pathogenesis, prediction of progression, and percutaneous interventionJournal of the Royal College of Physicians of Edinburgh
(2017)
N Ajmone Marsan et al.Valvular heart disease: shifting the focus to the myocardiumEur Heart J
(2023)
MD Cheitlin et al.The distribution of fibrosis in the left ventricle in congenital aortic stenosis and coarctation of the aortaCirculation
(1980)
TA Treibel et al.Reappraising myocardial fibrosis in severe aortic stenosis: An invasive and non-invasive study in 133 patientsEur Heart J
(2018)
View full text© 2023 Elsevier Inc. All rights reserved.
留言 (0)