
Remember me

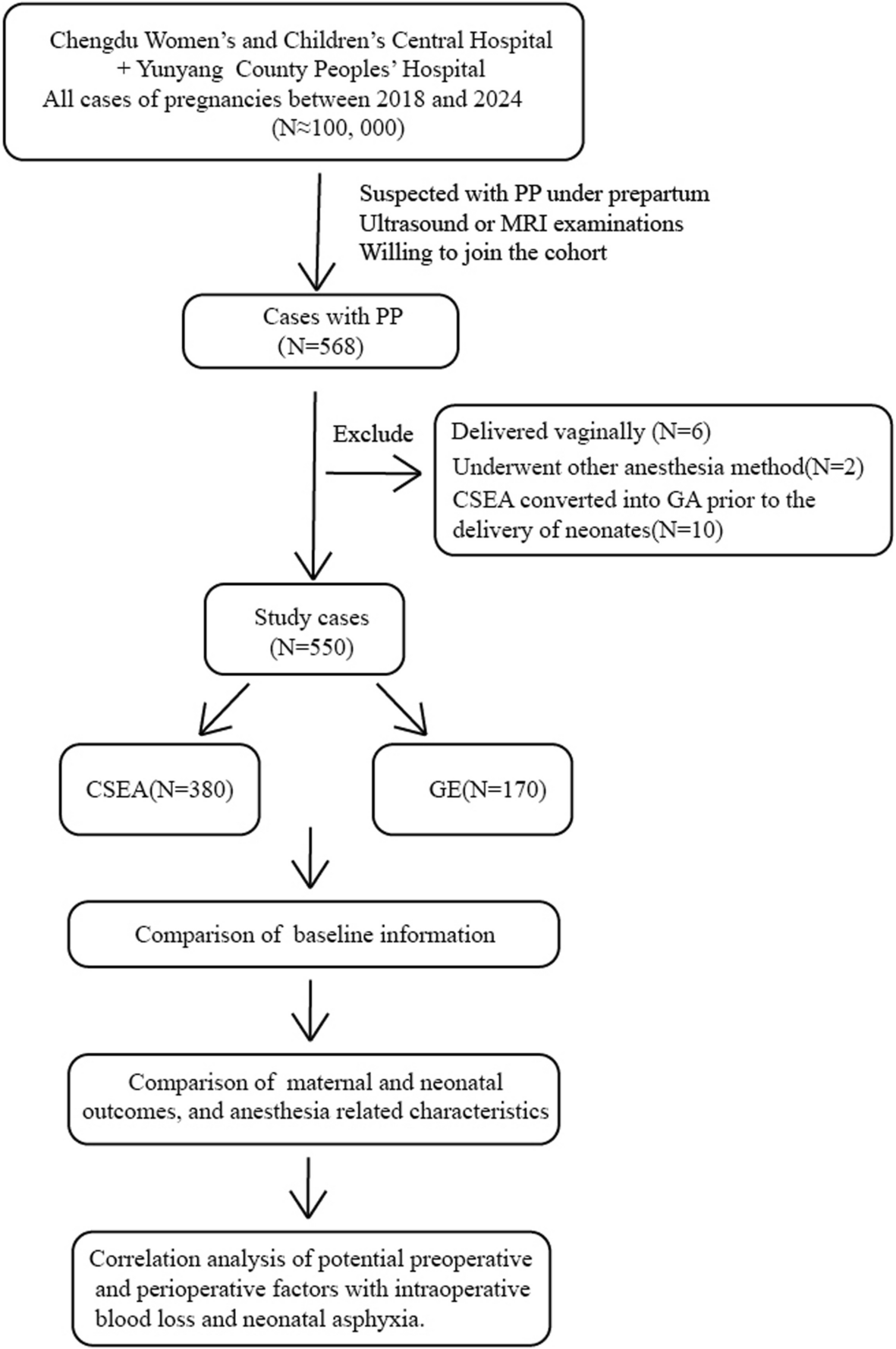





The study conformed to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of The Second Affiliated Hospital of Xuzhou Medical University ([2022] 052501), and this study was registered with the Chinese Clinical Trial Testing Center (ID: ChiCTR2200062400,04.08.2022). Written informed consent was obtained from all the subjects participating in the trial. The study plan was to enroll patients beginning in June, but patients were actually recruited between August 2022 and December 2022 after clinical registration. Inclusion criteria: ① Patients with an imaging diagnosis of hip fracture; ② Age ≥60 years old; ③ Dynamic NRS scores ≥4 points; ④ BMI: 18-30 kg/m2. Exclusion criteria: ① Patients with allergies to the drug used in this experiment; ② Patients with local or systemic infection; ③ Patients with coagulopathy; ④ Patients with severe cardiopulmonary insufficiency; ⑤ Patients with a history of ipsilateral hip surgery; ⑥ Patients with mental, language, communication, or hearing impairment; ⑦ Patients who refused to participate in this trial; ⑧ Patients with multiple systemic injuries.
Randomization, blinding and study interventionA nurse not involved in the study used Excel to generate a random integer set of 1-41, odd number into group F and even number into group P. These random numbers were placed in sealed opaque envelopes, and the anesthesiologist experienced in performing pericapsular nerve group block conducted the trial intervention. Group P received ultrasound-guided PENG block with 20 mL of 0.375% ropivacaine) and Group F received intravenous flurbiprofen 50 mg. In this study, a resident anesthesiologist who was unaware of the randomization assignment collected the data. Another member of this group who was blinded to the other steps of this test performed statistical analysis and remained blinded throughout the entire process.
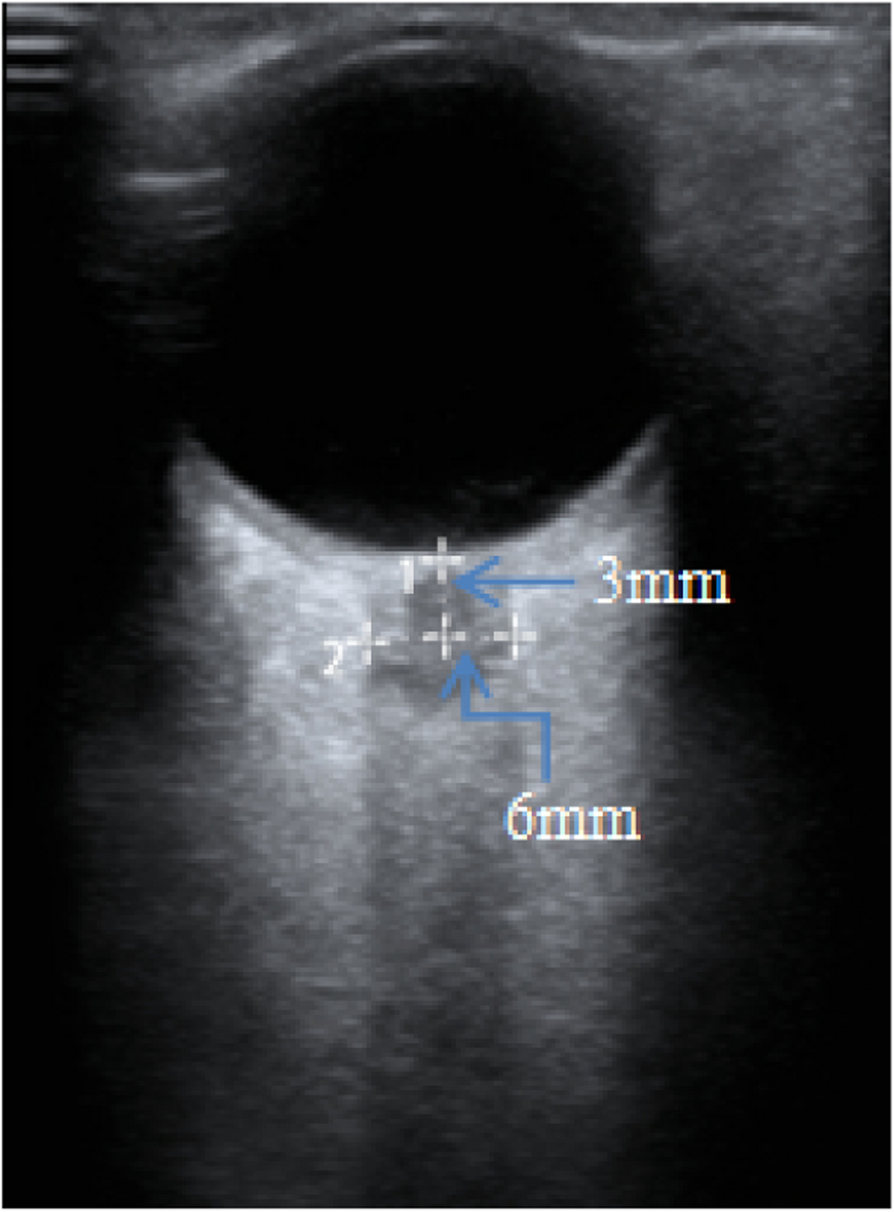
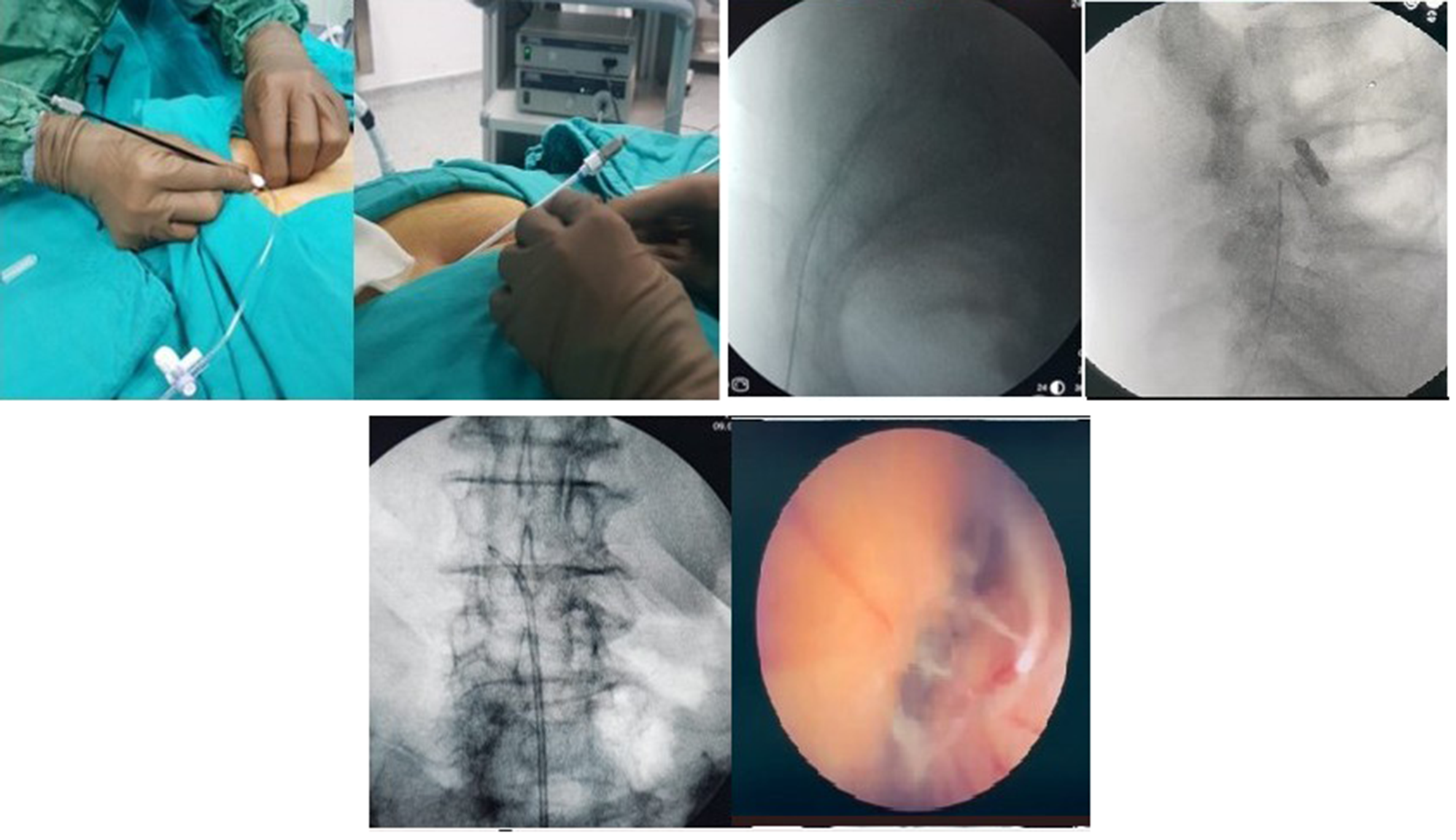
Patients in the group P received the PENG block as described by Girón-Arango [11]. The regional block was performed with the patient in the supine position. A curvilinear low-frequency ultrasound probe (2-6 MHz, Sonosite) was initially placed in a transverse plane over the anterior inferior iliac spine and then aligned with the pubic ramus by rotating the probe counterclockwise approximately 45 degrees. The iliopsoas eminence, the iliopsoas muscle and tendon, the femoral artery, and the pectineus muscle were observed. A 22G puncture needle was inserted from lateral to medial in an in-plane approach to place the tip in the musculofascial plane between the psoas tendon anteriorly and the pubic ramus posteriorly. Following negative aspiration, 2 mL of normal saline was injected to identify the correct location of the tip, followed by an injection of 20 mL of 0.375% ropivacaine (Naropin, AstraZeneca, eg, Fig. 1). Patients in the group F received intravenous 50 mg of flurbiprofen.
Fig. 1
Representative image and ultrasound scan of patient receiving PENG block. Notes: White arrow is ultrasound-guide tracing of puncture needle; * Iliopsoas tendon is marked. Abbreviations: PENG, pericapsular nerve group; AIIS, anterior inferior iliac spine; IPE, iliopubic eminence; FA, femoral artery; LA, local anesthetics
After those with contraindications were excluded, both groups received analgesia (Ultrasound-guided PENG block or intravenous flurbiprofen) as soon as possible after admission. When the NRS scores≥ 4 at rest after analgesia, the patients recevied intramuscular 5 mg dezocine as rescue analgesia. Dezocine was used repeatedly, if required, with dosing intervals of no less than 6 hours.
Outcome measuresThe basic information of all the patients was collected, including the static and dynamic NRS scores after the intervention. In addition, we collected pulse oxygen saturation (SpO2), mean arterial pressure (MAP), and heart rate (HR). The primary outcome was dynamic NRS scores (passive straight leg raising 15°) at 15 min, 30 min, 6 h, 12 h, and 24 h after the intervention. Secondary outcomes were static NRS score at 15 min, 30 min, 6 h, 12 h, and 24 h after the intervention, the highest NRS scores and number of rescue analgesics at 0-12 h and 12-24 h, the incidences of nausea, vomiting, bleeding at the puncture site, hematoma, and local anesthetic poisoning reaction within 24 h. Within 24 h after the intervention, overall satisfaction was scored on the VAS in which scores range from 0 to 10, with 0 indicating ‘not satisfied’ and 10 indicating ‘most satisfied’. If the patient slept between 23:00 and 7:00, we thought the pain was mild at this time, so the mean static NRS score was 1.5 points, thus indicating mild pain and the maximum dynamic NRS score was 3 points, also indicating mild pain.
NRS scores at 30 min is 30 min after the intervention, with the NRS score at this moment unrelated to the other interventions, and this same is also true for NRS scores at 6 h, 12 h, 24 h.
Statistical analysisThe sample size was determined to be sufficient through calculations using the GPower 3.1.1 computer program software. The power analysis indicated that a total of 34 participants, including a 15% dropout rate (number of measurements = 6), were needed for a medium partial η2 (0.25) when α = 0.05 for a power of 0.95 with 2 independent groups, using a repeated measures analysis of variance (ANOVA) and within-between subject interactions. A total of 38 participants, including a 15% dropout rate, were needed when the time before the intervention was not considered (number of measurements = 5).
The obtained data were analyzed with IBM SPSS Statistics 25 (IBM, Armonk, NY, USA). The parametric distribution of numerical variables was evaluated by the Shapiro–Wilk normality test. The Levene test was used to verify homogeneity. The normally distributed measures are denoted as the mean ± standard deviation (mean ±SD). The T test was applied to make independent comparisons between groups. Repeated measures ANOVA was used to analyze the repeated variables. Nonnormally distributed measures were expressed as the median and interquartile range (IQR) or marginal means from generalized estimation equations and standard deviation from raw data among persons with information at specific time points (mean ±SD)a. Mann‒Whitney U test or Generalized Estimation Equations for nonparametric continuous variables. In one patient with missing scores at 24 h, we did not interpolate. Moreover, the chi-square test or Fischer’s exact test was applied to compare categorical variables. A two-tailed P <0.05 was considered statistically significant.
Comments (0)