
記住我

The context in which teaching occurs has shifted dramatically.1,2 Blended learning, combining online and in-person teaching approaches, has taken on increasing prominence in the fields of higher and continuing education, improving access to learning for those with barriers to in-person learning, including those who wish to continue working while studying.3,4
For some time, master's level quality improvement (QI) education in health and social care has accommodated busy professionals with flexible options for learning. Curricular efforts in undergraduate and postgraduate clinical programs teaching QI have been extensively researched.5–9 Master's level programs specific to QI have only recently grown in number and maturity and are less well represented in the literature than undergraduate and postgraduate clinical programs.5–8 Although systematic reviews in this field continue to reveal general curricular attributes that associate to positive learner experience and impact on knowledge, skills, and attitudes, a recent review noted again that there is a paucity of detail on educational strategies to support replication.8 To understand more deeply how educators can effectively teach QI in a blended learning model, we studied faculty perspectives of an existing and successful program, which had already published data on learner impact.10,11
Beginning in 2009 and still running, the Jönköping Academy for Improvement of Health and Welfare (the Academy) at Jönköping University in Sweden offers an interprofessional master's program in QI and Leadership in health and welfare services. It seeks to bridge the theory–practice divide by creating a structure that ties the academic and practice environments together using a collaborative approach to both development and delivery of curriculum. A key design feature of the program is blended remote and face-to-face learning, to enable participation by working professionals who are encouraged to tie their studies to their workplace. Evaluations of learner experiences since 2009 show that students acquired improved leadership skills and felt their improvement efforts had a positive impact on their home health and social care systems, both at the point of service delivery and at the level of service design.10,11
To better understand which program conditions can support effective learning of QI and leadership competencies in a blended learning model, we undertook an in-depth study of the enacted curriculum from the point of view of program faculty. Distinct from the intended curriculum which is described by the policy frameworks and curricular guidelines, Porter and Smithson12 argued that “most learning is expected to occur within the enacted curriculum.” p.2 Brown used the metaphor of jazz, where the intended curriculum is the sheet music and the enacted curriculum is the interpreted performance, with the key being that different teachers will provide different renditions of the same piece.13 If the enacted curriculum is the dynamic space where learning occurs, then to understand the “how” of a given program, we must pay attention to faculty perspectives. The aim of our study was to identify and describe key features of the enacted curriculum that supported effective learning in the Jönköping Academy's Master's in Quality Improvement and Leadership program.
MATERIALS AND METHODSWe used a modified case study approach underpinned by an interactive research model. The overall case could be seen to include previously published studies of student outcomes and experience. Readers interested in a broader exploration of this program may read the previously published literature.10,11 Our focus was the enactment of a QI and leadership curriculum from faculty members' point of view in the context of the Academy's interprofessional master's program. Given the topic of the study and the nature of the participants, this study was exempted from institutional ethics review per the regional ethics review board.
In interactive research, we pursue a threefold task: (1) contribute meaningfully to practical concerns, (2) create new knowledge, and (3) learn together as research and practice systems interact through the course of a project.14 As with other forms of collaborative research, the distance between the researched and the researchers is often diminished.15,16 Specifically, BAG and JT participated as respondents and contributed to data collection, data interpretation, and writing. They and K.S. also served as faculty in the program.
ContextEstablished in 2009 and marked by the launch of its master's program, the Academy is based at Jönköping University (JU) in Jönköping, Sweden. Besides the master's program, the Academy attracts an active group of doctoral students and researchers and hosts the Centre for Coproduction. In 2010, the Academy had only a small core group of active faculty. Currently, there are over 15 faculty members and some 20 doctoral students, many of them former master's students.
Development and stewardship of the 3-year master's program initially involved all four schools at Jönköping University; the Region Jönköping County, responsible for health care services for all residents in the region; and the 13 municipalities responsible for social care within the same region. At its inception, additional partners included Linnaeus University in Växjö, Sweden, and the Dartmouth Institute for Health Policy and Clinical Practice in the United States.
Most Academy's master's students are practicing in health and social care. They include nurses (the single largest profession among students), physicians, occupational therapists, physiotherapists, social workers, administrators, engineers, psychologists, dentists, and communications and information technology professionals.
The program has its foundations in the Institute for Health care Improvement's Knowledge Domains17 and was developed with four design principles in mind: (1) action learning to link theory and practice, (2) interprofessional interaction, (3) blended learning, and (4) reflective practice. These design principles continue to be intentionally followed.
Individual courses in the first two years of the master's program require practical application of concepts that support improvement efforts in the students' professional practice setting. Those early improvement efforts form the basis for an interactive QI practicum, a research-based thesis project in that same setting, an approach inspired by the Dartmouth–Hitchcock Leadership Preventive Medicine Residency Program.18 For example, deep exploration of the student's work setting is required in one of the first courses, where the student is required to submit a paper that explores a local clinical microsystem's 5 Ps (purpose, people, patients, processes, and patterns), as outlined in a foundational course book.19
Study ParticipantsAll faculty involved in teaching and designing the initial offerings at the master's program, as well as faculty leaders involved in conceptualizing and designing the overall program, were invited to participate (n = 17). A total of 11 agreed. Although all 11 had roles in delivery of curriculum to some extent, two had primary roles that were in program leadership, four were involved in both program and course design and delivery, and five had roles in single course design and delivery only (CDD).
Procedure for Data Collection and AnalysisWe used document analysis, a focus group, individual interviews, and stimulated recall interviews. The primary author analyzed foundational documents, including program promotional materials and course syllabi. The 3-hour focus group was used to explore the participants' beliefs and thinking regarding how the program was meeting its intended objectives. Within the focus group, the participants themselves organized the data into themes. Six of the nine faculties who were teaching (program and course design and delivery & CDD) agreed to participate in semistructured individual interviews. As close as possible to the initial interview, where feasible, four stimulated recall interviews were held with those faculty. Table 1 summarizes the involvement of participants in the different phases of data collection.
TABLE 1. - Participation in Data Collection Methods by Faculty Role Method Participants* PL1 PL2 PCDD1 PCDD2 PCDD3 PCDD4 CDD1 CDD2 CDD3 CDD4 CDD5 Focus group X X X X X X X Interview X X X X X X Stimulated recall X X X X*PL, program leader; PCDD, program and course developer and designer; CDD, course developer and designer.
Stimulated recall is a collection of strategies designed to uncover thought processes and beliefs by anchoring interviews in observations of practice.20 In our study, we used stimulated recall to “make explicit and articulate the thinking, knowledge, theories, and beliefs that guided…teaching practice.” 21 Objects for stimulated recall included three video recordings of teaching sessions and one transcript of an online discussion. The focus of the stimulated recall interviews was to explore more specifically the faculty members' teaching strategies by observing an example of actual practice together. To manage the bilingual aspect of the interviews (K.S. spoke English as a first language and the respondents had varying degrees of fluency in English), K.S. translated any Swedish words during the interview to confirm understanding and had participants describe meaning where she could find no direct translation.
We used qualitative content analysis and data reduction, data display, and conclusion drawing to analyze our data.22 Owing to challenges in transcription resulting from the mixture of Swedish and English, K.S. coded all bilingual interviews directly from the audio recordings. The three interviews conducted exclusively in English were transcribed and then coded as text, using QSR NVivo 9 software. We used member checks (where the participants were able to review a summary of the interviewer's interpretation/translation) to confirm narrative accuracy when the person being interviewed was less fluent in English.
RESULTSWe analyzed data from multiple sources and grouped them into six themes as expressed in the enacted curriculum: (1) focusing on a common purpose, (2) developing technical and relational knowledge and skills, (3) linking theory and practice in the workplace, (4) leveraging collaboration for mutual benefit, (5) concentrating on leadership and coaching, and (6) applying a blended and interprofessional learning model (see Table 2 for representative quotations). These six themes mirror and expand on the four original program design principles.
TABLE 2. - Enacted Curriculum of a Master's Program in Quality Improvement and Leadership Themes Representative Quotations* Focusing on a common purpose “To a large extent that is implicit in our design, … that quality improvement … provides a unifying mission.”[A] “…the interesting thing about the construct of a microsystem, …which is owned by none of the professional disciplines but is simply a way of describing the reality that the customer or patient or beneficiary or client experiences, you end up getting permission to talk about the reality of interdependent work.”[B] Developing technical and relational knowledge and skills “My experience is that they say ‘it is too big and then you have to grasp the whole system and then it must go up the hierarchy’ and then you are …, kind of the system's prisoner. You have to … start thinking I can do something on my level and if I do something then it will probably create movements in other parts of the system because I am a part of the system.”[E] “Some of them have never met a patient or client before and [interviewing a patient] forces them [to do so] and some of them are really scared…but we all work for the patient so [at least] once you have to meet the patient and take their perspective…”[C] Linking theory and practice in practice “…how you learn by doing measurement in your own work setting…how do you improve your own and [support] colleagues…[to] increase learning among staff in [their] clinic.”[F] “…learners benefit from reflection in relating the material that they read and the experiences they have as they try to apply these things in practice, … what does this mean for my professional role and conduct, … and development in future …, and what does it mean for the system where I'm working …”[A] Leveraging collaboration for mutual benefit “One critical thing is that they have a coach in their own organization and they have a contract with their clinical boss that they are actually expected to do something … expectation from the workplace with a … supervisor from their own department that works well with the academic supervisor.”[E] “So those with extensive experience share that experience with those with less experience. Those with less experience can ask sometimes the naive questions and prompt learning on both their own part and the part of those more experienced and so forth.”[A] Concentrating on leadership and coaching “…some students, they do not want new things into their thinking, they want confirmation that their old thinking is alright, … We think you have a need for knowledge or information that you do not have yet - and that is a challenge to say that to a professional person who has been successfully operative for like 20 years … it can be a critique.” [D] “You cannot make a bridge to new insight if you don't ground one end of the bridge in the footings where the student lives. And they are not prepared to let you build something where they live if you are going to violate it….and so part of the challenge is to affirm that so that you get permission to construct the footings on their side.”[B] Applying a blended and interprofessional learning model “The asynchronous discussion forum] was fun to do because I could comment or enquire into a … comment, opening up the comment or challenging a piece of it or affirming a hint in the comment…”[B] “Only using [the online platform] will drain my own knowledge development because I develop my own knowledge when I am teaching… [in the classroom].” [E] “… if you do not know with some clarity about your own work and its relationship to the achievement of benefit…and if you do not know how others' work adds to, enhances or diminishes or threatens or destabilizes or stabilizes your own contributions, you are in no position actually to work well with one another.”[B] “We talk about the encounter with the patient but also in the team, and they have to be aware asymmetric relationships and how that affects those who are [on] a lower level in the asymmetry and that is often patients or clients but can also be those you work with.”[C] *[LETTER] signifies unique faculty participant; given the small number of participants and to protect confidentiality, we have not linked the participant to their role as presented in Table 1.Study participants (ie, program faculty) described the purpose of the education program this way to contribute to innovation and improvement in health and welfare, as anchored in patient and family centeredness with the ultimate beneficiaries being those receiving health and social care services. The program's focus on the student's practical workplace impact helped make interdependence and interprofessional collaboration discernible. In addition, the program and course work helped make visible the gap between intentions and realities in health and social care. Thus, the aims of improvement in health and welfare offered a “unifying mission,” while the tools of improvement helped students to address the gap.
Developing Technical and Relational Knowledge and SkillsAnother design principle of the enacted curriculum was supporting students to understand both tools of QI and theories behind those tools. Respondents described wanting to have learners internalize improvement knowledge through application, be willing to make (and learn from) mistakes, make obstacles to improvement visible, use measurement effectively over time, be stewards of resources in pursuit of improvement, and understand the assumptions underpinning models of change. Faculties were comfortable with creating some frustration in students. In one course, students interviewed a patient/client about their experience of illness and of seeking care, a task uncomfortable for some, particularly those without clinical experience.
Linking Theory and Practice in the WorkplaceA unique feature of the program was the emphasis on having students continue to work in practice and to link explicitly their learning with work settings. The intention was to ensure a strong connection between theory and the workplace. Examinations were thus centered on application of course content in the student's work setting. The master's thesis itself combined both a practical contribution to improvement in the student's work setting and an academic study of that effort, together forming the content of the concluding third year of study.
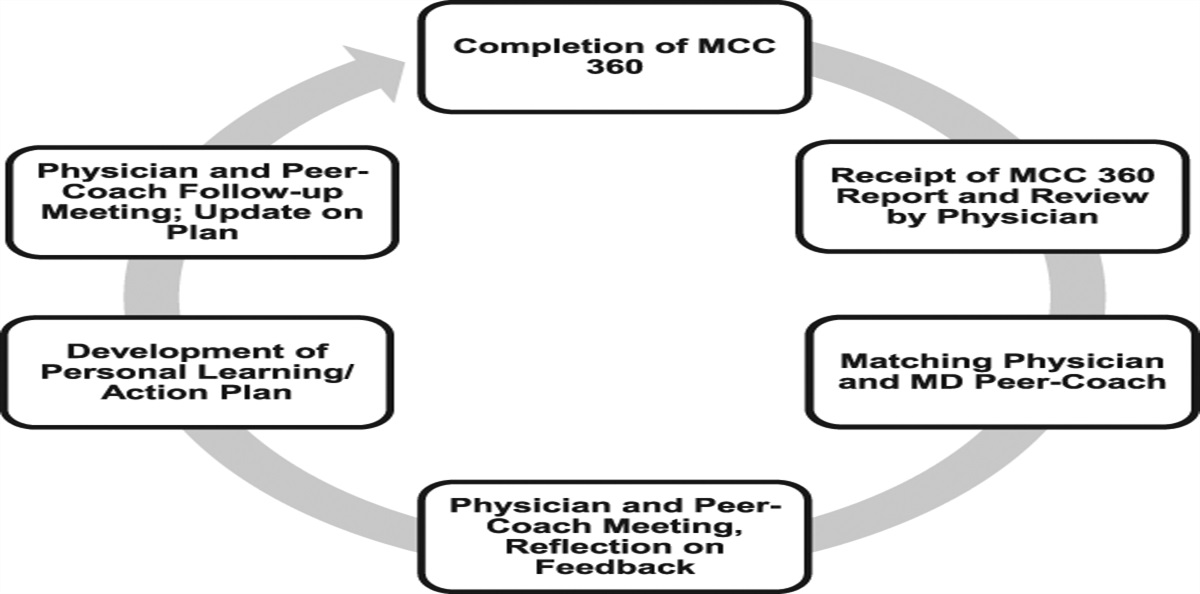
The program had an interpretive spiral design, described locally as a “cinnamon bun” model (Figure 1), to encourage students to iteratively return to, and therefore deepen their understanding of, concepts across and within courses. The faculty respondents reported that some of the students found drawing their learning forward and across topics very challenging. Students were also required to apply a reflective practice approach, connecting theory to application and share reflective journaling (as part of the remote interaction between campus sessions). Teachers too were encouraged to see the whole program and not only focus on their own subject matter. Reflective practice and program development were realized through a faculty learning group. They reviewed student evaluations, which led to continuous improvement of the program itself.
 FIGURE 1.:
FIGURE 1.: Jönköping Academy's “Cinnamon Bun” model—an interpretive spiral for curriculum design
Leveraging Collaboration for Mutual BenefitMuch of the collaboration that made the program successful lived in the relationship between the education and health and social service sectors. The program invited health and social service system leaders to formally endorse and support the time and effort required to take the program. In return, leaders and units benefitted from local improvement work and the development of their workforce.
A second kind of collaboration occurred in the cocreation of knowledge and understanding between teachers and learners. Many comments pointed out how much the faculty learned from their students. Honoring the experience and wisdom of learners (including current health and social care professionals) meant that the focus of the faculty was on adjusting with alternative teaching approaches to the range of learner needs, abilities, and constraints. As one respondent noted, “one of our big challenges is to meet [the] diversity of situations.” Study participants described how students were invited to share in the expert role usually reserved for the teacher.
A blurring of lines between teacher and learner created an “all teach—all learn” dynamic. Students taught each other about their areas of competence, coaching each other in improvement and leadership activities, and supporting each other in self-reflection. Teachers were learning from each other and from students. The faculties were not only there to provide coaching and support but also to provide both intellectual insights and practical expertise.
Concentrating on Leadership and CoachingAll faculties described their role as primarily facilitating and coaching a group of self-directed and highly motivated learners. One part of this coaching role was to invite the students to consider new ways of knowing, specifically regarding values and ethics. Participants recognized that this focus on values and ethics might be uncomfortable and risked alienating students and being counterproductive to learning. As a result, they described approaching students with respect, caring, and acknowledgement, actively validating the students' experiences and expertise.
Applying a Blended and Interprofessional Learning ModelThe blended learning model, online and in-person interaction and study, allowed the students to engage in the program while continuing to participate in the workforce. The study participants described that they initially believed that the online learning platform would facilitate structured discussion and access to content, while the campus sessions would support reflective and deep interaction. In practice, they found that the online platform allowed students to learn in new ways through asynchronous conversations where even the most introverted student could participate actively. Although the asynchronous interaction proved more useful than anticipated, one faculty member emphasized that the campus time for face-to face meeting was still invaluable. The campus meetings offered opportunities for students to deepen their thinking through face-to-face interaction and for faculty to develop more substantive relationships with students.
Although not an explicit topic of instruction, faculty addressed interprofessionalism through the program's design and course requirements. Participants identified that, on one hand, QI methods require effective communication and collaboration, almost always in interprofessional teams. On the other hand, good teamwork itself is supported by QI because it gives focus and structure to interprofessional collaboration. Reflection groups were designed deliberately to be interprofessional, faculties were drawn from multiple professional backgrounds, and assignments required students to “see” their own and their colleagues' competencies, knowledge systems, values, and biases. For example, students' reflective journals were reviewed by peers to deepen understanding and enhance learning. Program participants described how they used the concept that good QI requires interprofessional collaboration and that good collaboration can follow from QI.
DISCUSSIONProgram and course leaders at the Academy who participated in this study articulated the thinking behind the execution of their four a priori core design principles for teaching and learning of QI and leadership competencies. Through this exploration of the enacted curriculum, we expand the four principles, which have remained stable since the program began, into six themes which better help us explain the program's success as described in previously published literature reporting student and system outcomes.10,11
The importance of shared purpose related to organizational change is often cited in the literature.23,24 Although the program's aspirational purpose was more generally described as contributing to improvement in patient care and outcomes, the practical and near-term purpose was to help learners bridge professional silos and articulate the specific purpose of the local system within which they worked. An example of this more local purpose might be to “deliver exceptional care and improved outcomes to people living with diabetes in XYZ region.” This more granular method for defining purpose is the clinical microsystems approach of connecting service to a defined need in a population or subpopulation.25
There is a need to develop not only technical skills for improvement but also relational skills.26 The linking of QI and leadership competencies is strategic, reflected in an approach that equips the students to lead with both the technical and relational skills from wherever they are standing.
The emphasis of the master's at the Academy on linking theory and practice to support learning is itself not especially innovative.27–29 What is noteworthy, however, is that this focus on the student's own work setting is sustained throughout all three years of the program, where individual course assignments are synthesized into a thesis, all of which are connected to the learners' work context and tasks. This overall approach to program design is congruent with the interpretative spiral described by the “cinnamon bun” and reinforced by a reflective practice focus.
The multiple layers of collaboration enacted by the Academy's master's program, that is, shared planning, development, and execution from program design to course delivery, are quite instrumental in the Jönköping Academy's approach. One can see collaboration occurring at and between various levels: academic and delivery system, faculty, and students. The academic–practice partnership at the level of program design is crucial to ensuring success of students and their QI projects.30 The cocreation of knowledge in the classroom aligns with Knowles27 and his principles of the adult learner.
Faculty, selected for their expertise and experience, focused not only on cocreation of knowledge but also on making values and ethics explicit. There seemed to be an attitude of faculty engaging their entire selves (metaphorically, their heads, hands, and hearts) to engage these same aspects of the students.31
Given the nature of the student cohort (mostly practicing professionals within health and social care), it is not surprising that the teaching focus moved toward coaching and supporting leadership within the student group. In addition, curricular strategies such as peer review and asynchronous online discussion enabled peer coaching within the program. As the context in which health care professionals learn and practice is becoming increasingly volatile, uncertain, complex, and ambiguous, Maini et al32 argued that coaching and leadership skills are more and more relevant for undergraduate and continuing professional development. There is evidence that coaching provides a context suitable to developing what Cutrer et al33 refered to as the Master Adaptive Learner. The Master Adaptive Learner model is a medical education approach that would integrate very well into the Academy curriculum in that it parallels the QI steps of Plan–Do–Study–Act. It may benefit the Academy to consider a more structured and formalized approach to faculty stepping into the coaching role and how they can support the learners to more explicitly transfer peer coaching skills developed in the course of program activities to become coaches of improvement in their own workplaces.34
Blended learning generally refers to a learning environment that integrates online and face-to-face interaction.35,36 The Jönköping Academy's approach to blended learning in the master's program aligns with current evidence regarding the benefits and challenges of a blended learning environment.9,37 We show that the program was actually blended in more than one way. It was blended not only regarding delivery modes but also for academic and practice environments, theory and practice, and the interprofessional nature of both the teaching and the learning cohorts. In addition, our study shows that the online features of the blended curriculum lent itself to leveraging fundamental aspects of learning science regarding interleaving, or the mixing of subjects/concepts, and spacing, taking time and returning repeatedly to concepts.38
The design principles are mutually reinforcing. Although blended learning often provides logistical flexibility and allows busy professionals to participate in continuing education, it also enhances the ability to apply learning in one's own practice by virtue of remaining in practice while learning. The blended learning aspect of the program has a direct link to the interprofessional nature of the program, with evidence that online learning allows for a leveling of hierarchy between teachers and learners and also among learners.39 Similarly, the focus on common purpose is synergistic with the interprofessional design features of the program that support interprofessional collaboration around a QI challenge.
Methodological ConsiderationsOur research team included Academy insiders, with access and deeper understanding of the context, and outsiders, who provided perspective and balance. Because this study included only one organization, the results are limited in their generalizability. However, a single exemplary case, such as the faculty group at the Jönköping Academy, offers a unique opportunity to generate in-depth knowledge and contribute to theoretical generalization.40,41 Further research to explore how the design principles and themes are being enacted many years later with real-time triangulation between faculty and learner perspectives could be helpful.
CONCLUSIONThis study explored the thinking behind, and details of, the enactment of the program design principles for an interprofessional master's program in QI and leadership. The program designers initially established four core design principles. Our study of the enacted curriculum found six themes that can support effective learning: focusing on a common purpose, developing technical and relational knowledge and skills, linking theory and practice in the workplace, leveraging collaboration for mutual benefit, concentrating on leadership and coaching, and applying a blended and interprofessional learning model. Educators and program designers faced with an increased need to be flexible in teaching approaches and to offer opportunities for effective distance education can learn from this case example of effective teaching of QI and leadership in a blended format.Lessons for Practice ■ Master's level learning in quality improvement and leadership is enabled by a common purpose, technical and relational knowledge and skills, linking theory and practice while in the workplace, collaboration for mutual benefit, leadership and coaching, and a blended and interprofessional learning model. ■ A crucial step in learning from a program as delivered is to explore the enacted curriculum and not only the curriculum as planned. ■ The experience of a high-performing program in the delivery of blended learning can help others meet the challenges of master's level education for health and social care professionals in the 21st Century.
ACKNOWLEDGMENTSThe authors wish to thank the faculty participants at the Jönköping Academy for giving generously of their time and wisdom.
REFERENCES 1. Pokhrel S, Chhetri R. A literature review on impact of COVID-19 pandemic on teaching and learning. High Educ Future. 2021;8:133–141. 2. Daniel M, Gordon M, Patricio M, et al. An update on developments in medical education in response to the COVID-19 pandemic: a BEME scoping review: BEME Guide No. 64. Med Teach. 2021;43:253–271. 3. Garrison DR, Kanuka H. Blended learning: uncovering its transformative potential in higher education. Internet High Educ. 2004;7:95–105. 4. Castro R. Blended learning in higher education: trends and capabilities. Educ Info Tech. 2019;24:2523–2546. 5. Mosser G, Frisch KK, Skarda PK, Gertner E. Addressing the challenges in teaching quality improvement. Am J Med. 2009;122:487–491. 6. Cooke M, Ironside PM, Ogrinc GS. Mainstreaming quality and safety: a reformulation of quality and safety education for health professions students. BMJ Qual Saf. 2011;20:i79–i82. 7. Brown A, Lafreniere K, Freedman D, et al. A realist synthesis of quality improvement curricula in undergraduate and postgraduate medical education: what works, for whom, and in what contexts? BMJ Qual Saf. 2021;30:337–352. 8. Starr SR, Kautz JM, Sorita A, et al. Quality improvement education for health professionals: a systematic review. Am J Med Qual. 2016;31:209–216. 9. Bryan JL, Stewart DE, Uriarte J, et al. Eleven principles for teaching quality improvement virtually: engaging with geographically distributed learners. J Contin Educ Health Prof. 2018;38:276–281. 10. Nordin AMM, Areskoug-Josefsson K. Behavioural and operational outcomes of a Master's programme on improvement knowledge and leadership. Leadersh Health Serv (Bradf Engl). 2019;32:525–542. 11. Nordin A, Areskoug-Josefsson K. Effects of a Swedish master's programme on quality improvement and leadership - a qualitative study on micro, meso and macro levels of the welfare sector. Cogent Bus Manag. 2020;7:1725308. 12. Porter AC, Smithson JL. Defining, Developing, and Using Curriculum Indicators. CPRE Research Reports; 2001. Available at: https://repository.upenn.edu/cpre_researchreports/69?utm_source=repository.upenn.edu%2Fcpre_researchreports%2F69&utm_medium=PDF&utm_campaign=PDFCoverPages. Accessed January 15, 2022. 13. Brown MW. The Teacher–Tool Relationship: Theorizing the Design and Use of Curriculum Materials. In: Remillard J, Herbel-Eisenmann BA, Lloyd GM, eds. Mathematics Teachers at Work: Connecting Curriculum Materials and Classroom Instruction. New York, NY: Routledge; 2009:17–36. 14. Svensson L, Ellström P, Brulin G. Introduction—on interactive research. Int J Action Res. 2007;3:233. 15. Nyström ME, Karltun J, Keller C, Andersson Gäre B. Collaborative and partnership research for improvement of health and social services: researcher's experiences from 20 projects. Health Res Pol Syst. 2018;16:46. 16. Astleithner F, Hamedinger A. The analysis of sustainability indicators as socially constructed policy instruments: benefits and challenges of “interactive research”. Local Environ. 2003;8:627–640. 17. Institute for Healthcare Improvement. Eight Knowledge Domains for Health Professional Students. 1998. Available at: http://www.ihi.org/education/IHIOpenSchool/resources/Pages/Publications/EightKnowledgeDomainsForHealthProfessionStudents.aspx. Accessed December 3, 2021. 18. Homa K, Regan-Smith M, Foster T, et al. Coaching physicians in training to lead improvement in clinical microsystems: a qualitative study on the role of the clinical coach. Int J Clin Leadersh. 2008;16:37–48. 19. Nelson EC, Batalden PB, Godfrey MM. Quality by Design: A Clinical Microsystems Approach. 1st ed. San Francisco, CA: Jossey-Bass; 2007:459. 20. Lyle J. Stimulated recall: a report on its use in naturalistic research. Br Educ Res J. 2003;29:861–878. 21. Kane R, Sandretto S, Heath C. An investigation into excellent tertiary teaching: emphasizing reflective practice. High Educ. 2004;47:283–310. 22. Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. 2nd ed. Thousand Oaks, CA: Sage Publications; 1994:338. 23. Hollensbe E, Wookey C, Hickey L, et al. Organizations with purpose. Acad Manage J. 2014;57:1227–1234. 24. Quinn RE, Thakor A. The Economics of Higher Purpose: Eight Counterintuitive Steps for Creating a Purpose-Driven Organization. 1st ed. Oakland, CA: Berrett-Koehler Publishers; 2019:222. 25. Nelson EC, Godfrey MM, Batalden PB, et al. Clinical microsystems, part 1. The building blocks of health systems. Jt Comm J Qual Patient Saf. 2008;34:367–378. 26. Baker NJ, Suchman A, Rawlins D. Hidden in plain view: barriers to quality improvement. Physician Leadersh J. 2016;3:54–57. 27. Knowles MS. Andragogy in Action. 1st ed. San Francisco, CA: Jossey-Bass; 1984:444. 28. Kolb DA, Osland J, Rubin IM. Organizational Behavior: An Experiential Approach. 6th ed. Englewood Cliffs, NJ: Prentice Hall; 1995:646. 29. Gold B, England D, Riley W, et al. Development at an academic medical center: a partnership between practice plan, hospital, and medical school. J Contin Educ Health Prof. 2016;36. 30. Gonzalo JD, Dekhtyar M, Caverzagie KJ, et al. The triple helix of clinical, research, and education missions in academic health centers: a qualitative study of diverse stakeholder perspectives. Learn Health Syst. 2021;5:e10250. 31. Palmer PJ. The Courage to Teach: Exploring the Inner Landscape of a Teacher's Life. 20th anniversary ed. Hoboken, NJ: Jossey-Bass; 2017. 32. Maini A, Saravanan Y, Singh TA, Fyfe M. Coaching skills for medical education in a VUCA world. Med Teach. 2020;42:1308–1309. 33. Cutrer WB, Atkinson HG, Friedman E, et al. Exploring the characteristics and context that allow Master Adaptive Learners to thrive. Med Teach. 2018;40:791–796. 34. Wolff M, Deiorio NM, Miller Juve A, et al. Beyond advising and mentoring: competencies for coaching in medical education. Med Teach. 2021;43:1210–1213. 35. Singh H. Building effective blended learning programs. Educ Technol. 2003;43:51–54. 36. Thorne K. Blended Learning: How to Integrate Online & Traditional Learning. Sterling, VA: Kogan Page; 2003:148. 37. Boelens R, De Wever B, Voet M. Four key challenges to the design of blended learning: a systematic literature review. Educ Res Rev. 2017;22:1–18. 38. Gooding HC, Mann K, Armstrong E. Twelve tips for applying the science of learning to health professions education. Med Teach. 2017;39:26–31. 39. Keller C, Stevenson K. Participation in blended learning: settings and intersections of a master programme in healthcare. Int J Web Based Communities. 2012;8:504–520. 40. Tsang EWK. Generalizing from research findings: the merits of case studies. Int J Manag Rev. 2014;16:369–383. 41. Yin RK. Case Study Research: Design and Methods. 4th ed. Los Angeles, CA: Sage Publications; 2009:219.
留言 (0)