Medicinal plant resources of the studied ethnic groups
The present study provides the first quantitative analysis of 189 plant species utilized in traditional human ethnomedicine to address 100 ailments in peri-urban areas of south-central Ethiopia and is groundbreaking since it is the first quantitative ethnomedicinal research effort undertaken on extensively used plants in traditional medicine in the study districts. A higher number of medicinal plants have been recorded in Shashemene and Dilla peri-urban districts than in Hawassa per-urban areas. This could be due to the higher plant species diversity in the former districts due to the presence of natural forests, agroforestry practices, and plantations as well as higher plant knowledge acquisition by traditional healers in the studied areas. Moreover, the existence of interactions with agroforestry and natural resource institutions of learning, such as Wondo Genet College of Forestry and Natural Resources, Hawassa University, is attributed to the higher presence of plant resources. Several studies conducted in Ethiopia and abroad have reported varying quantities of therapeutic plants identified as a remedy for different human ailments. For instance, Chekole [7], Regassa et al. [49], Tefera and Kim [16], Tadeyos and Wendawek [50], and Mekuria and Abduro [51] compiled 51, 25, 70, 62, and 43 medicinal plant species, respectively, in their ethnobotanical investigations in different parts of Ethiopia. Ishtiaq et al. [52], Tugume et al. [53], Wiryono et al. [54], and Al-Robai et al. [55] documented 10, 27, 9, and 21 therapeutic plants, respectively, in Indonesia, Uganda, Pakistan, and Saudi Arabia.
Herbs were reported more frequently than other growth forms. Presumably, due to their widespread availability, the presence of market accessibility, and their greater therapeutic efficacy. Several studies reported similar results [56,57,58]. Fabaceae, Asteraceae, Poaceae, Lamiaceae, Solanaceae, Rutaceae, Cucurbitaceae, and Euphorbiaceae had the most dominantly utilized plant families among the three ethnic groups, suggesting that these plant families continue to provide a wide range of medical benefits to the local community. Several scientists have also developed hypotheses about specific plant families as part of their ethnobotanical study. For instance, Amjad et al. [59] demonstrated that the dominance of Asteraceae and Lamiaceae species in treating ailments is most likely due to the presence of secondary metabolites. In addition, [60,61,62] suggested that the dominance of these families in disease treatment might be due to their aromatic properties and abundance of essential oils. Furthermore, the findings of [41] indicate that these families were dominant in the flora of Ethiopia and Eritrea. Similar findings have also been observed elsewhere in the tropics [47, 49] and [54,55,56,57,58,59]. Furthermore, the discussions with informants also revealed that the local people have been using these medicinal plants for many generations and have acquired these skills through repeated, long-term practices.
Cross-cultural analysis of ethnobotanical knowledge
This finding strongly confirmed our hypothesis, which revealed a big difference in the knowledge of medicinal plants utilized among ethnic groups and ethnobotanical knowledge richness (Additional file 2: Table S2, Additional file 3: Table S3, Additional file 4: Table S4). The disparity was comparable in shared medicinal plant knowledge between the Oromo and Sidama ethnic groups (63.8%), and the Gedeo and Oromo ethnic groups (63.2%; Table 1). The difference in the use of reports may suggest social barriers [48]. For instance, the majority of Oromo healers were Muslims, and their language is different from that of the Sidama and Gedeo ethnic groups. This might hamper the sharing of ethnobotanical knowledge across ethnic groups, particularly the secrecy of healers [46, 60]. In comparison, the Oromo ethnic group solely reported a higher number of unique medicinal plant species than Sidama and Gedeo (Table 1). This might be due to the wider market access, intermarriage, mobile pastoralists, and proximity to natural and plantation forests, which make the knowledge broader than that of other ethnic groups. For instance [3, 46, 61, 62] conducted similar cross-cultural ethnobotanical knowledge comparisons in various countries and concluded that ethnicity and cultural practices have shaped traditional ethnobotanical knowledge among local inhabitants and might result in isolated knowledge of plant utilization [68,69,70].
For instance, Achyranthes aspera L. is a common medicinal plant species among the three studied ethnic groups. Although it has been reported to heal a variety of illnesses. It is claimed to heal respiratory organ illnesses between the Gedeo and Oromo ethnic groups (Additional file 2: Table S2), which is a differed use report from other pairs, and to cure spiritual complications between Gedeo and Sidama ethnic groups (Additional file 3: Table S3), and stomachache between Oromo and Sidama (Additional file 4: Table S4), respectively. Similarly, Aloe macrocarpa Tod. is a shared medicinal plant between the Gedeo and Oromo and Oromo and Sidama ethnic groups. However, it was described as a curative plant against gonorrhea between the Gedeo and Oromo ethnic groups, as well as malaria between the Oromo and Sidama ethnic groups (Additional file 2: Table S2, Additional file 4: Table S4). Again, Croton macrostachyus Hochst. ex Delile was a common medicinal plant across all the studied ethnic groups. However, in each pair, it was reported to cure three district ailments. These findings might indicate disparities in knowledge about the medicinal use of various plants among the ethnic groups studied (Additional file 2: Table S2, Additional file 3: Table S3, Additional file 4: Table S4).
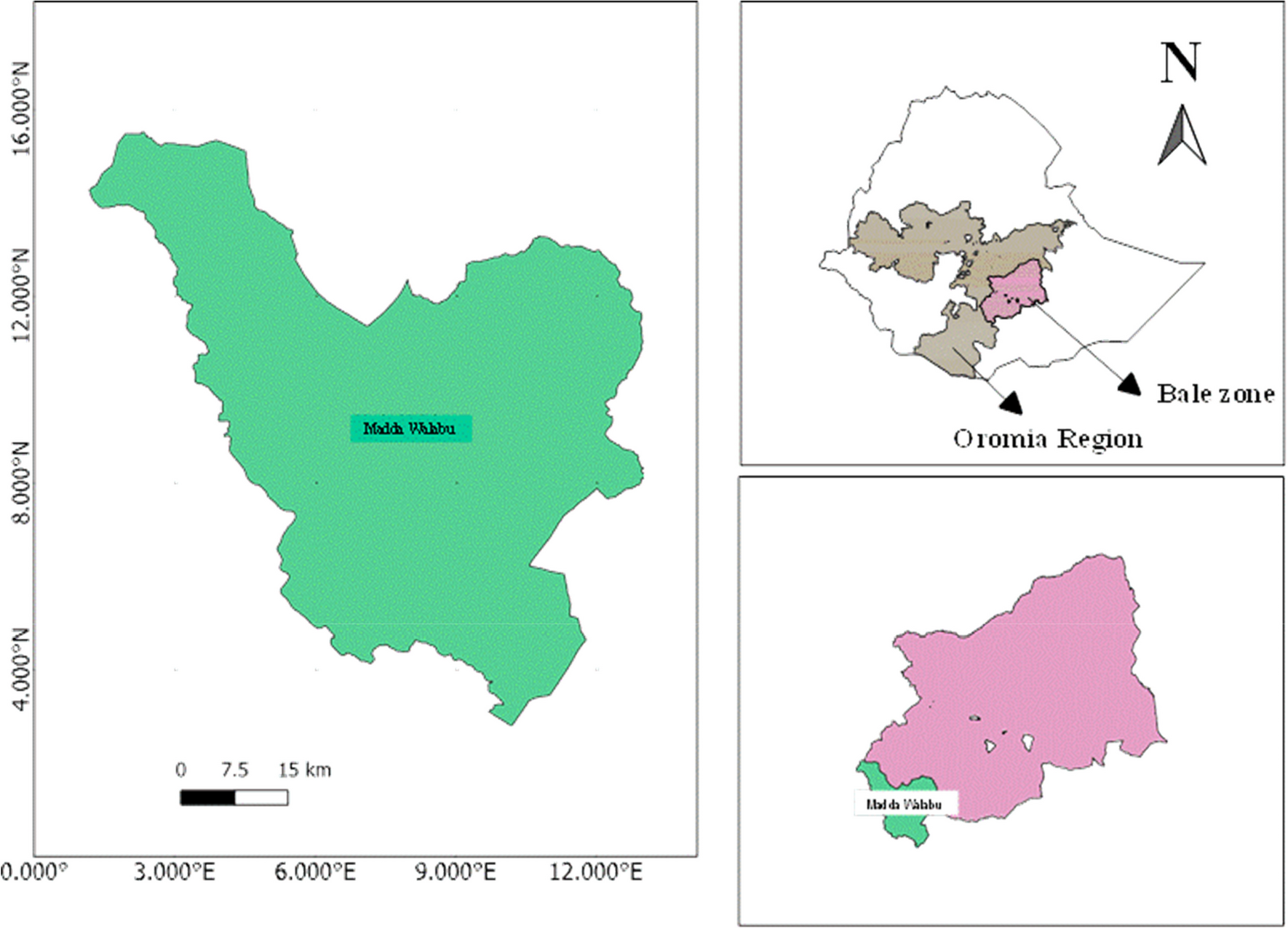
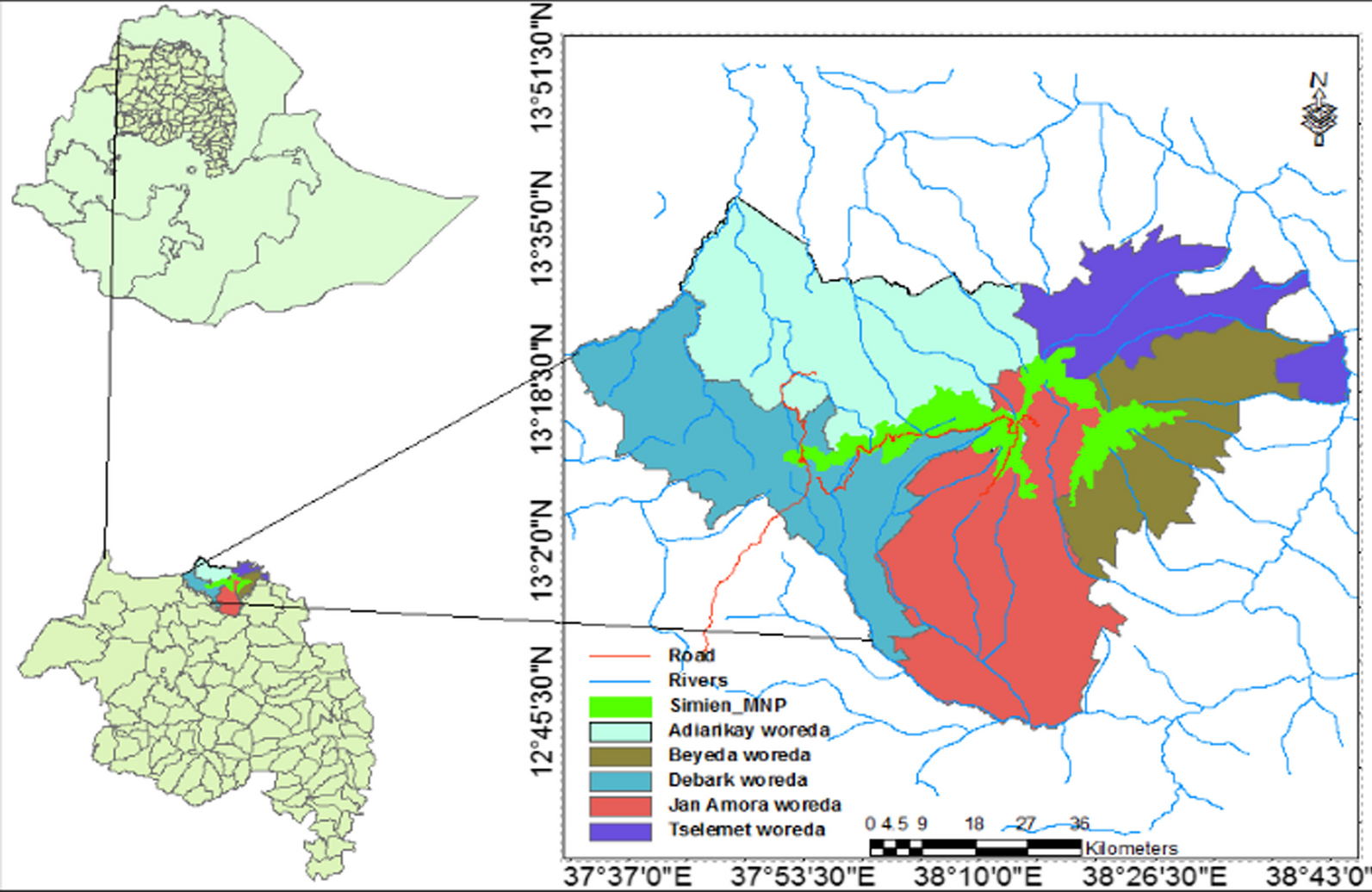
The other interesting finding in this study is that there were cultural similarities between ethnic groups (Table 1). As shown in Fig. 1, the study site of the Dilla peri-urban area is geographically far from the Shashemene and Hawassa study areas. However, this study revealed that the Gedeo and Sidama ethnic groups shared greater ethnobotanical knowledge, which was 39.8% higher than the other pairs (Table 1). This demonstrated that these ethnic groups used the same medicinal plants to treat the same ailments and were more culturally related than any other comparable pairs (Additional file 2: Table S2). For instance, both ethnic groups used Ajuga integrifolia Buch.-Ham. ex D.Don, Albizia gummifera (J.F.Gmel.) C.A.Sm., Allium sativum L., Artemisia abyssinica Sch.Bip. ex A.Rich., Calpurnia aurea (Aiton) Benth., Carica papaya L., Catha edulis (Vahl) Forssk. ex Endl., Cinnamomum verum J. Presl, and Croton macrostachyus Hochst. ex Delile against stomachache, dizziness, typhoid, spiritual complications, jaundice, and malaria. This similarity in plant use might be due to a common body of information about sickness, the wide distribution of species in the area, the historical stratifications of the studied ethnic groups, as well as similar sociocultural adaptations and interactions between people and their environments [3, 65, 66]. According to [72], similarities in how various ethnic groups use the same plants may be explained by the fact that some of them have had social connections with others. In addition, religious and linguistic cohesions may promote the transmission of knowledge on medicinal plant usage and illness treatment similarities between the two ethnic groups [73].
Comparing different indices of ethnomedicine in healing human ailments
Scholars believe that the high cultural importance value indicates that medicinal plants are widely used and highlights a high level of agreement in the survey culture about the species [74]. In this study, the overall analysis of the above-captioned indices revealed the presence of a high level of utilization of medicinal plants among the three ethnic groups studied. In the Sidama ethnic group, Zingiber officinale Roscoe scored the highest cultural importance value (0.73), followed by Croton macrostachyus Hochst. ex Delile (0.571) and Gymnanthemum amygdalinum (Delile) Sch.Bip. (0.397), which claimed to treat various ailments (Table 2). In this ethnic group, because of its use of diversity, Croton macrostachyus Hochst. ex Delile ranked at the top by the RFC (0.27), RI (1), and CV (0.039) indices. However, according to Tardío and Pardo-De-Santayana [4], Zingiber officinale Roscoe was considered a culturally more significant medicinal plant than Croton macrostachyus Hochst. ex Delile. With the same approach, Croton macrostachyus Hochst. ex Delile scored a high cultural significance value (0.762) and ranked first by all indices used, followed by Aloe macrocarpa Tod. (0.603) and Gymnanthemum amygdalinum (Delile) Sch.Bip. (0.54) in the Oromo ethnic group (Table 2). Interestingly, Croton macrostachyus Hochst. ex Delile again scored the highest cultural importance value (1.27) in the Gedeo ethnic group than Sidama and Oromo, followed by Albizia gummifera (J.F.Gmel.) C.A.Sm. (0.746) and Calpurnia aurea (Aiton) Benth. (0.492) (Table 2). Thus, the Gedeo ethnic group, followed by the Oromo, had stronger cultural practices to identify the medicinal potentials of the species (Croton macrostachyus Hochst. ex Delile) than the Sidama ethnic group.
It was also true that plants with higher use reports (UR) always had higher utilization levels [75]. Our findings are similar to previous findings by [55] and [76]. They conducted an ethnobotanical survey in different parts of Bangladesh and Saudi Arabia and found that plants with high use reports have high use values. In this study, Albizia gummifera (J.F.Gmel.) C.A.Sm. is a shared plant species among ethnic groups, and ranked 12th in the Sidama ethnic group with 13 use reports. Whereas it ranked 18th in the Oromia ethnic group with 10 use reports, and interestingly, it ranked second in having culturally relevant plants to cure various illnesses in the Gedeo ethnic group with 47 use reports (Additional file 5: Table S5). Moreover, Gymnanthemum amygdalinum (Delile) Sch. Bip., is again a species shared by all studied ethnic groups, ranked 3rd in the Sidama and Oromo ethnic groups with 25 and 34 use reports as culturally significant medicinal plant species, respectively, whereas 8th in the Gedeo ethnic group with 17 use reports (Table 2). This shows that, when compared among the ethnic groups, Gymnanthemum amygdalinum (Delile) Sch. Bip. is found to be a more culturally significant medicinal plant for the Oromo and Sidama ethnic groups.
In addition, medicinal plant species with high RFC and RI values should be recommended for pharmacological and phytochemical studies, as they are widely used and expected to have therapeutic properties [45, 57, 72, 73]. This emphasizes the importance of understanding the potential therapeutic properties of plants for various ethnic groups. In our study, RFC ranged in ascending order from Cinnamomum verum J.Presl, Moringa stenopetala (Baker f.) Cufod., and Ricinus communis L., (0.048 each) to Croton macrostachyus Hochst. ex Delile (0.27) in the Sidama ethnic group. Whereas, Psidium guajava L. (0.048) to Croton macrostachyus Hochst. ex Delile (0.333), and Lagenaria siceraria (Molina) Standl., Melia azedarach L., Nigella sativa L., Ocimum lamiifolium Hochst. ex Benth, Phytolacca dodecandra L'Hér., and Zingiber officinale Roscoe (0.048 each) to Croton macrostachyus Hochst. ex Delile (0.444), in the Oromo and Gedeo ethnic group, respectively (Additional file 5: Table S5). Moreover, Aloe macrocarpa Tod., Albizia gummifera (J.F.Gmel.) C.A.Sm., Calpurnia aurea (Aiton) Benth., Croton macrostachyus Hochst. ex Delile, Cucumis prophetarum L., Ekebergia capensis Sparrm., Gymnanthemum amygdalinum (Delile) Sch. Bip., Afrocarpus falcatus (Thunb.) C.N.Page, and Ruta chalepensis L. had scored the highest RFC and RI values across the studied ethnic groups, thus indicating their strong local medicinal role (Table 2) and highlighting their potential for pharmacological study in the future [78]. Furthermore, [70, 72] suggested that plants with lower RFC and RI scores may be less essential, but their low values may indicate that local people are unfamiliar with their wider utilization, potentially leading to knowledge extinction (Additional file 5: Table S5).
Public health and the marketability of medicinal plants in the study areas and beyond
The development of new medications and therapies for public health is greatly influenced by ethnobotanical knowledge studies [80, 81]. Because several ethnobotanical investigations could lead to the identification of new medicinal plant sources or the elaboration of the mechanisms behind traditional remedies [79]. For instance, such studies have resulted in the development of important drugs such as reserpine from Rauvolfia serpentina (L.) Benth. ex Kur plant species to treat hypertension, podophyllotoxin from Podophyllum peltatum L. to treat cancer, and bromelain from Ananas comosus (L.) Merr. to treat cancer [79]. According to several studies conducted elsewhere, medicinal plants and spices have recently been produced as natural, efficient antibacterial agents against a wide range of harmful microbes [81]. Allium sativum L., Croton macrostachyus Hochst. ex Delile, and Zingiber officinale Roscoe have been identified as potential plant sources for managing antibacterial, antifungal, and antiviral properties. They are potentially cost-effective in disease management and the problem of drug resistance [79,80,81,82,83].
The present study revealed that plants with high RI and RFC values have promising potential against different pathogens and play a great role in maintaining general public health in the studied areas and beyond. Afrocarpus falcatus (Thunb.) C.N.Page, Aloe macrocarpa Tod., Albizia gummifera (J.F.Gmel.) C.A.Sm., Calpurnia aurea (Aiton) Benth., Croton macrostachyus Hochst. ex Delile, Cucumis prophetarum L., Ekebergia capensis Sparrm., Gymnanthemum amygdalinum (Delile) Sch. Bip., and Ruta chalepensis L. are the most cited medicinal plant species against communicable and non-communicable diseases in the communities we studied (Additional file 1: Table S1). Besides in vitro, investigations of some of the aforementioned medicinal plant species were reported and found to be most effective against various disease-causing pathogens in various parts of Ethiopia [83, 85], and further research is recommended on their pharmacological contents.
During our key informants’ survey and market observation, we realized that income to traditional healers from patient treatment and the sale of medicinal plants was insignificant. Lack of awareness, cheap pricing, and less market access of the traditional medicine are likely influence the income. 80% of the collected medicinal plant resources did not have market access and were limited in dissemination. This would imply that most medicinal plants are only collected from the wild for remedy preparations only when needed. The same findings were reported in elsewhere in Ethiopia [86, 87]. While 20% of the medicinal plants were marketable, for example, Aframomum corrorima (A.Braun) P.C.M.Jansen, Allium cepa L., Allium sativum L., Aloe macrocarpa Tod., Aloe vera (L.) Burm.f., Artemisia absinthium L., Artemisia abyssinica Sch.Bip. ex Oliv. & Hiern, Calpurnia aurea (Aiton) Benth., Capsicum frutescens L., Carica papaya L., Coriandrum sativum L., Catha edulis (Vahl) Forssk. ex Endl., Cinnamomum verum J.Presl, Citrus × aurantiifolia (Christm.) Swingle, Citrus limon (L.) Osbeck, Coffea arabica L., Cucurbita pepo L., Cymbopogon citratus (DC.) Stapf, Echinops kebericho, Eucalyptus globulus Labill., Hagenia abyssinica, Indigofera arrecta Hochst. ex A.Rich., Kalanchoe densiflora Rolfe, Kalanchoe petitiana A.Rich., Lactuca inermis Forssk., Linum usitatissimum L., Lepidium sativum L., Mentha spicata L., Moringa stenopetala (Baker f.) Cufod., Nicotiana tabacum L., Nigella sativa L., Olea europaea subsp. cuspidata (Wall. & G.Don) Cif., Ruta chalepensis L., Rhamnus prinoides L'Hér., Taverniera abyssinica A.Rich., Triticum turgidum subsp. dicoccum (Schrank ex Schübl.) Thell., Vicia lens (L.) Coss. & Germ., Withania somnifera, and Zingiber officinale Roscoe. Although an in-depth valuation of traditional medicinal plant marketability in the respective research sites was outside the scope of this study, some healers appealed the importance of traditional medicinal plant marketability in the study areas. In overall, the present study could also be used as baseline for a future detailed investigation of the market potential and value chain of medicinal plant resources in the study regions and beyond.






留言 (0)