
Remember me






This trial was approved by the institutional review board of the First Hospital of the University of Science and Technology of China and registered at the Chinese Clinical Trial Registry with registration number ChiCTR2100055093(31/12/2021).
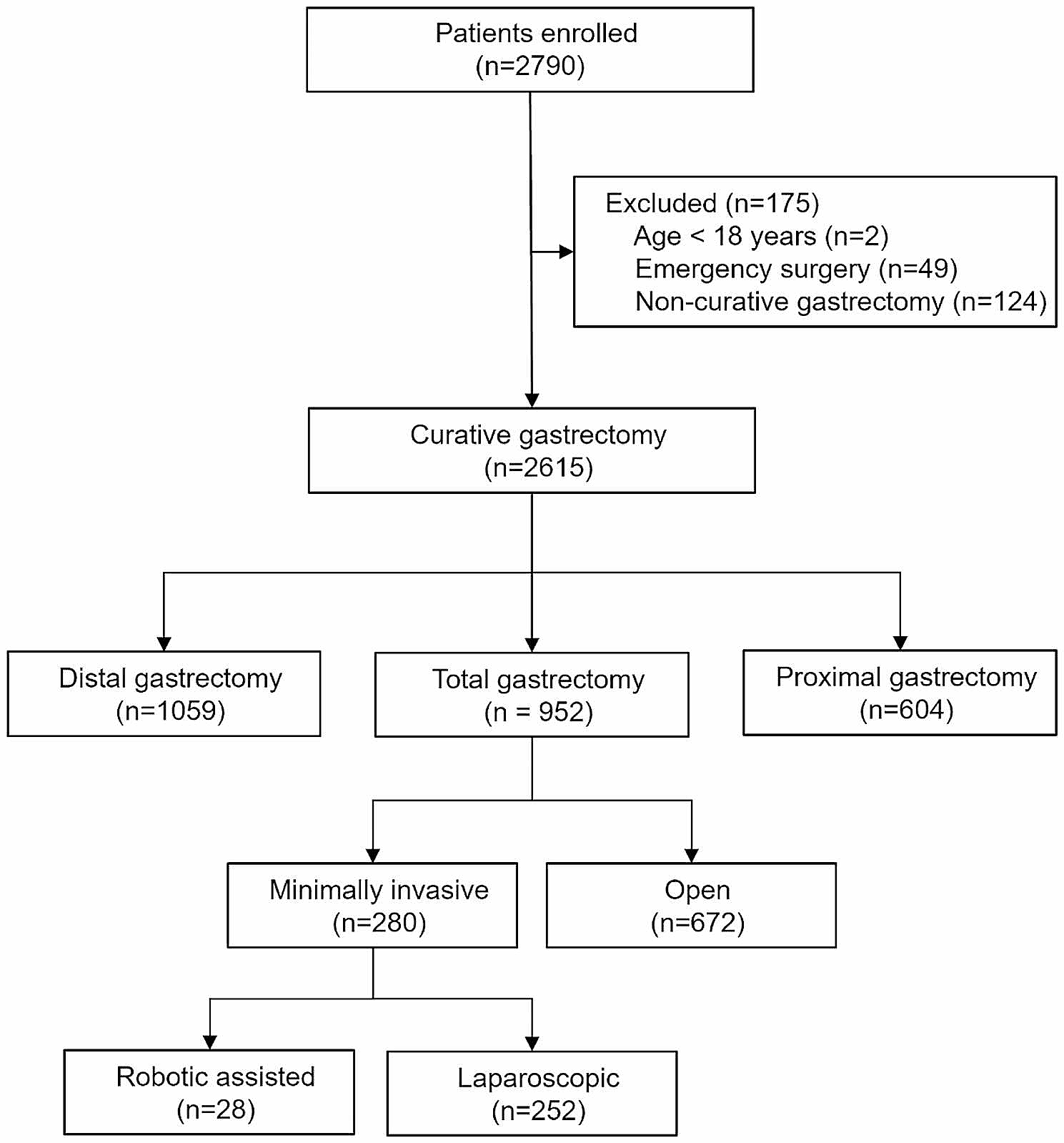
Out of 111 elderly patients who underwent cardiac surgery and received DEX infusion, 11 were excluded, 12 withdrew, and 88 were included in the study (Fig. 1). The patients were divided into two groups: Group L (n = 44), in which patients received a low-rate infusion of DEX at 0.1–0.5 µg/kg/h and Group H (n = 44), in which patients received a high-rate infusion of DEX at 0.5–0.9 µg/kg/h. The inclusion criteria were as follows: (1) having undergone cardiac surgery (valve or aortic root surgery) between January 2022 and November 2022; (2) age between 60 and 75 years; and (3) DEX infusion rate of 0.1–0.5 µg/kg/h or 0.5–0.9 µg/kg/h, continued until 1 h before postoperative extubation in the cardiac surgery intensive care unit (CSICU). The exclusion criteria were as follows: (1) preoperative disagreement or refusal to participate in the study; (2) pre-existing history of mental illness; (3) baseline MMSE (MMSE0) score ≤ 20; and (4) ejection fraction ≤ 50% after admission. The withdrawal criteria were as follows: (1) perioperative use of DEX that was not within the scope of the defined group parameters or the use of a loading dose; (2) a second admittance to CSICU; (3) incomplete postoperative follow-up data; (4) failure in patient data analysis; (5) Dex infusion for more than 36 h; and (6) III° atrioventricular block during Dex infusion.
Fig. 1
The technical flowchart of the clinical research on patients. MMSE, Mini-Mental State Evaluation; EF, ejection fraction; CSICU, cardiosurgery intensive care unit; DEX, dexmedetomidine
All patients underwent cardiac surgery following standard anesthesia and CPB protocols and were routinely admitted to the CSICU for postoperative management. The types of surgery were categorized into valve surgery and aortic root surgery. Valve surgery included procedures such as isolated mitral, tricuspid, and aortic valve surgery; combined mitral and tricuspid valve surgery; and combined mitral and aortic valve surgery. Aortic root surgery included procedures such as Bentall surgery, Wheat surgery, and David surgery.
We collected and analyzed data related to age; sex; body mass index (BMI); MMSE0 (recorded on preoperative Day 1 [T0]); educational level (specifically, those with < 5 years of education); history of hypertension and diabetes; type and duration of surgery; preoperative ejection fraction (EF); hemoglobin level; benzodiazepine use; doses of sufentanil, propofol, and penehyclidine; and duration of DEX infusion (Table 1).
Table 1 Baseline clinical characteristics and intraoperative variables of Group L and Group HData collectionWe recorded and collected relevant preoperative and intraoperative baseline data, as described above. The data also included various outcome indicators, such as MMSE score on postoperative Day 2 (MMSE1), Day 7 (MMSE2), Day 14 (MMSE3), and Day 28 (MMSE4); instances of intraoperative hypotension; duration of initial intubation; length of CSICU stay; incidence of postoperative delirium (POD); occurrence of myocardial infarction and stroke; length of hospital stay; and hospitalization-related mortality.
Primary outcome measuresOur primary outcome was short-term cognitive function. We used the MMSE score recorded on postoperative Day 2 as the primary observation endpoint. Assessments were conducted in the CSICU or the cardiac surgery ward on this day. During inpatient evaluation, patients were assessed face-to-face by the researchers, whereas for out-of-hospital evaluations, the MMSE scale evaluations were conducted through WeChat video visits, combined with a patient self-help model. Uniform assessment forms were used for both in-hospital and out-of-hospital evaluations.
Secondary outcome measuresThe secondary outcomes for this study included the incidence of POD, intraoperative hypotension and bradycardia, length of hospital stay, and in-hospital mortality. The CSICU of our unit has a routine protocol for POD evaluation. To differentiate from the residual effects of anesthesia, delirium screening was started 24 h after cardiac surgery and performed twice a day. The Confusion Assessment Method Intensive Care Unit (CAM-ICU) scale was used to assess delirium every 12 h, specifically at 9:30 and 21:30. When a patient was discharged from the CSICU to the ward, the CAM was used to assess delirium every 12 h until postoperative Day 5. If delirium was not resolved by this day, the evaluation continued until discharge. The incidence of POD was defined as the percentage of patients who developed delirium during their hospitalization. Intraoperative hypotension was defined as systolic blood pressure below 80 mmHg lasting for at least 1 min or instances where the systolic blood pressure dipped below 80 mmHg at least twice. Intraoperative bradycardia was defined as a heart rate ≤ 60 beats/min. Myocardial infarction was defined as an increase in troponin I by more than 10 ng/mL during the postoperative CSICU and ward stays, along with higher than normal CK-MB, total CK exceeding 10%, and a new Q wave in the ECG lead in two or more consecutive measurements. Postoperative stroke was identified when its diagnosis was confirmed by a neurologist during postoperative CSICU and ward monitoring. CSICU duration was defined as the time of the patient’s stay in the CSICU, calculated in hours. Hospital stay was defined as the time from registration of patient admission to their discharge. In-hospital mortality was calculated as the ratio of deaths from CSICU admission to discharge relative to the total number of patients in the study group.
Statistical analysisSample size calculationThis study aimed to compare the differences in the MMSE scores on postoperative Day 2 between the two study groups. Studies by Shaefi et al. [14] and Saczynski et al. [15] showed that the MMSE score on postoperative Day 2 is the lowest point, with the minimum clinically significant difference being 2 points after surgery. The pre-test results of 12 patients using low-dose infusion showed a mean and standard deviation of 24.4 ± 2.6 for the postoperative Day 2 MMSE scores. Assuming a difference test of the usage rate with a 5% two-tailed type I error rate (α = 0.05) and a test efficiency of 90%, the sample size was calculated using PASS 15.0 software, requiring 37 patients in each group. Considering a dropout rate of approximately 20%, a sample size of 46 patients per group was planned.
Statistical methodsNormally distributed continuous variables were described using mean ± standard deviation, non-normally distributed continuous variables were described as median (interquartile range), and categorical variables were described using percentages. The Mann–Whitney U test was used to compare the primary outcome indicators between the two groups; secondary outcome indicators, specifically the hours of initial intubation, CSICU stay, and duration of hospitalization; and baseline indicators such as age, BMI, MMSE0, CPB time, duration of surgery, anesthesia time, and infusion dose of sufentanil, propofol, and DEX infusion time. The Wilcoxon signed-rank test was used for within-group comparisons. Preoperative EF and hemoglobin were tested using an independent-sample t-test, and the remaining indicators were tested by Pearson chi-square test or Fisher’s exact test. Statistical analyses were performed using SPSS 22.0 (IBM, Armonk, NY, USA) or R software, and a two-tailed p-value < 0.05 was considered statistically significant.
Comments (0)