
Remember me


Medication preparation and administration are among the core activities that nurses perform daily, and they are far from linear processes.1, 2 Nurses must use multiple sources of information and clinical reasoning to prepare and administer medications—and do so in an environment that requires them to juggle competing demands and orchestrate diverse patient care activities.2-4 The cognitive workload is considerable, and can affect nurses' decision-making and their ability to deliver medications safely every time.3 Structural factors such as a facility's medication system, behavioral differences in nurses' approach to medication preparation and administration, and differences in nurse–patient interactions can also impact these tasks and lead to medication errors.5
In a systematic review of 66 studies, Berdot and colleagues focused on drug administration errors identified through observation and found that the median rate of the total opportunity for errors (the sum of total doses ordered and unordered doses given) was 10%.6 Another study conducted in two large hospitals in Iran found that administration errors occurred on average in one of every three medication doses.7 To reduce medication error rates and opportunities for error, numerous strategies have been implemented. These strategies include double-checking medications, improving relevant nursing education and training, using bar code–assisted medication administration systems, and creating medication “safe zones” to reduce interruptions and distractions.8-10 But these interventions are often implemented without input from the direct care nurses who actually prepare and administer medications.
In searching the literature, we found few qualitative studies that focused on nurses' experiences and perspectives regarding medication safety practices, and those that did were done outside the United States.2, 11, 12 In the Netherlands, a study conducted at a large academic hospital explored nurses' experiences with and perspectives on medication safety policies and practices.12 The researchers concluded that “implementation of safety practices alone is not enough” to ensure safe medication management by nurses. In Iran, researchers at a teaching hospital asked nurses to identify facilitators and barriers related to medication errors, as well as preventive measures.11 With regard to prevention, two main themes emerged: the importance of “acting professionally” (such as following policies and procedures for safe medication administration and engaging in continuous education) and the use of “technical strategies” (such as using red labels and double-checking to distinguish high-risk drugs and having skilled nurses administer drugs). In Australia, researchers sought to identify the medication administration safety strategies of nurses at a regional hospital.2 Nurses were observed and interviewed to determine what approaches they implemented. While the researchers found that nurses used numerous information sources and “sophisticated clinical reasoning” to administer medications safely, they also noted that interruptions, time pressure, and other factors were common obstacles. These studies provide valuable, real-world nursing perspectives on medication preparation, administration, and error prevention.
In alignment with the literature supporting specific interventions, our organization has implemented the use of automated medication dispensing cabinets, bar code–assisted medication administration, double checks of select medications, and education on medication safety practices. Yet medication errors remain prevalent, with over one-third of such errors occurring during administration alone. Obtaining the insights of direct care nurses could help to identify areas for improvements to policies and practices, including current nursing medication safety practices.
Study purpose. The aim of this study was to explore direct care nurses' experiences with and perspectives on medication safety practices and errors.
METHODSDesign. This study used a descriptive qualitative design, with semistructured interviews that were conducted in focus groups as well as one-on-one. The hospital health care system's institutional review board approved the study before data collection began.
Sample and setting. Participants were recruited from a convenience sample of over 2,500 nurses working within a 10-hospital health care system, which includes an academic level 1 trauma center, a pediatric facility with level 1 trauma services, a neonatal and women's hospital, and seven community hospitals in the southeastern United States. Recruitment methods included inviting nurse participants from an earlier online survey to volunteer, recruiting volunteers through email blasts describing the study and through various hospital-level meetings at which investigators described the study, and snowball sampling (in which additional nurses joined the study after hearing about it from a peer).
To be eligible for inclusion, one had to be an RN or LPN who administers medications on inpatient acute care units and in the ED at one of the hospital study sites. Nurses working in ambulatory, procedural, or outpatient settings; those working in allied or support areas; and nurses in leadership, administrative, education, or executive roles were excluded. Nonnurse team members were also not eligible.
Data collection. Interviews focused on daily medication administration practices, medication errors, and near misses. The open-ended questions used in the interviews were developed by the research team based on the literature and were reviewed for relevance and appropriateness by two content experts on the team: an experienced qualitative nurse researcher (VL) and a nurse scientist (DP). The final interview guide enabled investigators to ensure consistency across groups. Questions included, “What's a typical day like on your unit when you prepare and give medications?” “What gets in the way of safely administering medications?” and “When a medication error is made on the unit, how is it handled?” (For more, see Representative Examples of Interview Questions.)
 Box 1:
Box 1: Representative Examples of Interview Questions
Investigators provided participants with a printed information sheet explaining the study prior to the interviews. All interviews were conducted by the two primary investigators (LA, AAS) between March and November 2019. The two investigators worked together in alternate roles, with one person leading and facilitating the interview and the other taking field notes. All of the interviews took place in hospital areas that ensured privacy (such as offices or meeting rooms) in order to promote an environment that supported confidentiality and open dialogue. Depending on the number of participants and level of participant engagement, the interviews lasted between 45 and 60 minutes. Time was allotted at the start for questions and answers about the study, and agreement to participate was indicated by remaining for the focused interview. Participants could withdraw from the study at any time. Every interview was audio recorded. A professional transcription services agency was employed to transcribe the interviews verbatim, so as to ensure the accuracy of captured elements.
Data analysis. Directed content analysis was used to examine transcribed and deidentified data from the interviews.13 The team's three researchers (LA, AAS, VL) individually reviewed the first two transcripts and coded the data. Codes were discussed until consensus was reached, and a codebook was developed for subsequent coding by the two primary investigators. All three researchers continued to meet monthly to keep discussing the codes and emerging themes, and to make sure that bracketing was maintained. (Bracketing is a crucial step used to ensure that codes and themes reflect participants' views and not researchers' preconceptions.) Descriptive statistics were used to describe demographics.
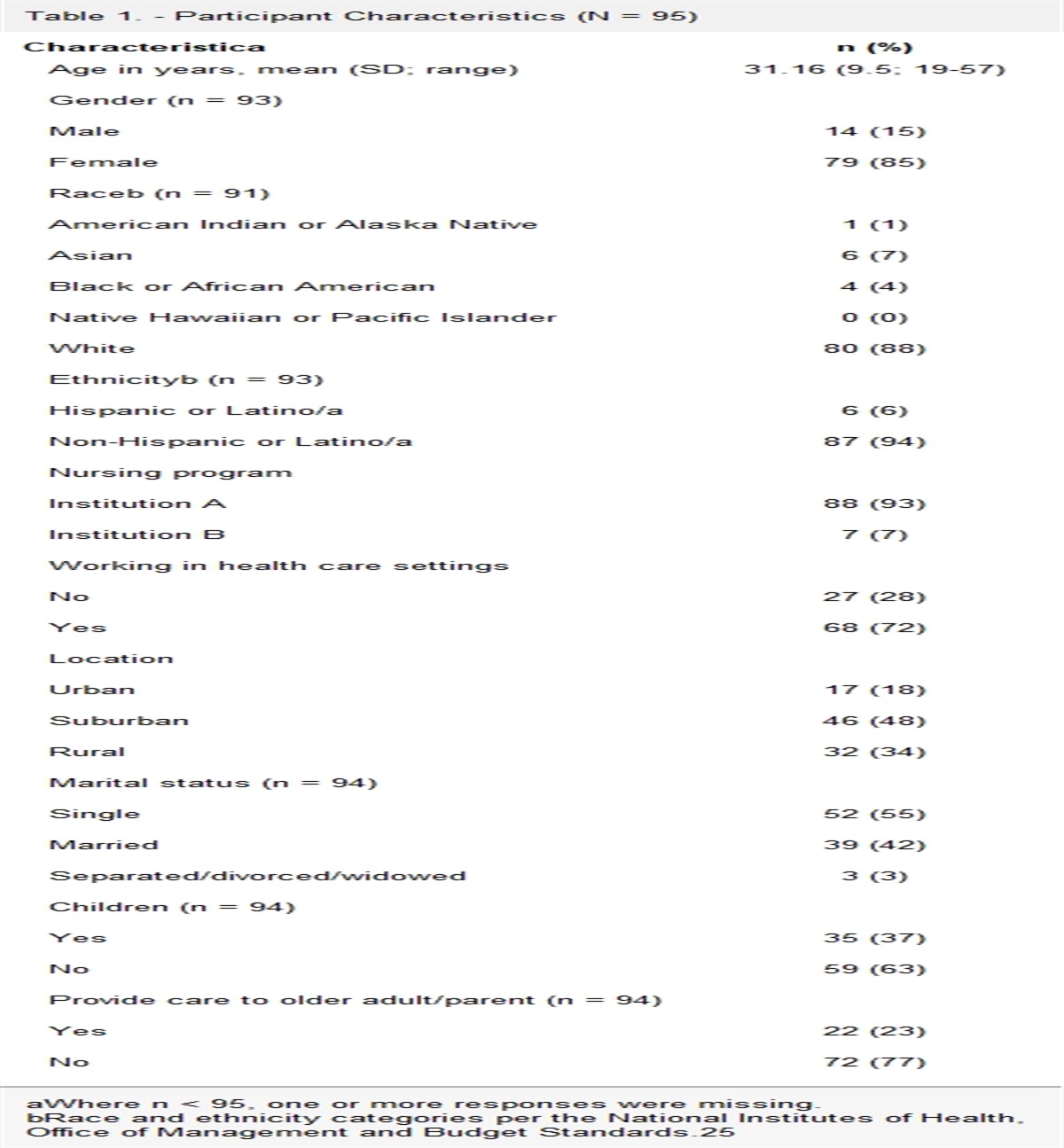
RESULTSSample. A total of 21 nurses participated, with 19 doing so via nine focus groups, each comprising two to five participants, and two doing so via one-on-one interviews. A majority of participants identified as female and non-Hispanic White. The mean age was 39 years (range, 24 to 60 years). The majority held a bachelor of science degree or a BSN. The mean length of nursing practice was nine years (range, one to 34 years); the main practice areas were the ED; medical–surgical unit; and intermediate care, progressive care, or step-down units. For more details on participant demographics, see Table 1.
Table 1. - Demographics (N = 21)a Characteristic n Gender Male 5 Female 16 Age, years Mean age (range) 39 (24-60) Highest education level Diploma 0 LPN 0 ADN/ASN 4 BS/BSN 16 MS/MSN or higher 1 Years practicing as a nurse Mean years (range) 9 (1-34) Practice areas Medical–surgical or oncology 6 Intermediate or progressive care or step-down unit 6 ICU 2 ED 7 Primary shift worked Day shift 14 Night shift 7 Hours worked per week Mean hours (range) 35 (12-48) Race and ethnicity American Indian or Alaska Native 0 Asian or Asian American 2 Black or African American 0 Hispanic or Latino 1 Native Hawaiian or other Pacific Islander 0 Non-Hispanic White 12 Another race 0ADN = associate degree in nursing; ASN = associate of science in nursing; BS = bachelor of science; MS = master of science.
aFor some questions there were missing responses. All values reflect only the available data.
Interview findings. In general, the interviews were lively, with participants freely sharing their experiences during interactive discussions. They described both positive and negative interactions with nurse colleagues, other health care professionals, and unit-based and hospital-wide systems that affected their ability to deliver medications safely. Many of the real-world, day-to-day challenges named during discussions resonated across groups. Some participants reflected on past errors and discussed how errors have shaped their personal medication safety practices. Others discussed errors and mistakes made by nurse colleagues but did not acknowledge that they themselves might have done so; as one nurse commented, “[It's] their problem, not my problem.”
Participants were asked about medication safety practices used at their place of employment, including hospital system–wide measures, their own clinical knowledge, and their own role as patient advocates. They described multiple system-wide measures, such as bar code–assisted medication administration, smart infusion pumps with drug libraries, and independent double-check verification processes for high-risk medications. They acknowledged the importance of the nurse's role and their own clinical knowledge. Many described using their clinical assessment skills (for example, checking vital signs, assessing consciousness and pain levels, and swallowing ability) to evaluate patient status as a “last checkpoint” before drug administration. Participants also discussed acting as patient advocates by communicating with physicians or pharmacists if an ordered medication seems incongruent with the patient's status or if an order is missing for a necessary medication, and by talking with patients about their medications (indications, potential side effects, dosing) and periodically reassessing to determine efficacy.
Four major themes concerning nurses' medication safety practices emerged from the interviews: the care environment, nurse competency, system influences, and the error paradigm (see Figure 1). These themes were often interrelated.
 Figure 1.:
Figure 1.: Predominant Themes and Codes from Qualitative Interviews
The care environment. This theme refers to factors in the work environment that affect the nurse's ability to focus well enough to prepare and deliver medications safely. Participants identified several such factors that adversely affected their ability to do so. The most common barriers were described as general unit chaos, heavy workloads, work-arounds that bypassed systemic safety measures, the time-consuming nature of nursing duties, and distractions and interruptions. These factors often intertwined and compounded the stress they felt.
Participants described various situations that were chaotic, involved heavy workloads, and caused them to multitask in an effort to manage time. Participants from all practice areas gave examples of distractions and interruptions that had disrupted their focus and resulted in their having to redo their work in preparing and administering medications. This in turn could cause them to bypass systemic safety mechanisms, as they tried to finish up quickly before they were distracted or interrupted again. The general chaos on the units required nurses to pivot and reprioritize their tasks frequently throughout the workday. They shifted between non–direct patient care tasks (such as answering phones and updating electronic health records [EHRs]) and direct patient care tasks (such as answering questions for patients and families and administering medications). One participant shared this chaotic experience:
“The monitor tech is calling you. The patient has [electrocardiogram] leads off. It's like, “I'm trying to pull meds. Hold on.” Then the charge nurse calls you and says, “Hey, I'm gonna give you another patient from the ED.” It's like, wait. The ED's calling to [give] report.”
Several participants spoke of heavy workloads and time constraints. They felt there often wasn't enough time in the day for them to care for patients the way they wanted and to accomplish all the tasks required. This caused some nurses to use work-arounds. As one participant stated, “People start to take shortcuts in an effort to keep the time management going.” Moreover, medication preparation and administration tasks can vary in ways that affect time management. Several participants described the task of crushing medications for patients as time-consuming and stressful. As one stated,
“Crushing meds is definitely a time-consuming process, especially when you have several meds that you need to crush to administer; and some patients take their pills very slowly.”
Another participant described the stress that occurs when almost every patient is on the same medication schedule: “You'll have several patients with a 30-minute window where you can give medications, and it's three or four of your [total number of] patients.” This made it difficult to administer all medications on time.
Many participants discussed the myriad continuous distractions and interruptions that happened throughout their workday. Distractions were described as events in the care environment (such as medication rooms, nurses' stations, hallways) that took their attention away from preparing or administering medications. One participant described the medication room this way:
“It's just so noisy. Sometimes I couldn't even hear myself think because the nurses come in and talk, and drawers are closing, someone is stocking items on a shelf.”
Interruptions were described as unexpected or undesirable pauses in the medication preparation and administration workflow, typically due to interactions with other people (including other nurses, physicians or other clinicians, physical or occupational therapists, diagnostic technologists, dietary or environmental services personnel, unit secretaries, patients, and family members). Such interruptions often led to feelings of frustration. One exasperated participant described the effect of interruptions by saying,
“From mixing a medication in the med room to walking out of a med room to the patient's room, I could have 15 more interruptions and get sidetracked, and then administer [the medication] late.””
Another participant described how an interruption as she was preparing medications caused her to make an error, which, had she not caught it, could have had serious consequences:
“I had written the name of the medication on the label, but then another nurse started talking to me. I didn't even notice that the medication was not in the syringe.”
Nurse competency. This theme encompasses the knowledge and skills that support safe medication practices and how gaps in these areas can contribute to errors. Participants spoke of several competency-related factors, including clinical judgment, real-world experiences, the ability to recognize cues to double-check medications, knowledge in their own specialty area, and their own perceptions of error severity.
Participants offered many examples of how lapses in clinical judgment could have led or did lead to a medication error. They discussed the steep learning curve faced by new nurses transitioning to practice, who must quickly assimilate the skills necessary to prepare and administer medications safely in busy clinical settings. Some participants described situations in which a nurse might pay insufficiently close attention to orders, whether because of a chaotic unit environment or an erroneous assumption that frequently given orders will remain the same each time. In some instances, medication errors occurred because safe medication practices were inadvertently not followed. One participant offered this example:
“I've given [the] wrong insulin to the wrong patient. I . . . was too busy. There [were] procedures going on in . . . my other [patient's] room and I was trying to rush to try and get that done and instead of going into the right room, I went into the wrong room and gave insulin. No ill effects. I checked their blood sugar probably 20 times that day. It makes me feel stupid. It makes you feel like you failed your patient.”
Some participants also spoke of feeling that it was their responsibility to question a physician's orders when they knew the orders were incorrect. These nurses felt as if they were gatekeepers, tasked with keeping patients safe from harm, in addition to all their other daily duties.
For the purpose of this study, we considered nurses to have higher or lower competency based on one or more of the following: self-reported job tenure, highest completed education and training, and nursing skills. Nurses with higher competency levels had increased knowledge related to medications and medication practices in their specialty units. Nurses with lower competency levels, especially novice nurses, reported having trouble making decisions related to medication practices. One participant who worked on an orthopedic unit said that being familiar with common medication practices on that unit was useful in planning ahead, saying, “Since the orthopedic doctors typically give Ancef [cefazolin] for prophylaxis, I [know I] should anticipate seeing orders for Ancef post-surgery.” The participant was ready to request this antibiotic if it wasn't ordered. In contrast, some participants talked about how a novice nurse might not understand why a given medication was ordered for a patient, and whether it was appropriate for the patient in that clinical situation. One participant explained,
“I had one [medication order] the other night, just went back and questioned the doctor. I said, “Do you really want to give this? Because the patient is on Plavix.” And the doc went back and goes, “Hmm. Yeah, maybe we shouldn't.” It's just knowing your meds, and if you're not sure . . . make sure you look it up.”
Many participants felt that being able to apply both experience and critical thinking to medication practices was foundational to patient safety. As one participant shared,
“I had an extremely strong orientee, just [a] wonderful, critical thinker, had worked in another aspect of health care before she came to being a nurse, just thinking ahead, anticipating things she needed to do down the road during her shift.”
Several participants talked about how real-time cues reduced the possibility of errors and real-world experiences increased competency. One participant said that a dilution table on the automated dispensing cabinet helped her as she prepared medications: “It directs us to double-check it. I always use it.” Others talked about experiencing the real-world learning curve, and how gaining practical experience helped them integrate their knowledge and skills as they adjusted to their unit. Connections were made between “book knowledge” and “practical knowledge,” which are both critical to safe medication practices. One participant explained,
“In school, you recall that you learned about what to do when someone's blood sugar is too low. Then in the real world, “Oh, it's less than 45 [mg/dL], and I need to push something into them. Where do I get that? How do I do that?” You don't really get that in nursing school.”
Some participants spoke of how using poor clinical judgment or not using critical thinking, as well as inexperience, can contribute to situations that result in medication errors. One participant offered this example:
“The medication was given late at 11 AM but was originally ordered at 9 AM. A task on the MAR [medication administration record] appeared for administration of Zantac at 2 PM, and the nurse wasn't thinking. She saw a checkbox, so she went and gave another dose three hours later [which was too soon].”
In another example, a nurse wasn't aware of the risks of duplicative treatments, which can be dangerous to a patient. As the participant described,
“They didn't discontinue the Lovenox [enoxaparin] order, and the patient's on Eliquis [apixaban]—they can't have a second anticoagulant available.”
System influences refers to the hospital system's policies and procedures that impact nurses' workflow with regard to medication preparation and administration. Participants discussed both positive and negative system influences on medication safety. Positive influences included useful policies and procedures as well as collaborative teamwork. Participants offered examples such as systematic procedures for double-checking high-risk medications and for consulting with pharmacists about which medications could be crushed before administering through a gastrostomy or jejunostomy tube. Negative influences included EHR limitations, incorrect orders, automated dispensing cabinet device issues (such as nonworking indicators, incorrect restocking by a pharmacy technician), variations in medication deliveries to units, and inadequate communication or collaboration with other providers. Several participants voiced feelings of frustration and powerlessness when situations seemed beyond their control, and they discussed many such instances in detail.
For example, one systemic source of frustration was the lack of a clear process for delivering medications to a unit, which meant that medications weren't delivered in the same way every time. As one participant stated,
“There are three places we look for meds . . . we never know where they're going to be. . . . They hold us up [by this] delay in receiving meds.”
Another systemic source of frustration was the time wasted when waiting for a physician to return phone calls for orders to address a patient's abnormal laboratory values, such as an order for the electrolyte protocol. Furthermore, a lack of communication between primary and ancillary care teams (such as hemodialysis or radiology teams) made it difficult for nurses to think critically and strategize about when to give medications when the timing was affected.
A third example involved procedures for ordered tests, treatment schedules, and transfers. One nurse called medication administration a “moving target,” saying they never knew when to hold or administer certain drugs (such as β-blockers) because of the variable schedules of ancillary services. Lastly, participants discussed confusion caused by issues with the EHR, especially when patients came to their unit from the ED. For instance, medication orders are initiated for new patients upon admission to a unit. If a nurse can't readily locate in the EHR the time a medication was last given for a patient transferred from the ED, there is a risk of double dosing the patient. Many participants stated that this occurred frequently and was an added stressor.
The error paradigm refers to how nurses think and feel (their beliefs) about their personal decisions and actions (experiences) regarding medication safety practices and near misses or errors. This paradigm is influenced by the care environment, nurse competency, and the system. Some participants talked about how making an error affected their attitudes and actions in relation to medication practices, safety, and errors in general. These participants seemed to recognize the potential severity of their errors and used their prior experience with errors to change their own medication practices and reduce future risk. One nurse described starting a personal checklist for medication-related checks and habits. Another said that when she made or heard about an error, it made her more aware, and she consciously reflected on the error with the goal of preventing such errors in the future. She felt that this helped her to “be more focused and thoroughly read an order and not make an assumption just because I've seen an order a hundred times.”
Other participants talked about errors in a casual way and downplayed their potential severity. Some commented that nurses didn't report errors when they made them, and that practice deviations were generally acceptable and happened all the time. For example, on some units, it is common practice to crush medications even when doing so is contraindicated for a medication. Since it's common practice, this is never reported as an error. Another prevailing belief was that errors are acceptable if the potential outcomes from that error are not perceived to be severe. For example, one participant justified an instance in which insulin was not given because they were “too busy” to check the patient's blood glucose level. The patient's blood glucose subsequently rose “off the charts.” It was eventually lowered, but the participant downplayed the error, stating, “I don't think it's fatal, or it's not something that's really serious.” This was also their reason for not reporting the error.
Many participants seemed unsure about what an error was or could be. While all participants were able to define a medication error at the beginning of the interview, that definition seemed to become more ambiguous and less precise once discussion began. Through their experiences with making errors, many participants developed personal definitions that reflected their own perceptions of and self-judgments about error severity in subsequent situations. There were disconnects between participants' definitions of error and whether they admitted or accepted that an error had occurred on their units or in their own practice. Furthermore, many participants talked about how their perception of error severity played a role in whether they called a given error “an error.” One participant described her thinking by saying,
“If you give an extra dose of Tylenol [acetaminophen], do you consider that an error? I think a lot of it has to do with whether there is any harm to the patient. Sometimes it's like, “Well, it's still within the range,” even though you gave the wrong dose [than] was ordered.”
In her view, giving an extra dose of Tylenol didn't in itself constitute a concrete error; rather, she was guided by whether the dose could have or had resulted in harm to the patient. Throughout the interviews, this justification was heard repeatedly. There seemed to be a general complacency about such events, and an attitude that errors will happen anyway. Participants often felt powerless to prevent errors, as one said, “because mistakes happen. Mistakes can happen.” In addition, some participants knew that how they were handling such errors was wrong but did it anyway. They believed that if there was minimal impact to the patient, no efforts to report the error or correct the situation were necessary. As one participant stated, “Benign errors . . . are just ignored and not reported.”
See Table 2 for more examples of interview quotes by theme.
Table 2. - Examples of Participant Quotes by Theme Theme Quotes The care environment“What I feel mostly compromises medication safety on rehab is the workload because there's a lot of meds to administer. The patient teams are large . . . that makes the workload very high, which increases [the] stress level. Increased levels of stress definitely have the effect of causing people to take shortcuts in an effort to maximize time management.”
“So, after handoff report, the nurses will line up in Omnicell [an electronic medication management system] and give the meds. That is when it's hectic. And I think that the open[ing] for errors is then, when the nurse, instead of focus[ing] on pulling meds, they converse when they do the Omnicell. So it's easy to be distracted, pulling wrong meds because they don't look at the window that opens up, and they just grab the wrong medication.”
“Oh, just a lot going on during med pass. I've got this one patient's meds in front of me. I might be getting calls about another patient. I might have my tech asking me something. I might have family members coming up to me.”
Nurse competency“It's just the culture. Whatever the culture is, and especially new nurses, that's what they're gonna do. If they think it's okay to do work-arounds, then who's not gonna do that? Of course you're gonna do that.”
“I feel like nursing is actually involved with all the parts [of medication management], because it's the whole thing. I tell my new nurses that I don't ever want to hear [them] say, ‘The doctor ordered it. That's why I gave it.’ Because if they order it wrong—it's still our job to correct it. We give it to the patient, so it always comes back to the nurse.”
“I think the amount of new nurses we have right now overall is one of the leading factors. I think they don't have enough humility to ask for help. I think they think they know a lot more than they do. The only reason why I say that is because [while] getting handoff, you have an idea of what happened overnight and you're like ‘I wonder why they were still giving this lady her meds even though she can't physically say her name. Her voice is audibly garbled, can't really understand her, yet they're still giving her PO medicines.’ Did you really think that was a good idea?”
System influences“I work at night on med–surg. There is little interaction with whoever prescribed [the medication]. We have on-call nurse practitioners who don't like to do anything. They don't like to do anything, so if there is a problem, if I see something that doesn't make sense, I can page them and let them do nothing about it. Sometimes I'll call pharmacy. They're actually more helpful. [I can ask] ‘Should I give this? Should I not? What should I do?’ Because those nurse practitioners, they don't want to change anything. They don't want to make a decision. They don't. Sometimes they'll be like, ‘Okay. Well, I'll talk to the provider.’”
“I feel like the IDV [identity verification] process has really slipped back. I feel like, not with everybody, but IDV-ing does not really occur properly. Because many of the errors are IDV meds. Clearly, it was not IDV-ed by two nurses.”
“Some of those physicians in some of those specialty areas, they're a little bit more fine-tuned when it comes to writing their pain prescriptions. But then you have [an internist] that sometimes is a little bit more lenient. You'll have a patient with pain medication options of Tylenol [acetaminophen] and ibuprofen, and they both have the same mild indication, and it's like, which one do I pick? At that point, it's like, okay, which one does the patient prefer? Based off of what they're telling us with regulatory and all this stuff, we shouldn't have multiple options, because at that point, it's like we're playing physician.”
The error paradigm“We have to do a lot of self-checks and balances to make sure that everything is being done appropriately for the specific patient that we're caring for.”
“I think that some of the med errors that are perceived as benign, so to speak, are just ignored and not reported.”
“I guess we're just gonna have to have med errors. I tried.”
“There's definitely work-arounds, where if you're a nurse, you can find one for anything.”
“I would say that's probably why, unfortunately, errors occur too, because—and it's not your fault, but it's just everybody now, especially having the [bar code–assisted medication scanning], we all think, ‘Oh, this is a safeguard,’ so we're not as cautious—because we think that the system's supposed to prevent the error.”
This qualitative research study is one of the first in the United States to explore the medication safety practices of nurses. Our interviews with participants elicited rich data from which four themes emerged: the care environment, nurse competency, system influences, and the error paradigm.
In the care environment, participants depicted frequent chaos, heavy nursing workloads, and distractions and interruptions as increasing the risk of medication errors. These findings are congruent with results from prior studies, which found safe medication preparation and administration to be adversely affected by these factors, among others.1, 14-16 Indeed, a recent qualitative systematic review by Schroers and colleagues found that distractions and interruptions were the most common contextual causes of medication errors.17 Frequent distractions and interruptions interfere with medication preparation and administration processes, adding to the nursing workload and increasing the risk of mistakes.18 Ironically, it's most often nurses and other health care professionals who are the source of distractions and interruptions.19, 20 High patient acuity levels and inadequate unit staffing further exacerbate the nursing workload.1, 15
Regarding nurse competency, we found that medication safety practices were adversely affected by lapses in clinical judgment and by the steep learning curve new nurses face in transitioning to practice. Gaining practical medication knowledge can be difficult, and even experienced nurses may lack sufficient skills to ensure safe medication management, especially when ongoing educational reinforcement and support are lacking.17, 21 More experienced nurses have been shown to make fewer medication errors than less experienced nurses; novice nurses in particular need a high degree of medication management education and support.1, 11, 22 In order for nurses to develop and maintain high levels of competency in medication safety practices, organizations must support them by providing adequate and ongoing education, training, and mentorship.
In this study, system influences that adversely affected participants' ability to safely prepare and administer medications included insufficient policies and procedures, poor resource availability, inconsistent medication delivery, and incorrect physician orders. These findings are similar to those of prior research. Several studies have found that ineffective or impractical policies and procedures, as well as unclear physician orders, contribute to medication errors.1, 14, 15, 23 The qualitative systematic review by Schroers and colleagues found that nurses perceive insufficient protocols, a lack of guidelines, and poor equipment design as contextual factors that lead to medication errors.17 Poorly designed unit workspaces and “problematic” organization of medication supplies have also been identified as factors that contribute to medication errors.24
The error paradigm—the influence of participants' beliefs and experiences on their medication practices—emerged as the fourth theme in our study. While some participants developed personal checklists as safeguards against future medication errors, others seemed uncertain or complacent about what really constituted an error. Notably, the proactive use of self-checking appears unique to our study, although many studies cite the use of double-checking with other nurses (either together or independently in pairs) as a medication safety practice.25-27 The presence of complacency, a casual attitude, and a tendency to make assumptions regarding medication safety practices have also been noted in the literature.17 For instance, misunderstandings about what constitutes a medication error, especially errors of omission such as missed doses, have been shown to adversely impact error reporting.14 Similarly, giving a medication at the wrong time has been seen as “flexibility” rather than as an error.28 These perceptions are in keeping with the varying perceptions of and self-judgments about error severity that were evident in many of the interviews.
Strengths and limitations. This qualitative descriptive study is one of the few U.S. studies to focus on the medication safety practices of nurses; moreover, the sample consisted only of direct care nurses. Thus, we were able to elicit the rich perspectives of those who actually prepare and administer medications in the clinical setting.
A main limitation of the study was that not all of the hospitals within the health care system of interest were represented. The results might not reflect the full spectrum of opinions and experiences of nurses across the organization. Another limitation is that study participants self-selected by volunteering for interviews. It's possible that the nurses who volunteered might naturally be more conscientious in their medication practices than those who didn't volunteer.
Implications for practice. Medication practices are influenced by myriad factors at many levels from the individual to the organizational, as the four emergent themes indicate. Our in-depth discussions with direct care nurses allowed for a comprehensive and robust examination into their perspectives on and experiences with medication management in practice, including instances of errors and near misses. What was missing from the discussions was evidence that the participants understood how those factors worked together to support or impede safe medication practices within the hospital health care system. Gaining a deeper understanding of both specific factors and their complex interplay is essential to identifying opportunities for improvement.
In the interviews, participants described chaotic care environments and countless daily distractions and interruptions. It is imperative that hospitals create care environments that better support medication safety practices. Determining ways to reduce distractions and interruptions (especially during high-volume medication times) and teaching nurses strategies for dealing with such disruptions should be prioritized. Innovative approaches such as simulation-based education can be used to teach nursing students and novice nurses interruption management skills.29 The ability to manage interruptions has been shown to lower nurses' sense of overwhelm, decrease risk of error, and improve practice efficiency.29 Addressing environmental aspects such as the location of and noise levels in medication rooms can also be helpful.
Heavy nursing workloads augmented the stress and chaos that participants described in the interviews. Organizations must closely examine whether current nursing workloads can safely be allowed to continue unchanged. There is abundant evidence that heavy workloads lead to cognitive fatigue, physical exhaustion, and subsequently higher medication error rates.17 Innovative or alternative care delivery models that take this into account are urgently needed.
More robust education and training that respects nurses' medication management processes, addresses medication errors and near misses, and incorporates available resources (such as clinical pharmacists and online databases, among others) should be provided. Furthermore, organizations must critically assess their unique structures and processes in terms of how these impact nurses' medication competence. A recent concept analysis of medication competence defined it as “a comprehensive skill that develops from the assimilation of pharmacology knowledge, pathophysiology and anatomy awareness, pharmacogenetic integration, medication calculation and administration skills, clinical judgment, collaboration, and utilization of information technology.”30 A systematic literature review found that improving nurses' knowledge of and attitudes toward patient safety and practice errors could improve their adherence to patient safety principles, thus leading to better outcomes.31 In particular, as our findings indicate, nurses must have a solid understanding of what constitutes a medication error and its potential consequences. All of this provides a foundation from which to build organization-specific nursing education and training that can be integrated into onboarding and yearly competency practicums.
From a systems perspective, organizations should encourage and facilitate the active participation of direct care nurses in medication management committees. These committees typically discuss errors and near misses, address changes to medication-related structures and processes, discuss policy and guideline development, and often play a role in planning the construction of new units or hospitals. Input from direct care nurses is essential, as these nurses are most familiar with the day-to-day intricacies of medication preparation and administration, and their input can stop organizations from creating new policies or procedures that aren't feasible in real-world nursing. Nurse engagement in quality improvement projects that concern medication management is also vital to achieving optimal outcomes. To these ends, nurse leaders should strive to build a workplace culture that supports nurses in calling attention to issues without fear of retribution.32
CONCLUSIONSThe complexity of medication safety practices makes it difficult to implement improvement strategies. In exploring direct care nurses' experiences with medication safety practices and errors, this study offers a glimpse into real-world medication management from the nurse's unique perspective. The four emergent themes—the care environment, nurse competency, system influences, and the error paradigm—overlap and interact, demonstrating the complexity of medication practices within a hospital health care system. Nurses clearly have an integral role in this aspect of care and most can perform with competence. Yet we found that in challenging, real-world situations, some nurses will override or circumvent certain medication safety practices in order to “get things done.” This discovery should inform future research that explores how to untangle the medication administration process and better prevent errors.
Taken together, the study findings suggest numerous areas for improvement to current medication practices. Potential strategies should include actively addressing environmental barriers to safe medication practices, ensuring more robust medication management education and training (including guidance regarding the importance of adhering to the definition of medication errors and of reporting errors), and revising policies and procedures with input from direct care nurses. More research is needed to determine how to positively impact the workplace culture, care environment, and error paradigm, support the work of and encourage input from direct care nurses, and guide organizational leaders in revising relevant policies and procedures.
Comments (0)