
Remember me







Since the inception of the patient safety “movement,” efforts to improve patient safety within hospitals have relied heavily on the retrospective investigation of adverse events.1 Retrospective incident investigations as a mechanism for safety improvement are founded on an interpretation of safety theory, which proposes that errors are multifactorial in nature and that identifying and addressing organizational latent failures through investigation and recommendations will reduce future recurrence.2,3
In recent years, the generation of recommendations, after incident investigations, has come under increasing academic scrutiny.4–7 This interest has occurred in parallel with the establishment of national-level independent investigatory bodies (e.g., HSIB in the UK, Norwegian Healthcare Investigation Board in Norway),8,9 and in the UK, an ever increasing number of public inquiries and the ever expanding set of associated recommendations (e.g., Kirkup,10 Ockenden,11 Infected Blood Inquiries12). Therefore, exploring the act of recommendation generation is of increasing relevance as the number of recommendations across both local and national level investigation activity grows exponentially.
Although there are a plethora of aims and processes for investigations, a consistent feature is the production of recommendations. Despite 3 decades of incident investigation activity in health care,13 few studies have critically examined the process.5,14 In addition to the lack of empirical work examining recommendation generation, there is a lack of practical guidance, on the generation of recommendations.6 One systematic review used a modified version of the National Institute for Occupational Safety and Health hierarchy of risk controls to categorize the recommendations from included studies,5,15 concluding that 80% of recommendations were “weak,” that is, unlikely to result in significant improvements in safety or risk reduction. Furthermore, Hibbert and colleagues16 undertook a retrospective study, following investigations within an Australian regional health system. The study used and modified the U.S. Department of Veteran Affairs action hierarchy (AH) to categorize recommendations as strong, medium, or weak and concluded that only a small number of recommendations were strong and the most common types of recommendations involved reviewing or enhancing policies/guidelines/documentation as well as training and education.16 It is important to note that these issues extend beyond health care. Indeed evidence suggests that a lack of guidance and a plethora of other sociotechnical factors impede the generation, implementation, and evaluation of recommendations across safety investigations in contexts such as rail, maritime, and nuclear.6,17
Recommendation Generation Within Local Health Care InvestigationsDespite the centrality of incident investigation and recommendation generation within patient safety policy globally, there is a surprising lack of understanding about what actually happens in local health care settings with respect to this important activity. In particular, there is a lack of empirical focus and consensus about recommendation generation by people conducting investigations at a local health care organization level.4,13 This review therefore aims to examine the extant empirical knowledge about this issue. We have focused on hospital settings rather than primary/community care because of the fundamentally different ways in which care is delivered and case mix,18 as well as the relatively lower level of incident reporting and relevant published literature in primary care.18–20
Scoping Review AimsThe purpose of this review was to consider the following questions:
What approaches to incident investigation are used before the generation of recommendations? What are the processes for generating recommendations after a patient safety incident investigation? What are the number and types of recommendations proposed? What criteria are used, by hospitals or study authors, to assess the quality or strength of recommendations made? METHODSWe conducted a scoping review, following the preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews guidance.21
Sources and SearchesSearches were performed on February 28, 2019, and January 30, 2021, using MEDLINE, EMBASE, PsychINFO, and CINAHL. Search terms were iteratively developed to capture the key phases of incident investigation including terms for the incident, investigation, and subsequent recommendations (see Appendix 1 for search terms, https://links.lww.com/JPS/A565). Searches were restricted to English language and studies published since 1999, when the Institute of Medicines’ seminal report, To Err Is Human, was published,22 prompting greater focus on patient safety.
Study SelectionThe aim of this review was to examine the routine investigation and recommendation generation processes that occur in hospitals.
Studies were included if they reported on a series of incidents occurring in the hospital, which were chosen for investigation by hospital-based staff, who also generated subsequent recommendations. Studies reporting on incidents from any clinical context or level of harm were included.
Studies were excluded if they reported data from the following:
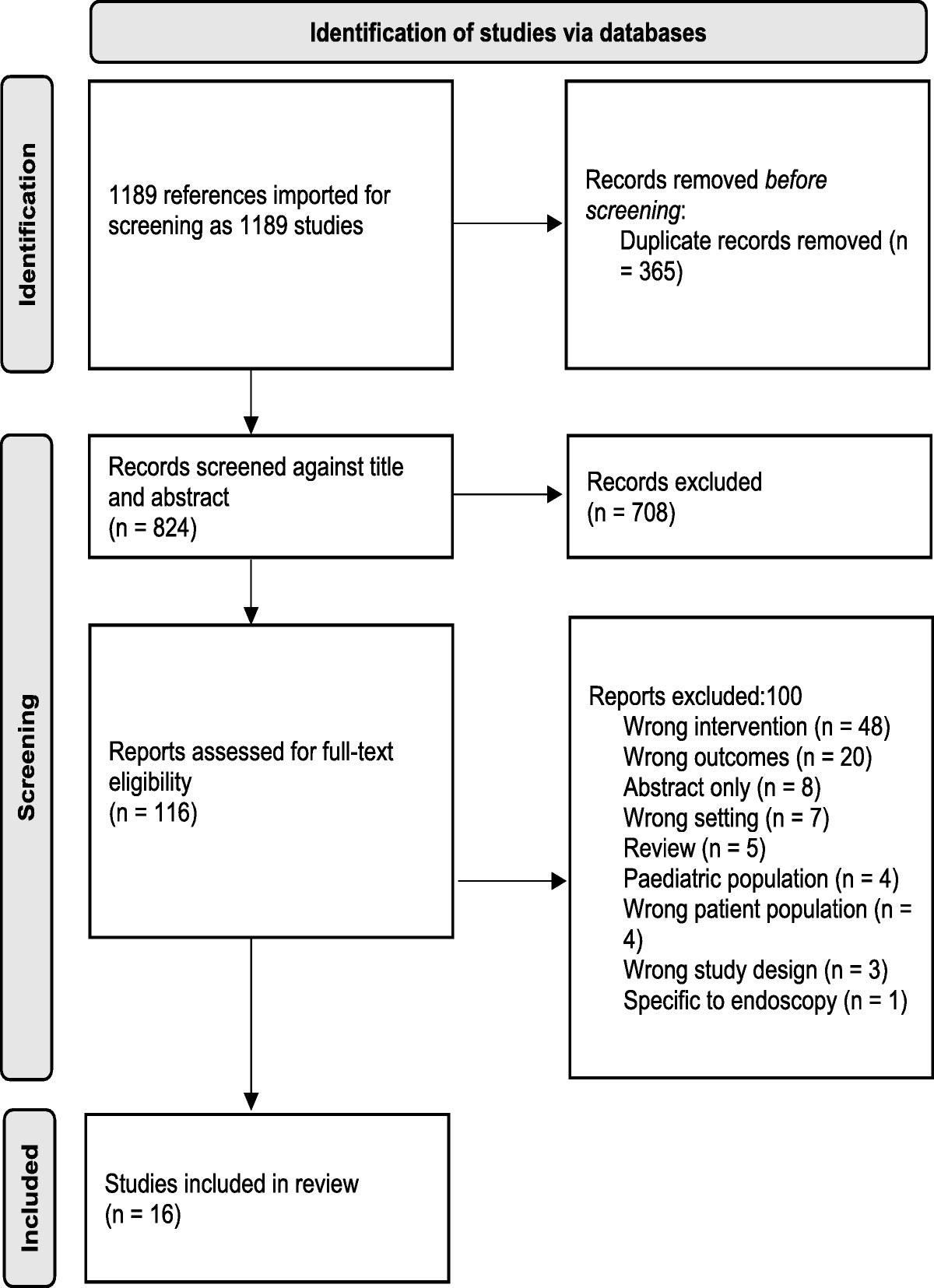
Community, primary care, or primarily mental health care Investigations/recommendations carried out or proposed outside of a hospital, for instance, by an external research team or regional organization Investigations primarily carried out for the purposes of research Not published/peer-reviewed (e.g., conference papers)Searches yielded 15,010 articles. The article title and abstracts were reviewed by W.L. Random samples of 5% (n = 720) were screened independently by both J.O.H. and R.L. to check congruence. A total of 246 articles were selected for full-text review. Full-text screening was undertaken by W.L., with 10% independently screened by each of J.O.H. and R.L. (n = 20). Any discrepancies were discussed and resolved between authors. Eleven articles met the inclusion/exclusion criteria (all agreed with W.L., J.O.H., and R.L.) and contributed to the review (Fig. 1). Regular meetings with the other author (C.V.) allowed discussion of article eligibility.
 FIGURE 1:
FIGURE 1: PRISMA-ScR flow diagram for study selection.
Data Extraction and Quality AssessmentThe purpose of the review was to examine the nature of recommendations proposed within hospitals, which was not the primary aim of all the included studies, but those included did contain empirical data on recommendations.
We assessed study quality using the Quality Assessment for Diverse Studies (QuADS) tool.23 This tool is a well-cited approach to assessing the quality of methodologically heterogeneous studies, which demonstrates reliability and validity.23,24 After discussion of the application of the tool and relevance of quality scoring by all the authors, W.L. reviewed and scored all included articles. A random sample (n = 4 [36%]) of studies were independently reviewed and scored by J.O.H. and R.L., with disagreements resolved with discussion.
Data Synthesis and AnalysisTo address research questions 1, 2, and 4, we undertook content analysis of the included studies using 4 stages; decontextualization, recontextualization, categorization, and compilation.25 First, authors read and made themselves familiar with the included studies before extracting “meaning units” of text relevant to answering the aims of the review (decontextualization). After extraction of meaning units, the remaining article text was checked for further relevant content (recontextualization). Next the extracted meaning units were split into specific areas relevant to each research question; the word count was reduced without losing the meaning/content (categorization). The research questions were answered by condensing the extracted text using the original study terms and language, as well as providing numerical counts of how often content was reported across the studies.
To address research question 3, we used the AH, proposed by the U.S. Veteran Affairs National Center for Patient Safety to categorize the recommendations extracted from included studies.16,26–29 Recommendations from the included studies were discussed by all the authors across 2 meetings and assigned to the core categories of the AH, then counted, to report frequency. If, after discussion, it was felt that a recommendation or category of recommendations did not fit into one of the AH categories, a new category was created and agreed.
RESULTSThe characteristics of included studies (n = 11) are summarized in Table 1. Included studies contained 4680 recommendations from 2818 investigations carried out across 171 hospitals.
TABLE 1 - Summary of Included Studies Author (Year) Reference No. Country Clinical Context No. hospitals No. Incidents Analyzed Types of Incident(s)/Incident(s) Relating to Levels of Harm of Investigated Incident(s) No. recommendations How Are Recommendations Categorized? Corwin et al (2017) 30 United States Intensive care 47 70 Delay in care; medication; medical procedure; equipment failure; removal of lines, catheters, tubes, drains; transfusion, elopement; discharge; suicide attempt; fall; airway/ventilation Incidents causing harm only 276 Categories developed by authors based on included investigations recommendations Figueiredo et al (2018) 31 Brazil Tertiary general hospital 1 1316 Drug supply chain; fall; pressure ulcer; other skin lesions; surgical procedure (relation with laterality); transfusion process; unplanned withdrawal of catheter, drain, tube or catheter; Identification of patient; loss of sample; bruise; extravasation; delay in exam/procedure completion; prolonged fasting; failure to release the technical report; evasion; technical or equipment/material handling failure; failure to identify material/instruments; related to childbirth; nutritional therapy; health care related infection; failure during technique, procedure or transportation; death and others No harm and harm incidents included 1326 Categories developed by authors based on included investigations recommendations Hamilton et al (2019) 27 Australia Hospitals/pediatric 16 42 Delayed diagnosis; delayed recognition or response to a deteriorating patient; procedural adverse event; patient identification or procedure mismatching; medication adverse event; delayed definitive treatment; unexpected death/event after hospital presentation or admission; testicular torsion delayed diagnosis or management Incidents causing harm only 150 U.S. Department of Veteran Affairs’ criteria, or AH (VA AH) Hibbert et al (2018) 16 Australia Hospitals in region 36 227 Clinical process/procedure; falls; behaviors; problems with diagnosis; problems with procedures or interventions; wrong patient/body part; inpatient suicide; retained instruments/other; gas embolism; ABO incompatible blood transfusion; medication error; maternal death; wrong infant discharged Incidents causing harm only 1137 U.S. Department of Veteran Affairs’ criteria, or AH (VA AH) Irwin et al (2011) 32 United Kingdom Hospitals in region/pharmacy 23 573 Dispensing of medications No harm and harm incidents included 251 Categories developed by authors based on included investigations recommendations Kellogg et al (2017) 33 United States Academic Medical Centre 1 302 Procedure complication; cardiopulmonary arrest; neurological deficit; retained foreign body; pulmonary/arterial embolus; birth complication; medication administration error; incorrect procedure/study; sepsis; wrong-site surgery/procedure; devastating illness; myocardial infarction; hemorrhage/hematoma; arrhythmia; unknown cause of death; adverse medication event; compartment syndrome; fall, inpatient; event proximate to discharge; self-harm; electrolyte disturbance; assault, inpatient; bowel perforation; equipment failure; sleep apnea; ventilation complication No harm and harm incidents included 499 Categories developed by authors based on included investigations recommendations Kwok et al (2020) 28 Hong Kong Hospitals in region 43 214 Surgery/interventional procedure involving the wrong patient or body part; retained instruments or other material after surgery/interventional procedure; ABO incompatibility blood transfusion; intravascular gas embolism resulting in death or neurological damage; death of an inpatient from suicide; maternal death or serious morbidity associated with labor or delivery; infant discharged to wrong family or infant abduction; other adverse events resulting in permanent loss of function or death; medication error which could have led to death or permanent harm; patient misidentification which could have led to death or permanent harm No harm and harm incidents included 760 U.S. Department of Veteran Affairs’ criteria, or AH (VA AH) Morse and Pollack (2012) 26 United States Pediatric hospital 1 20 Medication event; delayed identification of clinical deterioration; equipment failure; enteral feeding via central line; breast milk event; unsterile surgical equipment; inappropriate patient behavior in the “play room”; significant tissue injury; name change patient identification; readmission event; wrong site MRI under general anesthesia No harm and harm incidents included 78 U.S. Department of Veteran Affairs’ criteria, or AH (VA AH) Robbins et al (2020) 34 United Kingdom University hospital 1 22 No details Incidents causing harm only 101* Hierarchy of intervention effectiveness (people versus system focused) (Cafazzo and St-Cyr35) van der Starr et al (2014) 36 The Netherlands Neonatal/pediatric intensive care 1 17 Medication errors; procedural; unanticipated death, unanticipated resuscitation; nursing care No harm and harm incidents included 84 Factors influencing clinical practice devised by Woloshynowych et al3 Zeng et al (2016) 37 United States Hospital 1 15 Reported most common: communication failure between team members; tasks to automate for dosimetry; simulation issues; IT system failures; scheduling issues No harm and harm incidents included 18 Categories developed by authors based on included investigations recommendations Total 171 2818 4579 *Lacked detail to enable categorization and therefore not included in Table 3.Included studies were conducted in the United States (n = 4), the United Kingdom (n = 2), and Australia (n = 2), with one each from the Netherlands, Brazil, and Hong Kong.
Clinical Context and Incident HarmStudies reported data from across all clinical specialties (n = 6), pharmacy/medication (n = 1), anesthesia and intensive care (n = 2), and pediatric care (n = 2). Incidents reported within studies varied in their type (e.g., delay in care, fall, dispensing of medication) and resulting harm (see Table 1 for more detail).
Quality AssessmentThe included studies demonstrated an average QuADS score of 56% (range, 26%–69%) Five of 11 studies lacked theoretical underpinning such as the discussion of an accident causation model. Half of the studies did not report, in sufficient detail, the justification of sampling or selection of data collection tools. Six studies had no evidence that research stakeholders had been involved in their planning or conduct. Four studies had limited or no discussion of their strengths or limitations. No studies were excluded based on quality.
RQ1) Approaches to Incident Investigation Used Before the Generation of RecommendationsNine studies reported using root cause analysis (RCA),16,26–28,30,33,34,36,37 3 used both RCA and the London Protocol,16,36,37 and the remaining 2 used no specific tool or method.31,32 Four studies reported that a team of 2 to 8 staff (physicians, nurses, and managers) undertook the investigation,28,33,36,37 and 2 reported specific investigator training.34,36 The remaining studies did not provide these details.
As part of the investigation process, 3 studies reported interviewing staff,33,36,37 one of which specified that incidents were reconstructed from a median of 6 interviews (n = 3–15).36 One study reported that parents of children involved in incidents were interviewed “if felt to be useful,” and this occurred in 2 of 17 incidents.36
Four studies reported on the time spent undertaking investigations. This was highly variable, ranging from 3 to 90 hours.26,34,36,37 Three studies reported that investigations should be completed within a set period of time, ranging from 30 to 60 days,28,30,33 although they did not specify if this was from when the incident occurred or was reported, or the decision to investigate was made.
RQ2) The Processes for Generating Recommendations After A Patient Safety Incident InvestigationNone of the included studies reported using specific tools or methods for recommendation generation. One article reported that staff and parents were invited to suggest recommendations, whereas none of the remainder reported this kind of stakeholder involvement.36 Eight studies proposed that recommendations should prevent incident recurrence16,27,28,30,33,34,36,37 and eliminate, mitigate, or reduce a risk, hazard, or “root causes.”28,30,33,34 No purpose or aim for recommendations was stated in the remaining 3 studies.
RQ3) The Number and Types of Recommendations ProposedA variety of terms were used to describe the recommendations generated after investigations. We present these terms in Table 2, but because the terms were not clearly defined within the studies, we were not able to determine differences or similarities and have therefore reported them as written. A total of 4579 recommendations were extracted from 10 included studies (Table 3), with an average of 3.7 (1–5) per investigation. Recommendations were not extracted from the 11th included study because of insufficient detail to enable categorization.34 Six studies assigned recommendations to predetermined categories based on (i) the U.S. Department of Veteran Affairs’ criteria or AH,16,26–28 (ii) factors influencing clinical practice devised by Woloshynowych et al,3,36 or (iii) the “hierarchy of intervention effectiveness” (people versus system focused).34 The remaining 5 studies developed their own categories based on analysis of their included recommendations.30–33,37
TABLE 2 - Terms Used to Describe the Recommendations After Investigations Frequency Study Reference Recommendations 5 Hibbert et al,16 Hamilton et al,27 Kwok et al,28 Corwin et al,30 van der Starre et al36 Action(s) 5 Kwok et al,28 Corwin et al,30 Figueiredo et al,31 Kellogg et al,33 Robbins et al34 Action plan(s) 2 Morse and Pollack,26 Zeng et al37 Corrective actions/action plans 2 Morse and Pollack,26 Robbins et al34 Solutions 2 Kellogg et al,33 Robbins et al34 Process improvements 1 Zeng et al37 Interventions 1 Irwin et al32 Risk reduction strategies/measures 1 Morse and Pollack26 Preventative measures 1 van der Starre et al36 Recommended actions 1 Corwin et al30 Managerial responses 1 Irwin et al32 Error management strategies 1 Irwin et al32 Risk controls 1 van der Starre et al36 Process improvement projects 1 Zeng et al37
Comments (0)