
Remember me







Accidental falls are the most common patient safety incidents in acute care settings. According to the Korea Patient Safety Reporting and Learning System, 45.7% of 62,408 voluntarily reported safety accidents that occurred between July 2016 and September 2022 in South Korea were falls. Several efforts to prevent and predict falls in Korea have used health information technology. Particularly, a research group at study hospital, a leading global digital hospital that is a Healthcare Information and Management Systems Society Analytics Stage 7 institution, has attempted to reduce accidental falls using information technology. For example, they developed fall risk prediction models based on electronic medical record (EMR) data and compared them against the performance of a tool traditionally used to assess patient fall risk.1,2
Computerized decision support systems (CDSSs) are designed to aid clinical decision making and link patient characteristics to a computerized knowledge base, thus enabling patient-specific recommendations.3 They can improve adherence to clinical practice guidelines (CPGs) and access to medical or health knowledge at the point of care. Moreover, they can increase the accuracy of screening and diagnoses, reduce medical errors, and enhance the quality of documentation, referrals, and efficiency. For instance, a previous synthesis of systematic reviews reported that CDSSs improve medical staff performance as well as adherence to clinical processes.4,5
Randell et al6 conducted a systematic review of CDSS use in nursing practice, based on 8 studies. They found that such systems have had an inconsistent effect on nursing performance and patient outcomes. Another systematic review of 28 studies reported that nursing DSSs improve compliance with recommendations and reduce decision time. However, the impact is not always consistent, particularly regarding patient outcomes.7
Dykes et al8 developed the fall Tailoring Interventions for Patient Safety (TIPS) CDSS to generate an evidence-based care plan according to the unique risk factors affecting each patient. The goal of the system was to enable patients to easily understand their risk factors and fall-prevention care plan regardless of their literacy level. The fall TIPS was subsequently found to reduce falls by 15% to 25% and fall-related injuries by 34% in a series of clinical trials.8,9 Thus, this nurse-led, patient-centered program, which was based on actionable factors, efficiently prevented falls.10 In 2015, Duke University Hospital implemented a CDSS to enhance documentation of fall risk assessments and fall-prevention care plans as well as to reduce patient falls and injuries.11 Overall, the implementation had an inconsistent effect: the documentation of fall risk assessments improved significantly, but there were no changes in clinical outcomes such as patient falls and falls with injury rates.
AIMS AND OBJECTIVEWe developed a CDSS that automatically calculates the risk of falls using EMR data and provides evidence-based fall-prevention recommendations based on risk factors at the point of care. We implemented the CDSS and analyzed its impact in terms of usability, changes in fall-prevention nursing practices, and number of falls that occurred.
MATERIALS AND METHODSThe CDSS for fall prevention was developed in 2 phases. Phase 1 involved the development of fall risk prediction models, whereas phase 2 involved the combination of CPGs, prediction models, and EMR data to produce tailored recommendations for fall prevention (Fig. 1). The process and results of phase 1 were described in a previous study.2
 FIGURE 1:
FIGURE 1: Computerized decision support system for fall prevention.
The CDSS for fall prevention was developed according to the 5 stages of the system development life cycle: (1) requirement and knowledge analyses by group interviews, (2) CDSS design informed by the requirement analysis, (3) development of a knowledge base and data extraction queries, (4) implementation and application of the CDSS in a study ward, and (5) evaluation of the impacts of the CDSS based on usability, changes in fall-preventive nursing practices, and the number of falls that occurred.
Requirement and Knowledge AnalysesFor the requirement and knowledge analysis, we conducted group interviews to assess user expectations about the knowledge and functions of the CDSS. In the interview, 3 of the 21 nurses who were recruited to use the CDSS in the study ward responded to 4 questions: (1) How do you predict or assess the risk of falls and how do you prevent falls in a clinical setting? (2) What type of information do you want the CDSS to provide? (3) What types of functions or features do you want the CDSS to have? (i.e., user interface specifications), and (4) Do you have any preferred user interface designs for the CDSS? The feasibility of integrating the users’ functional requirements into the clinical flow and EMR was examined by a team including nurse supervisors, a hospital chief information officer, and systems developers from EMR vendors.
Design and DevelopmentFigure 2 shows a use-case diagram to demonstrate different ways in which users might interact with the CDSS based on the group interview and feasibility examination.
 FIGURE 2:
FIGURE 2: Use-case diagram of fall-prevention CDSS.
Before designing and developing a CDSS that linked EMR data with existing knowledge, we developed a prototype that incorporated the functions and interfaces that were indicated by the users as desirable.12 Although the prototype was not able to use real patient EMR data to calculate the risk of falls in real time, it provided tailored recommendations according to patient risk factors and helped users to document their interventions. Knowledge for fall prevention was extracted from the CPGs published by the Agency for Healthcare Research and Quality, the National Institute for Health and Care Excellence, the Registered Nurses’ Association of Ontario, the Ministry of Health of Singapore, and Korean Hospital Nurses Association. The knowledge was listed by risk factor. Three nurses assessed the clinical applicability of the knowledge. There was fair to good agreement (interrater reliability = 0.586) among the three nurses. For knowledge that was judged by more than 1 of the 3 nurses as inapplicable to the clinical setting, the head nurse decided whether to include that knowledge in the CDSS. In total, the knowledge base included 37 tailored interventions related to risk factors, 6 tailored interventions for patients with a high risk of falling, and 20 nonspecific interventions applicable to all inpatients.
The intervention knowledge was mapped to standardized nursing statements for our analysis of the effect of the CDSS. In cases where there were no standardized nursing statements to represent knowledge, we created new nursing statements. In total, 63 interventions were mapped to 80 existing standardized nursing statements and 18 newly created nursing statements.
Microsoft Visual Studio, NET, and Oracle 11 g were used for application development and database management.
ImplementationThe fall-prevention CDSS was implemented as a 1-way system that could extract the patient’s real-time data from the hospital information system (HIS) to calculate the risk of falls and provide tailored recommendations according to patient risk factors, but could not transmit data generated by the CDSS to the HIS. The CDSS was used between March 21, 2019, and August 31, 2019, in one of the inpatient wards with the highest prevalence of falls. Nurses were trained twice on the CDSS functions and how to use them. Nurses were encouraged to use the CDSS and to provide nursing interventions according to the recommendations offered by the CDSS.
Evaluation Usability TestOne month after the CDSS was introduced, the nurses evaluated its usability via the Usefulness, Satisfaction, and Ease of Use questionnaire. The Usefulness, Satisfaction, and Ease of Use is a 30-item survey that examines 4 dimensions of usability, namely, usefulness, ease of use, ease of learning, and satisfaction.13 The nurses assessed usability using a 7-point Likert scale (1, strong disagree; 2, disagree; 3, somewhat disagree; 4, neutral; 5, somewhat agree; 6, agree; 7, strong agree) in this study.
Changes in Fall-Prevention Nursing PracticesWe examined changes in nursing practices for fall prevention and the number of falls before and after CDSS implementation, as shown in Figure 3. Changes in fall-prevention practices among the nurses were assessed via 2 methods: (1) a survey to capture the time spent on nursing care for fall prevention and (2) an analysis of nursing documentation in the electronic nursing records (ENR). According to the nursing process (i.e., assessment, diagnosis and plan, intervention, and evaluation), the survey investigated the amount of time spent on nursing care for fall prevention to identify which activities the nurses spent the most time on. Changes in the frequency of fall-prevention practices before and after CDSS usage were analyzed by counting the mean frequency of documented fall-prevention interventions per day. Because the patterns of nursing practices for fall prevention were different between the high-risk and low-risk groups of falls in a previous study,14 changes in nursing documentation and time spent on nursing care for fall prevention before and after CDSS implementation were analyzed by dividing patients into high-risk and low-risk groups. The standardized nursing statements were mapped to knowledge from the CPGs and then categorized and analyzed according to intervention type, as in a previous study.14
 FIGURE 3:
FIGURE 3: Indicators used to evaluate the impact of the CDSS.
The pre-CDSS observation period was from July 1, 2017, to June 30, 2018, and the post-CDSS observation period was from March 21, 2019, to August 31, 2019. We included nursing documentation for patients who stayed in the study ward for more than 2 days in the analysis.
Number of FallsWe identified and compared the number of falls among patients admitted to the study ward during the pre-CDSS and post-CDSS observation periods. A fall patient was defined as any patient with a fall accident registered in the incident reporting system, or with any of 9 fall-related standardized nursing statements such as “fall,” “collapsed,” and “slipped and fell” in nursing documentation.1,2,15 Fall-related nursing statements were verified by 1 head nurse and 2 nurses in the study ward.
Data AnalysisThe characteristics of nurses and usability of the CDSS after 1 month of use were summarized using descriptive statistics. We used an independent t test to compare the amount of time spent engaged in nursing care for fall prevention and the mean frequency of documented fall-prevention practices per day before and after using the CDSS. The mean frequency of fall-prevention nursing practices per day was computed as the number of aggregated nursing statements according to the intervention type (nonspecific intervention versus tailored interventions based on risk factors) divided by the length of stay for each patient. Moreover, the study patients were divided according to whether they were at high or low risk of falling, and the differences in nursing practices were compared between the 2 groups. The high-risk group included participants who had been classified as having a high risk of falling at least once during their hospitalization period. The statistical significance was set at P < 0.05 and calculated using a 2-sided test. R software (version 3.6.3; R Foundation for Statistical Computing, Vienna, Austria) was used for the analyses.
Ethical ConsiderationsThis study was approved by the institutional review board (IRB) of the study hospital (IRB No. B-1810/499-304) and performed according to the relevant guidelines and regulations of the IRB.
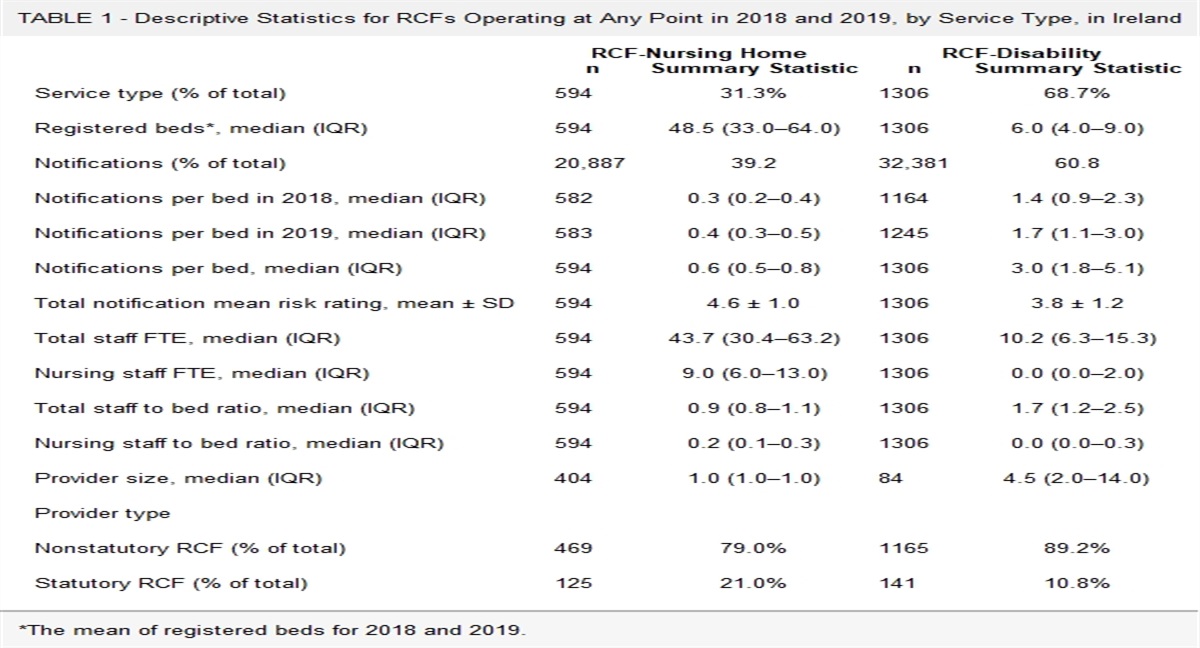
RESULTSAll 21 nurses in the study unit participated in the usability test. Among them, 12 nurses participated in a survey investigating the time spent on fall prevention before using the CDSS and 14 nurses completed a survey after using the CDSS. Table 1 shows the characteristics of the nurses. In particular, the average age of the nurses was 31 years, and they had an average of 7 years of clinical experience.
TABLE 1 - Characteristics of Nurses Involved in This Study Characteristics No. (%) Sex: female 21 (100.00) Age, y 21–25 3 (14.28) 26–30 9 (42.86) 31–35 4 (19.05) 36–40 5 (23.81) Clinical experience <5 y 11 (52.38) Between 5 and 10 y 4 (19.05) >10 y 6 (28.57) Position Nurse 19 (90.48) Charge nurse 1 (4.76) Head nurse 1 (4.76)Table 2 presents the usability data, which were collected after the nurses had used the CDSS for 1 month. The average score for the ease of learning was the highest among 4 dimensions. Of 30 items, the item asking about whether using the system was “fun” within the “satisfaction” dimension had the lowest average score (4.048 ± 1.203). The average scores of the items related to the ease of learning and simplicity of the system were higher (5.190 ± 1.167 and 5.143 ± 1.108, respectively) compared with the other items.
TABLE 2 - The Usability of the CDSS (N = 21) Dimensions Items M ± SD M ± SD Usefulness It helps me be more effective. 4.714 ± 0.956 4.530 ± 0.218 It helps me be more productive. 4.667 ± 1.064 It is useful. 4.709 ± 0.873 It gives me more control over the activities in my life. 4.571 ± 1.165 It makes the things I want to accomplish easier to get done. 4.619 ± 1.161 It saves me time when I use it. 4.238 ± 1.179 It meets my needs. 4.381 ± 0.921 It does everything I would expect it to do. 4.238 ± 0.995 Ease of use It is easy to use. 4.952 ± 1.283 4.667 ± 0.263 It is simple to use. 5.143 ± 1.108 It is user-friendly. 4.667 ± 1.064 It requires the fewest steps possible to accomplish what I want to do with it. 4.667 ± 1.316 It is flexible. 4.667 ± 1.064 Using it is effortless. 4.619 ± 0.973 I can use it without written instructions. 4.714 ± 1.230 I don’t notice any inconsistencies as I use it. 4.857 ± 1.153 Both occasional and regular users would like it. 4.381 ± 0.740 I can recover from mistakes quickly and easily. 4.190 ± 0.813 I can use it successfully every time. 4.476 ± 1.030 Ease of learning I learned to use it quickly. 5.048 ± 1.117 5.083 ± 0.081 I easily remember how to use it. 5.095 ± 1.091 It is easy to learn to use it. 5.190 ± 1.167 I quickly became skillful with it. 5.000 ± 0.949 Satisfaction I am satisfied with it. 4.619 ± 0.973 4.422 ± 0.214 I would recommend it to a friend. 4.619 ± 0.921 It is fun to use. 4.048 ± 1.203 It works the way I want it to work. 4.381 ± 1.117 It is wonderful. 4.524 ± 1.167 I feel I need to have it. 4.524 ± 1.209 It is pleasant to use. 4.238 ± 1.044For usability score means, 1 = strongly disagree; 2 = disagree; 3 = somewhat disagree; 4 = neutral; 5 = somewhat agree; 6 = agree; and 7 = strongly agree.
M, mean.
The time required for fall-prevention care is displayed in Supplementary Table 1 (https://links.lww.com/JPS/A566). Overall, the time spent on fall-prevention practices per patient increased after using the CDSS. Furthermore, the high-risk group exhibited the highest increase in the amount of time spent on fall-risk assessments, nursing diagnoses, and planning by fall risk and risk factors upon using the CDSS. Before implementing the CDSS, the high-risk group received nursing interventions such as environmental modifications and patient or caregiver education regarding the risk of falling. By contrast, the time spent documenting fall-prevention interventions, conducting nursing diagnoses, and planning by risk factors increased the most in the low-risk group.
Changes in Frequency of Fall-Prevention InterventionsTable 3 shows the changes in the number of documented nursing statements related to fall-prevention interventions before versus after using the CDSS. Each of the 480 patients included in the post-CDSS observation period experienced fall-prevention care using the CDSS at least once. Upon using the CDSS, the mean frequency of nursing statements related to fall-prevention practices per day increased from 8.519 to 9.435. The number of nonspecific interventions, including environmental modifications, increased, whereas the number of tailored interventions based on risk factors decreased. Significantly more fall-prevention interventions were documented by the nurses for patients with a high risk of falling (before, 10.64/day; after, 10.42/day) compared with patients with a low risk of falling (before, 6.58/day; after, 8.96/day) regardless of CDSS use. However, nurses documented significantly more fall-prevention interventions after using the CDSS in the group with a low risk of falling only.
TABLE 3 - Changes in Frequency of Fall-Prevention Nursing Interventions Pre-CDSS (No. Patients = 1319), M ± SD Post-CDSS (No. Patients = 480), M ± SD t (P) Total number of nursing statements per day 8.519 ± 2.927 9.435 ± 3.169 6.719 (<0.0001) Nonspecific intervention 5.965 ± 2.290 7.294 ± 2.598 12.218 (<0.0001) Tailored intervention 2.550 ± 1.035 2.137 ± 1.043 −8.812 (<0.0001) Lower limb weakness 2.056 ± 0.629 1.713 ± 0.715 −11.471 (<0.0001) Dizziness/vertigo 0.415 ± 0.677 0.316 ± 0.636 −3.312 (<0.001) Altered elimination 0.054 ± 0.281 0.043 ± 0.192 −0.968 (0.333)During the pre-CDSS observation period, the incidence of falls was 3.092 cases per 1000 patient days. By contrast, the incidence of falls was 3.872 cases per 1000 patient days during the 5 months of CDSS use. There were no statistically significant differences (P = 0.451) in the incidence of falls before versus after CDSS use.
DISCUSSIONIn South Korea, periodic assessment of a patient’s fall risk using a verified scientific tool is a main safety requirement for health care or hospital accreditation. Accordingly, the nurses in the study hospital were expected to assess patient fall risk at least twice per week using the Hendrich II Fall Risk Model. Under these circumstances, the use of the new CDSS increased the nurses’ workload and stress related to the workplace information system.16 This was particularly the case for the nurses who were encouraged to use the CDSS along with the Hendrich II Fall Risk Model. Previous studies have indicated that adapting new information systems or technologies to the existing workflow tends to increase stress and dissatisfaction among nurses.17–19 In the current study, nurses were asked to participate in the system requirement analysis, design, and development processes. The goals of this were to ensure that their needs were reflected and to reduce stress or discontent among the end users. However, the usability scores were lower than expected. The nurses might have anticipated that the new system would significantly reduce the amount of time spent on documentation and increase the amount of time available for direct nursing care. The nurses had likely hoped that the contents of nursing intervention provided via the CDSS would be automatically documented in the ENR system to improve work efficiency. However, these functions were not implemented because of budget and time constraints. Consequently, the nurses had to manually document CDSS-provided nursing interventions in the ENR system on top of routine care for fall prevention. The clinical effectiveness of a CDSS is linked to its integration within an EHR such that no additional clinical data entry is required and recommendations are provided as part of the clinical workflow.11,20 Thus, in future studies, the CDSS should be integrated into the EHR system.
Changes in Time Spent on Nursing Care for Fall PreventionThe amount of time spent on nursing diagnoses and planning according to the risk of falls (P = 0.036) and risk factors (P = 0.012) increased in the high-risk patients after implementation of the CDSS. Nurses also spent more time conducting nursing diagnoses and planning by risk factors for low-risk patients (P = 0.014). These findings are consistent with a Duke University Hospital study11 that showed that a CDSS for fall risk identification and fall prevention improved fall risk assessments and fall-prevention plans of care for patients with a high risk of falling. In this study, the CDSS might have helped nurses to better identify and understand each patient’s risk factors for falls, allowing them to spend more time than before on nursing assessments, diagnoses, and planning for each risk factor. However, no significant time differences were found for nonspecific or tailored nursing interventions before versus after CDSS usage.
Changes in Frequency of Fall-Prevention Nursing InterventionsWe analyzed the impact of the CDSS on fall-prevention nursing practices using nursing documentation according to a previous study21 that used nursing documentation to measure the effect of a CDSS on evidence-based nursing practice in oncology nurses. The mean frequency of nursing statements related to fall-prevention practices per day increased from 8.519 to 9.435 upon using the CDSS. In detail, nursing statements related to nonspecific interventions such as environmental modification increased (from 5.965 ± 2.290 to 7.294 ± 2.598), whereas those related to tailored interventions according to risk factors significantly decreased (from 2.550 ± 1.035 to 2.137 ± 1.043). Moreover, nurses documented significantly more fall-prevention interventions for patients with a low risk of falling after CDSS implementation (from 6.578 ± 1.927 to 8.957 ± 3.131). The CDSS might have helped nurses to provide more nonspecific interventions to low-risk patients who were typically overlooked in terms of fall prevention. These findings are not consistent with our expectation that the number of nursing statements related to tailored interventions would increase, particularly in the high-risk group. Because nurses’ decision making is influenced by multiple factors such as clinical experience, judgment or autonomy, personal belief or values, and organizational context,7,22,23 the level of nurses’ adherence to the recommendation provided by the CDSS may not have met our expectations.
Nurses in the study hospital tended to document fewer nursing assessments, diagnoses, and planning for fall prevention compared with documentation of nursing interventions. This was likely because of a lack of standardized nursing statements representing nursing assessments, diagnoses, and planning. Thus, it was difficult to evaluate changes in the records related to nursing assessments, diagnoses, and planning for fall prevention before versus after implementation of the CDSS according to the findings of the survey. To examine the relationship between the time spent on nursing care for fall prevention and the number of records for fall-prevention nursing care, it is necessary to create standardized nursing statements representing nursing assessments, diagnoses, and planning for fall prevention.
Number of FallsWe found that fall-related accidents did not decrease after implementation of the CDSS. These results are consistent with Lytle et al,11 who developed the CDSS to remind nurses to complete fall risk assessments and documentation. Previous studies24,25 that have evaluated the impact of EHR implementation on nurse-sensitive patient outcomes such as falls and pressure ulcers have also reported that the use of a new system is not associated with a reduction of adverse events. It was also consistent with findings of systematic reviews on effectiveness of the CDSS that reported more improvement in practitioner performance than in patient outcome.4,26 However, the fall TIPS DSS considerably reduced the rate of falls and fall-related injuries.8,9 There are a number of factors that may have contributed to the success of the fall TIPS DSS. For instance, the tool was used for a sufficient period (i.e., 21 months), and the researchers ensured the participation of patients, caregivers, and family members in the program. Previous studies have reported that nurses require from approximately 12 months to more than 2 years to fully adapt to a new information system.27,28 Therefore, analyses of nurses’ experience 1 year after implementation of a nursing information system could lead to enhanced system development and adoption.29
LimitationsThis study had several limitations. First, our results lack generalizability because the impact of the CDSS was tested in a single unit of one hospital. Second, the short period of CDSS application may have influenced our ability to study its effectiveness. Third, the CDSS could not be fully integrated into the HIS, including the ENR system. Consequently, nurses had to manually document their activities associated with the CDSS using nursing statements. This might have led to underdocumentation of nursing interventions. Fourth, it was not possible to examine the relationship between the time spent on nursing care for fall prevention and the number of records on fall-prevention nursing care (with the exception of nursing interventions) because of a lack of standardized nursing statements representing nursing assessments, diagnoses, and planning. Fifth, some of the nurses participated in both the control and study groups, violating the requirements of an independent 2-group experimental design.
CONCLUSIONSData regarding the impact of CDSSs on fall prevention have been inconsistent. The CDSS usability scores after 1 month of use were 4.530, 4.667, 5.083, and 4.422 for the 4 dimensions of usefulness, ease of use, ease of learning, and satisfaction, respectively. Regarding the amount of time spent on nursing care for fall prevention, the time spent conducting nursing diagnoses and planning by risk factors increased significantly after using the CDSS. In addition, the mean frequency of nursing statements related to fall-prevention practices per day increased upon using the CDSS, particularly in the low-risk group. However, we observed no improvement in clinical outcomes, such as a reduction in fall rate. Future work is needed to examine CDSSs that have been fully integrated into HISs and to evaluate the effectiveness of such systems for sufficient periods of time in multiple inpatient wards. As a method for evaluating the effectiveness of CDSSs, we recommend a time-motion study, in which changes in nursing practices are directly measured according to time and type.
REFERENCES 1. Jung H, Park HA. Testing the predictive validity of the Hendrich II Fall Risk Model. West J Nurs Res. 2018;40:1785–1799. 2. Jung H, Park HA, Hwang H. Improving prediction of fall risk using electronic health record data with various types and sources at multiple times. Comput Inform Nurs. 2020;38:157–164. 3. Sim I, Gorman P, Greenes RA, et al. Clinical decision support systems for the practice of evidence-based medicine. J Am Med Inform Assoc. 2001;8:527–534. 4. Jaspers MW, Smeulers M, Vermeulen H, et al. Effects of clinical decision-support systems on practitioner performance and patient outcomes: a synthesis of high-quality systematic review findings. J Am Med Inform Assoc. 2011;18:327–334. 5. Kruse CS, Ehrbar N. Effects of computerized decision support systems on practitioner performance and patient outcomes: systematic review. JMIR Med Inform. 2020;8:e17283. 6. Randell R, Mitchell N, Dowding D, et al. Effects of computerized decision support systems on nursing performance and patient outcomes: a systematic review. J Health Serv Res Policy. 2007;12:242–249. 7. Akbar S, Lyell D, Magrabi F. Automation in nursing decision support systems: a systematic review of effects on decision making, care delivery, and patient outcomes. J Am Med Inform Assoc. 2021;28:2502–2513. 8. Dykes PC, Carroll DL, Hurley A, et al. Fall prevention in acute care hospitals: a randomized trial. JAMA. 2010;304:1912–1918. 9. Dykes PC, Burns Z, Adelman J, et al. Evaluation of a patient-centered fall-prevention tool kit to reduce falls and injuries: a nonrandomized controlled trial. JAMA Netw Open. 2020;3:e2025889. 10. Dykes PC, Hurley AC. Patient-centered fall prevention. Nurs Manage. 2021;52:51–54. 11. Lytle KS, Short NM, Richesson RL, et al. Clinical decision support for nurses: a fall risk and prevention example. Comput Inform Nurs. 2015;33:530–537; quiz E1. 12. Jung H, Park HA. Development and evaluation of a prototype CDSS for fall prevention. Stud Health Technol Inform. 2019;264:1700–1701. 13. Lund AM. Measuring usability with the use questionnaire12. Usability Interface. 2001;8:3–6. 14. Jung H, Park HA, Lee HY. Comparisons of fall prevention activities using electronic nursing records: a case-control study. J Patient Saf. 2022;18:145–151. 15. Jung H, Yoo S, Kim S, et al. Patient-level fall risk prediction using the observational medical outcomes partnership’s common data model: pilot feasibility study. JMIR Med Inform. 2022;10:e35104. 16. Heponiemi T, Hyppönen H, Vehko T, et al. Finnish physicians’ stress related to information systems keeps increasing: a longitudinal three-wave survey study. BMC Med Inform Decis Mak. 2017;17:147. 17. Kaihlanen AM, Gluschkoff K, Laukka E, et al. The information system stress, informatics competence and well-being of newly graduated and experienced nurses: a cross-sectional study. BMC Health Serv Res. 2021;21:1096. 18. Bristol AA, Nibbelink CW, Gephart SM, et al. Nurses’ use of positive deviance when encountering electronic health records–related unintended consequences. Nurs Adm Q. 2018;42:E1–e11. 19. Chang CP, Lee TT, Liu CH, et al. Nurses’ experiences of an initial and reimplemented electronic health record use. Comput Inform Nurs. 2016;34:183–190. 20. Lobach D, Sanders GD, Bright TJ, et al. Enabling health care decisionmaking through clinical decision support and knowledge management. Evid Rep Technol Assess (Full Rep). 2012;203:1–784. 21. Cortez S, Dietrich MS, Wells N. Measuring clinical decision support influence on evidence-based nursing practice. Oncol Nurs Forum. 2016;43:E170–E177. 22. Nibbelink CW, Brewer BB. Decision-making in nursing practice: an integrative literature review. J Clin Nurs. 2018;27(5–6):917–928. 23. Gerdtz MF, Bucknall TK. Triage nurses’ clinical decision making. An observational study of urgency assessment. J Adv Nurs. 2001;35:550–561. 24. Furukawa MF, Raghu TS, Shao BBM. Electronic medical records, nurse staffing, and nurse-sensitive patient outcomes: evidence from the national database of nursing quality indicators. Med Care Res Rev. 2011;68:311–331. 25. Dowding DW, Turley M, Garrido T. The impact of an electronic health record on nurse sensitive patient outcomes: an interrupted time series analysis. J Am Med Inform Assoc. 2012;19:615–620. 26. Garg AX, Adhikari NK, McDonald H, et al. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA. 2005;293:1223–1238. 27. Carayon P, Cartmill R, Blosky MA, et al. ICU nurses’ acceptance of electronic health records. J Am Med Inform Assoc. 2011;18:812–819. 28. Terry AL, Brown JB, Bestard Denomme L, et al. Perspectives on electronic medical record implementation after two years of use in primary health care practice. J Am Board Fam Med. 2012;25:522–527. 29. Lee TT. Nurses’ experiences using a nursing information system: early stage of technology implementation. Comput Inform Nurs. 2007;25:294–300.
Comments (0)