
記住我
When medical oncologists consider the risks that patients face, they generally focus on adverse drug events. Clinical trial publications universally include a table describing and quantifying adverse drug events using a standardized grading system, Common Terminology Criteria for Adverse Events.1 In addition, adverse drug events are collected following Food and Drug Administration approval of new agents, in the course of providing routine care as patient-reported data, and in the context of pragmatic clinical trials.2–5 At the same time, we, and our patients, know little about the risks experienced during the course of receiving routine cancer care. However, a panoply of potential risks to patient safety exists including those due to deviations from evidence-based care, to medical errors, to delays, to poorly organized and coordinated care, to unnecessary exposures, and to inequities in care; these are the risks that can result in unnecessary suffering due not to cancer or its treatment, but from system failures.6
Research efforts to characterize and quantify the risks to patient safety experienced by medical oncology patients have relied largely on retrospective review of medical records, surveys of patients and staff, and review of large databases. The focus has been on characterizing errors in ordering, preparing, administering, and monitoring parenteral and oral chemotherapy. Independent of the methodology, each has demonstrated ongoing risks to patient safety ranging from 1 to 4 errors per 1000 orders, affecting 1% to 3% of patients.7–12
In the routine care setting, healthcare systems use a variety of approaches to assess patient safety including voluntary incident reporting systems, trigger tools, patient complaint and grievance registries, review of malpractice claims and risk management files, executive patient safety walk rounds, and patient experience surveys and interviews.13 In principle, the collection and systematic analysis of incident reports should allow patient safety experts to design and implement solutions to improve patient safety: reports are submitted by frontline workers who are in the best position to identify safety issues and staff are encouraged to report not only serious events, but also episodes of minor harm, near misses, and potential hazards. However, for the most part, incident reporting systems have not lived up to expectations.14–16 There are a few reasons why they have failed to improve care. For example, many healthcare facilities focus on the quantity of reports rather than on receiving high-quality actionable ones. Others fail to reach out to those who took the time to submit a report, reducing their confidence in the program. A recent critical review of incident reporting systems pointed out another flaw—the lack of standard definitions of incidents and the lack of validated taxonomies.15 The authors noted that “when definitions were clear, such as in studies of blood transfusions and macro-level drug reporting, IRSs [incident reporting systems] were more likely to improve safety.”
In 2020, we developed and validated a medical oncology–specific incident reporting taxonomy with the hope that the specificity inherent in a specialty-focused system would translate into opportunities to improve the safety of patients receiving systemic treatment for cancer.17 In the current study, we applied the new taxonomy to characterize several hundred randomly selected incident reports from 3 different cancer centers. The purpose of the analysis was to (1) test its ability to be used in different settings, (2) characterize and quantify patterns of incidents, and (3) identify specific safety risks that could result in future harm for patients receiving anticancer therapy.
METHODSThe project was deemed exempt from institutional review board review because it did not meet the criteria for research involving human subjects as defined by the Department of Health and Human Services and Federal Drug Administration regulations.
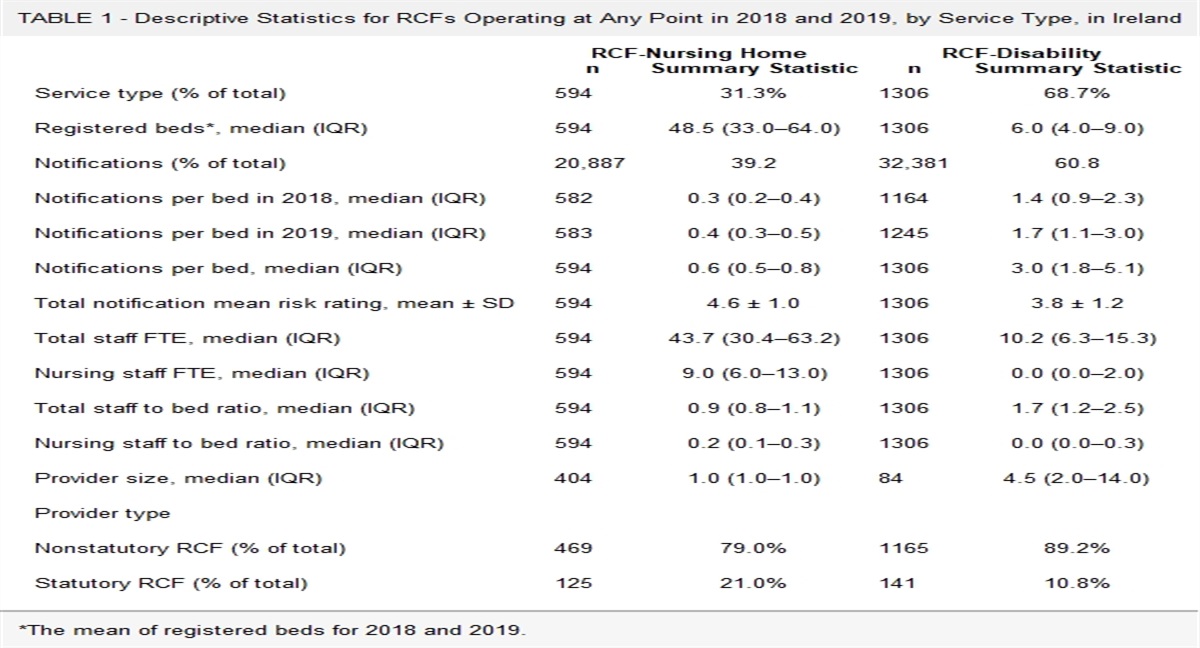
The key component of the project was to assess the ability of the taxonomy to be applied to routinely collected voluntary patient safety reports across 3 distinct sites following standard criteria.17,18 We randomly selected 309 deidentified incident reports from the same 3 cancer centers initially involved in the validation (Supplemental file A, https://links.lww.com/JPS/A567). Using a structured process, coders were instructed to read each incident carefully, searching for key words or phrases that best explained why the incident reporter placed the entry, and to search the incident and contributing factor code sheets to identify the best fit for each. Each report was coded for primary and, where possible, secondary incident types and for up to 2 contributing factors. Coders were instructed to concentrate only on the incident as described and not to draw inferences or bring specialized knowledge to bear. Coders understood that the primary focus of the project was on incident categorization; contributing factors collection was for exploratory purposes only. The incident taxonomy is summarized in Table 1. The full taxonomy is reproduced in Supplemental file B, https://links.lww.com/JPS/A568. Contributing factors categories are included in Supplemental file C, https://links.lww.com/JPS/A569.
TABLE 1 - Incident Taxonomy Level 1 (3 Categories) Level 2 (4 Categories) Level 3 (26 Categories, Examples) Level 4 (44 Categories, Examples) Clinical Safety Drug prescription Change in order not communicated Wrong drug ordered Contraindication to ordered drug Pharmacy preparation Labeling problem Delays Medication administration Drug activation before clinical assessment IV catheter management Adverse drug reactions Potentially avoidable Procedure Procedure Quality/knowledge/skills Evaluation and assessment Inadequate history taking Therapeutic decisions Failure to arrange appropriate, timely, short-term, or long-term follow-up care Relational Relational Care coordination Care coordination among 3 or more parties Institutional/management Institutional/management Protocols and guidelines Failure to adhere to published guidelinesThree of the authors (J.J., T.M., J.Z.) participated in the coding exercise. Each incident report was reviewed separately by 2 coders in batches of 25. Within 1 week of completing a batch, the 2 coders met to review the assignments. Those reports for which the coders agreed on the incident category were deemed “primary agreement.” The coders then attempted to reach consensus on the remaining reports and, where an agreement was reached, deemed “secondary agreement.” The remainder was submitted to group review (J.J., T.M., J.Z., A.R., and S.S.) for which “tertiary agreement” was reached if 3 or more reviewers agreed on an incident category. Contributing factors were not adjudicated but rather were combined for descriptive analysis.
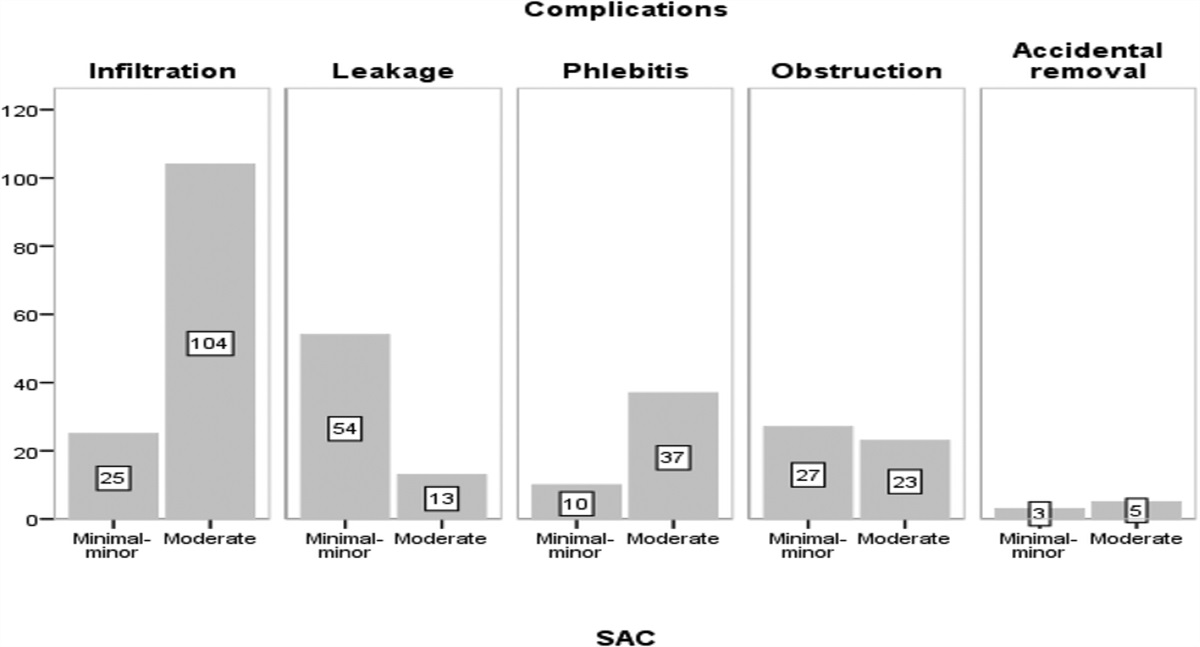
During the process of cataloguing incident types, the authors recognized several hazards that posed the potential for future harm to medical oncology patients. This led to a secondary analysis to clarify and quantitate a set of care scenarios related to those hazards that could place patients at risk for major or catastrophic harm, either immediate or delayed. One of the authors (J.J.) reviewed all events, either separately or with a second author (J.D.). A draft list of scenarios was then reviewed with the other clinical authors (J.Z., T.M). during a structured session overseen by a qualitative researcher (A.R.) and epidemiologist (S.S.). This 3-step group consensus process was used to create a final list of scenarios. Then, each scenario was assessed using the Safety Assessment Code (SAC) matrix, which characterizes incidents based on 2 criteria: severity assessment (catastrophic, major, moderate, minor) and probability of occurrence of the worst possible outcome (frequent, occasional, uncommon, remote).19 High- and intermediate-risk scenarios were included in the final list.
Additional data available with the incident reports from the individual institutions included severity of harm and reporter’s role. The analysis was limited because the scoring approach and the classification system varied among the institutions. For example, only one institution included a category for unsafe conditions. While all institutions included categories for near-miss, minor harm, major harm, and death, the terminology varied. Reports were also characterized by reporter type, which, based on the available data for this analysis, was limited to 2 categories: physicians compared with “all others.”
Descriptive statistics and other analyses were calculated using Excel (Microsoft Corporation One Microsoft Way Redmond, WA).
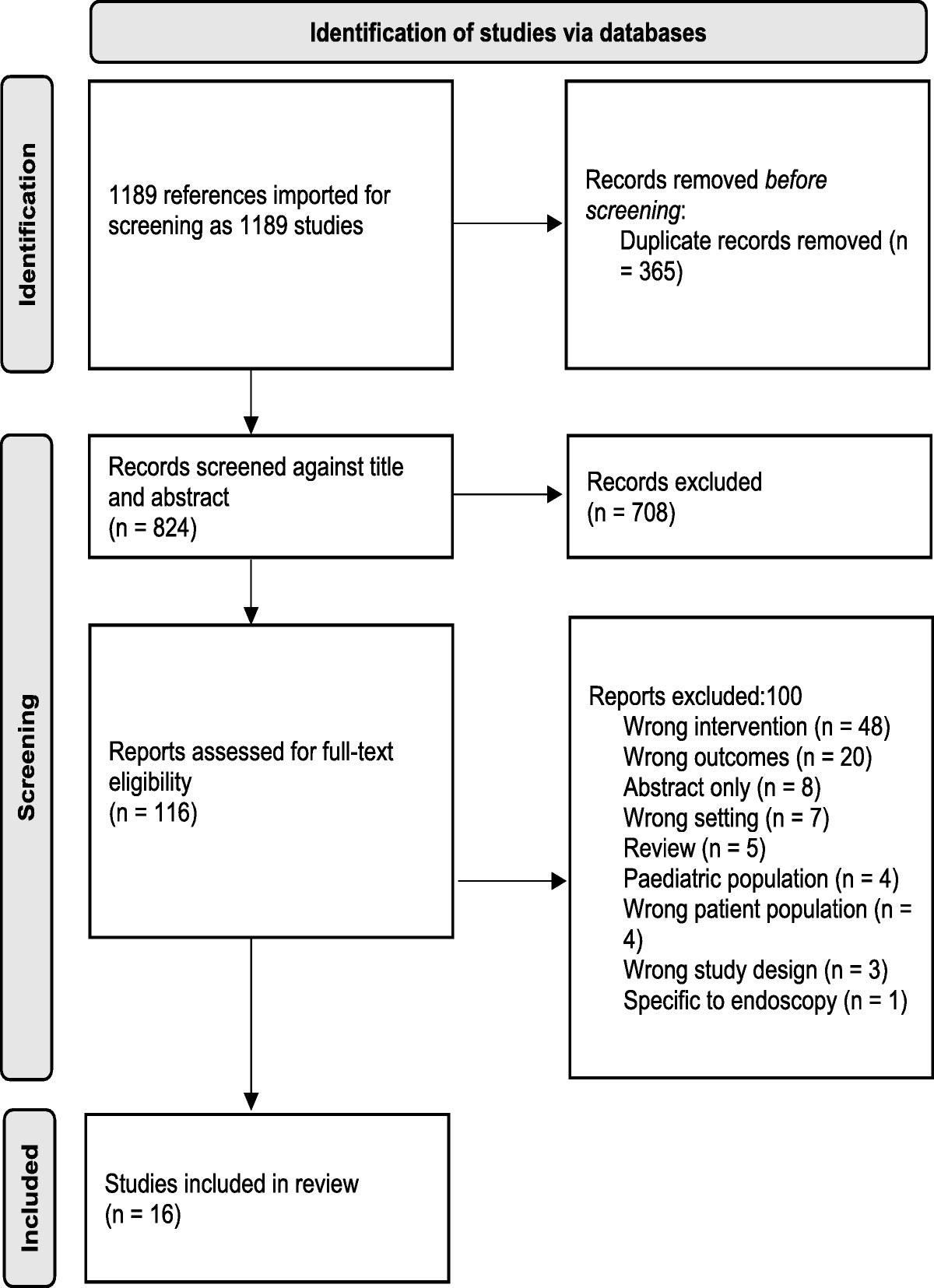
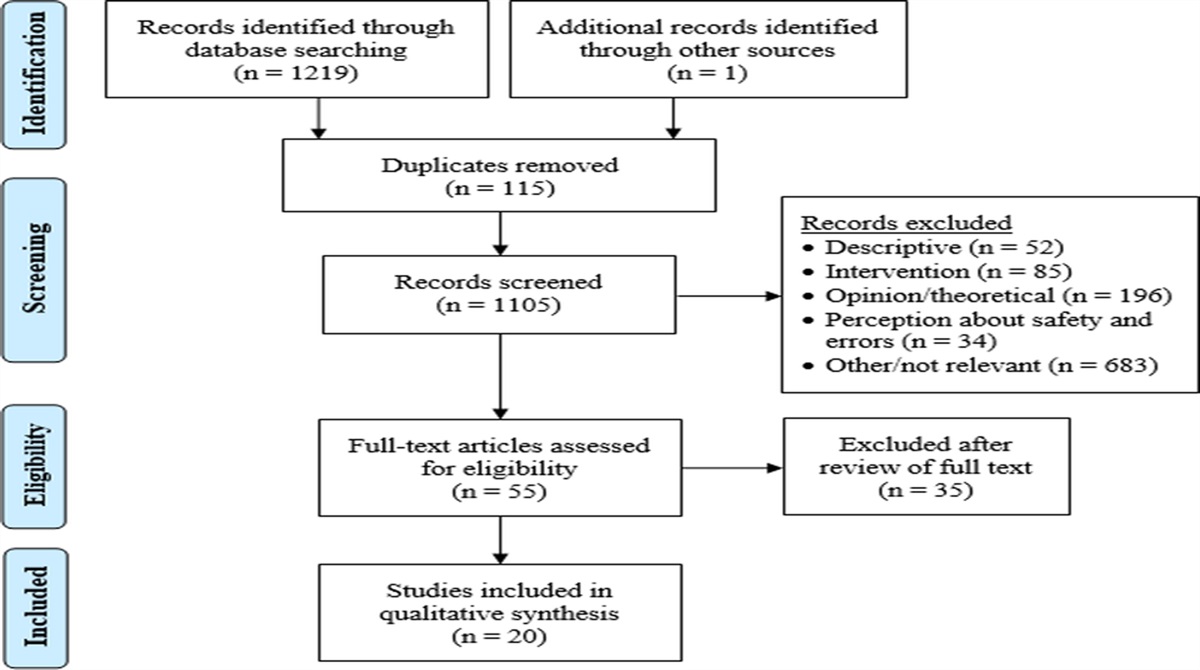
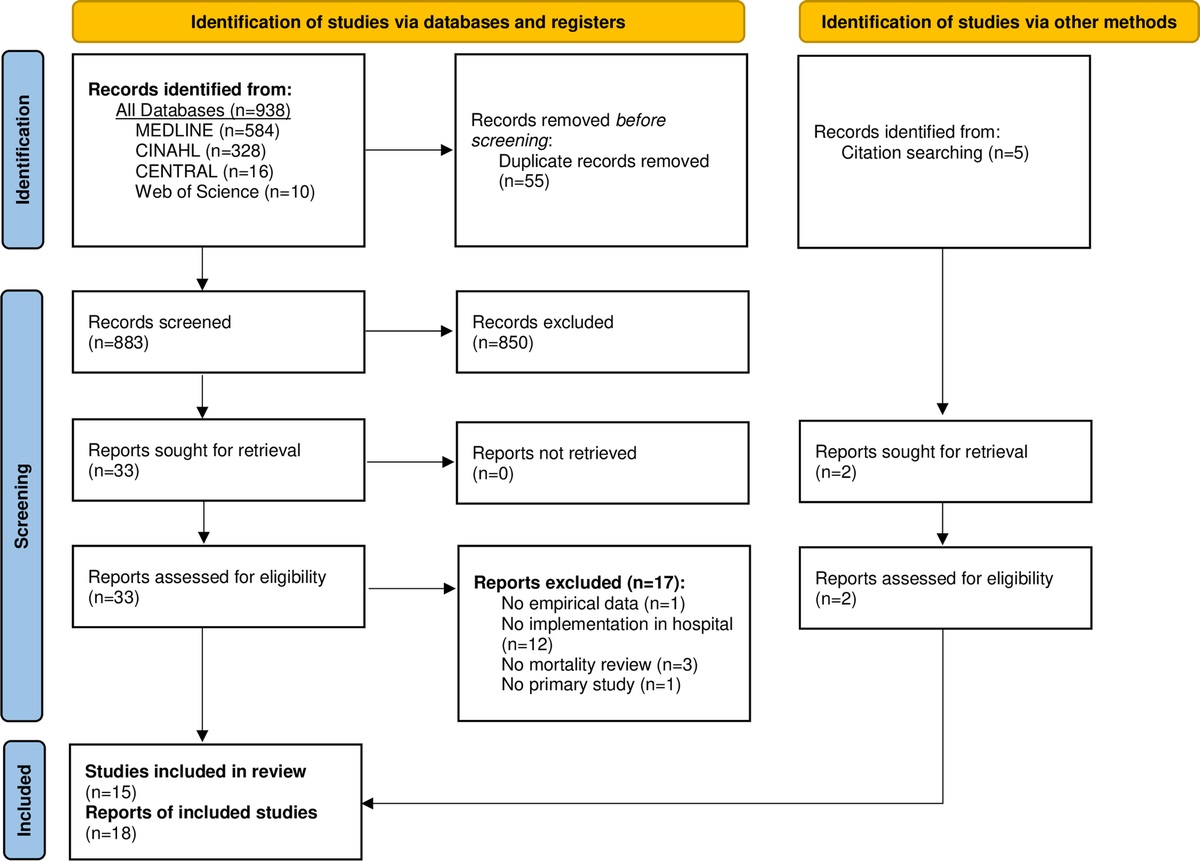
RESULTS Incident CategorizationOf 309 incident reports, 2 were excluded. One was a duplicate report. The second was a mischaracterized radiation oncology incident. For the remaining reports, 2 coders reached primary agreement on 69% on first review. Of the 98 reports that remained, the 2 coders reached secondary agreement for an additional 82. The remaining 16 reports were submitted to group review; majority agreement was reached in 13; 3 were excluded because of insufficient narrative. Overall, 300 reports were assigned to a specific incident category, a 98.7% success rate; 4 were characterized as “incident other” (Fig. 1).
 FIGURE 1:
FIGURE 1: Process for assignment of an incident category for 309 randomly selected incident reports from 3 cancer programs.
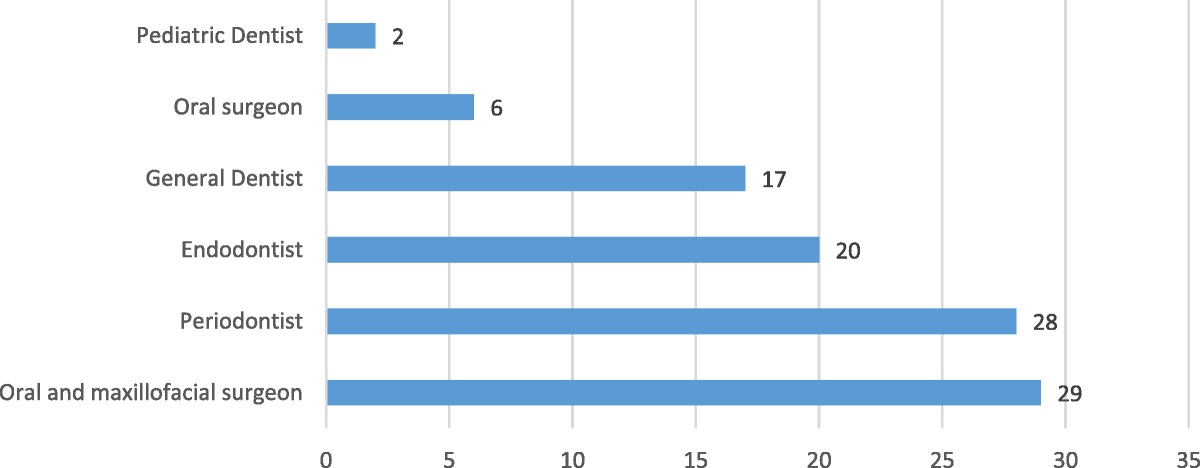
A second incident category could be assigned for 32 reports, which were combined with primary incidents for further analysis (Fig. 2, n = 336). Incident types were rolled up to 21 categories for ease of interpretation (all categories were selected at least once except for “anesthesia, sedation complication”) and were stratified by institution. Incidents related to prescriber ordering accounted for the largest number of reports (75), followed by nursing care–related (50), relational issues (49), and pharmacy-related issues (48) (Fig. 2, Table 2). The proportions attributed to each site varied substantially.
 FIGURE 2:
FIGURE 2: Incident categories arranged in descending order of frequency and stratified by site (n = 304). For ease of interpretation, relational categories 15 to 17 (documentation of care, communication, coordination of care and other relational issues) were combined (“relational”). Similarly, categories 11 to 13 (evaluation and assessment, therapeutic decision making and evaluation or therapeutic decision making, other) were combined under “clinical evaluation.”
TABLE 2 - Most Common High-Level Incident Categories (n = 222) Incident Categories and Subcategories No. Incidents by Category/Subcategory Prescriber related 75 Wrong order 36 Delay 12 Dose adjustment not ordered 7 Dose order change not communicated 6 Contraindicated medication ordered 2 Prescriber ordering, other 12 Nursing care related 50 Administration error 20 IV management error 8 Activation before assessment 8 Delays 2 Order activation issue 1 Administration other 1 Height or weight issue 1 Failure to reconcile labs 1 Nursing care, other 8 Relational 49 Overall care coordination 26 Communication (usually limited to 2 parties) 13 Documentation errors 9 Relational, other 1 Pharmacy related 48 Delay 19 Preparation error 19 Mixing incompatible or contraindicated medications 2 Pharmacy, other 8Among the 36 “wrong order” incidents, 28 were related to chemotherapy prescribing. Nine involved patients enrolled in clinical trials. Four involved the prescription of an oral antineoplastic agent, each of which occurred in the setting of a clinical trial. Of the 20 medication administration incidents, 13 involved chemotherapy, 2 involved a clinical trial, and 1 related to an oral antineoplastic agent. Five reports described patients receiving an infusion at the wrong rate; in at least 3 cases, incorrect programming of an infusion pump was deemed to be causal (Table 2).
Incident SeverityThe findings, stratified by institution, are depicted in Supplementary File D, https://links.lww.com/JPS/A570. Ninety-two percent of reports either described a near miss or a completed event without injury; 7.9% of incidents were associated with minor, transient harm; and 2 events resulted in severe harm, including one patient death.
Two high-severity incidents were identified in the cohort. One entailed a patient who developed irreversible congestive cardiomyopathy after receiving multiple cycles of doxorubicin. The total dose administered was within acceptable limits, but serial cardiac imaging had not been performed following a normal pretreatment study. The second high-severity incident described a delay in administering the correct antibiotic for a critically ill patient with sepsis from a rare bacterial species.
High-Risk ScenariosIn a secondary analysis, 11 scenarios were identified that posed safety risks. Nine scenarios were scored as high or intermediate risk based on the SAC matrix and were included in the final list.
High-risk scenarios are detailed in Table 3 with an example provided for each. They are grouped into six broad categories. The first, health information technology, includes 3 different scenarios. “Carry-forward” errors may be a risk unique to patients receiving systemic anticancer therapies. For chemotherapy regimen cycles that contain more than 1 day of treatment, dose changes made during a cycle may not be included in additional cycles, increasing the risk of future toxicity. This error occurred at all 3 cancer centers including 2 that share a proprietary electronic health record with a chemotherapy order entry system, and one that uses an in-house–developed electronic health record with chemotherapy order entry. While some systems provide pop-up warnings for providers to prevent the error, these are easily overridden. Other provider order entry designs include defaults to the previously changed dose, with an option to change to the initial dose, which may or may not be acted upon. Carry-forward errors accounted for at least 5 incident reports. Other health information technology–related incidents—treatment and appointment scheduling—were at least partly enabled by technology, which requires providers to enter separate requests for both the order and the scheduling of the order. Programmable pump errors were described in at least 5 incidents. Environment of medical oncology care and growing complexity of care accounted for additional broad groupings. These risks were attributed to the frequent lack of co-location of care for providers, pharmacists, and nurses responsible for medical oncology care risking failures in communication. The remaining 2 groupings, administrative tasks and knowledge management, are not unique to medical oncology but pose potential risk of serious incidents.
TABLE 3 - Intermediate- and High-Risk Scenarios High-Risk Scenario Description/Example SAC Matrix Risk Score19 1 Health information technology “Carry forward” chemotherapy orders For chemotherapy regimen cycles that include more than one day of treatment, dose changes made during the cycle may not be included in future cycles if (1) the provider has already created future cycles or (2) the provider copies the cycle forward. System prompts to adjust the dose are easily overlooked.Contributing factors were collected as part of an exploratory analysis. A total of 478 contributing factors was identified by at least one reviewer. This number exceeds the total number of incident reports because contributing factors were not adjudicated. A contributing factor was identified for 83% of reports. Supplemental file E (https://links.lww.com/JPS/A571) provides a high-level summary of the findings. Issues related to individual performance accounted for 50% of contributing factors (n = 239), principally mistakes (errors of omission, commission, or misaction), inadequate communication by an individual, failure to follow an existing procedure, policy or guideline not followed, or followed incorrectly or incompletely. Issues related to IT functionality, teamwork, resource availability or quality, and policy or protocol accounted for the remainder.
DISCUSSION Primary AnalysisWe tested the ability of a recently validated medical oncology incident taxonomy to evaluate a large random sample of incident reports from across 3 diverse cancer centers. We confirmed the usefulness of the taxonomy, which was able to classify 98.7% of incidents. Sixty-seven percent of incidents were encompassed by the following 4 categories: prescriber ordering (22%), nursing care (15%), pharmacy (14%), and relational issues (15%, including communication, coordination, and documentation). Incidents were successfully classified regardless of the category of the reporter, which varied across each health system.
We identified unexpected variation in reporting patterns across the 3 sites (Fig. 2). For example, site 2 accounted for 57% of total pharmacy reports but only 15% of nursing-related reports. On the other hand, site 3 accounted for 29% of total pharmacy reports and 42% of nursing-related reports. Two explanations may account for the variation. One is that the rates reflect actual differences in the patterns of safety and quality experienced by the patients and staff at the different sites. Another possibility—one that we favor—is that the different patterns reflect cultural and operational variation across the 3 sites. For example, at one site, staff in one high-reporting department receive annual feedback on the number of incident reports that they submit (Supplemental file A, https://links.lww.com/JPS/A567).
The report content also differed by site. While most reports describe either interrupted errors or errors that reached the patient without causing demonstrable harm, 2 reports (0.7%) described major harm. The rate of incidents reaching the patient varied across the 3 sites from 2% at site 2 to 17% at site 3 (where both major harm incidents were reported). The proportion of incident reports submitted by physicians varied by nearly 10-fold across the 3 sites (10.7%, 1.7%, 16.1%, for sites 1, 2, and 3, respectively).
The striking variation across the 3 sites for reporting events reaching the patient and the proportion of physician reports raise the possibility of differences in safety culture. Several investigations have shown a correlation between the measured strength of an institutional safety culture and the likelihood of voluntary clinician reporting. Willingness to report may also benefit from ongoing training efforts that stress the importance of reporting and from the likelihood that the reporter receives feedback.20–23
Secondary AnalysisWe undertook a qualitative analysis to identify scenarios that pose the potential for causing major harm to medical oncology patients. Nine scenarios met the criteria for inclusion (risk score of high or intermediate) including 6 with the potential for a catastrophic outcome. On the surface, each of the scenarios seems to be related to human error, and in fact, frontline staff are almost always at the “sharp end of the stick”6; they are the proximate cause of the incident and often are blamed. However, each of the scenarios is at least partly the consequence of “enabling” upstream decisions that set the stage for the incident.24 Using the taxonomy to classify the incidents, the foundational issues could be identified.
The first step in any quality improvement initiative is to define the problem. The next step is to develop solutions. One potential path to improvement is through human factors engineering (HFE). From an HFE standpoint, staff are at the mercy of poorly designed systems that, if managed better, could greatly reduce the risk of future incidents. Human factors engineering–focused solutions can be described for each of the nine scenarios. For example, redesign of man-machine interfaces has the potential to reduce the risk for the first 4 scenarios—computerized order entry and programmable pumps.25–32 Recognition of the complexity of medical oncology care could lead to the development of checklists and other tools to reduce risk, especially in the setting of highly complicated clinical trials where several concerning incidents were identified.33 In some high-risk industries, cross-checking has been shown to have limited value, yet in medical oncology, we rely heavily on double checks for chemotherapy preparation and administration.34 Even errors related to deviations from evidence- and consensus-based recommendations could benefit from HFE. Tools such as treatment pathways, if properly integrated into workflow, improve adherence.35
Contributing Factors AnalysisAs part of an exploratory analysis, we collected data on potential contributing factors. Reviewer confidence in assigning at least one contributing factor was substantially lower than for assigning an incident category; fully one-third of incident reports lacked sufficient clarity for at least one of the reviewers to assign a contributing factor (data not shown). Improving details collected by incident reporting systems to characterize contributing factors may identify future improvement projects and help move improvements upstream of harm.20
LimitationsIt is important to point out the limitations of this study. The narrative reports were voluntarily submitted by reporters who were asked to provide a brief description of the incident or risky setting and usually without knowledge of the factors that contributed to it. Some narratives were rich with detail, while others included a single bullet of information. Nonetheless, we were able to assign an incident category for nearly all reports with a satisfactory degree of certainty. Another limitation of the study is that of generalizability. Although we included incident reports from 3 different cancer centers (which, in totality, included ambulatory and inpatient care, academic medical center and community sites, and pediatric and adult patients), and we used a rigorous analytic approach including triangulating across researchers from the 3 sites, the sample size is relatively small. Future work should build on these data before they can be considered to reflect medical oncology care more broadly.
ConclusionsWe have tested a recently validated medical oncology–specific incident reporting taxonomy at 3 cancer centers. The taxonomy was able to be applied to routinely collected voluntary patient safety reports; 98.7% of incidents could be assigned a specific incident category. Secondary analysis identified 9 scenarios that place patients at risk for major or catastrophic consequences, each of which may benefit from an HFE-based improvement plan. We believe that the taxonomy is ready for further testing and that if implemented broadly (akin to such programs as the Radiation Oncology Incident Learning System) could be used to identify and ameliorate lurking safety risks facing our patients.36
ACKNOWLEDGMENTThe authors thank Expert Advisory Panel, which included Sharon Lane, RN, CPPS; Jennifer Mack, MD, MS; Lawrence Wong, PhD; Jessica McGuire, RN; Lisa Fitzgerald, MHA; Dana Platt, MSHCA, RN, CPHRM; and Brendan Sendrowski, RPH.
REFERENCES 1. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. Available at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf. Accessed July 11, 2022. 2. Mosley SA, Hicks JK, Portman DG, et al. Design and rational for the precision medicine guided treatment for cancer pain pragmatic clinical trial. Contemp Clin Trials. 2018;68:7–13. 3. Basch E, Reeve BB, Mitchell SA, et al. Development of the National Cancer Institute's patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst. 2014;106:dju244. 4. Postmarketing adverse event reporting compliance program. Available at: https://www.fda.gov/drugs/surveillance/postmarketing-adverse-event-reporting-compliance-program. Accessed July 11, 2022. 5. Khozin S, Blumenthal GM, Pazdur R. Real-world data for clinical evidence generation in oncology. JNCI. 2017;109. doi: 10.1093/jnci/djx187. 6. Jacobson JO. Suffering, systems, and safety: applying the principles of systems safety to improve the care of patients with cancer. JCO Oncol Pract. 2020;16:115–120. 7. Gandhi TK, Bartel SB, Shulman LN, et al. Medication safety in the ambulatory chemotherapy setting. Cancer. 2005;104:2477–2483. 8. Ford CD, Killebrew J, Fugitt P, et al. Study of medication errors on a community hospital oncology ward. J Oncol Pract. 2006;2:149–154. 9. Schulmeister L. Chemotherapy medication errors: descriptions, severity, and contributing factors. Oncol Nurs Forum. 1999;26:1033–1042. 10. Ranchon F, Salles G, Spath HM, et al. Chemotherapeutic errors in hospitalised cancer patients: attributable damage and extra costs. BMC Cancer. 2011;11:478. 11. Weingart SN, Price J, Duncombe D, et al. Patient-reported safety and quality of care in outpatient oncology. Jt Comm J Qual Patient Saf. 2007;33:83–94. 12. Weingart SN, Zhang L, Sweeney M, et al. Chemotherapy medication errors. Lancet Oncol. 2018;19:e191–e199. 13. Levtzion-Korach O, Frankel A, Alcalai H, et al. Integrating incident data from five reporting systems to assess patient safety: making sense of the elephant. Jt Comm J Qual Patient Saf. 2010;36:402–410. 14. Macrae C. The problem with incident reporting. BMJ Qual Saf. 2016;25:71–75. 15. Stavropoulou C, Doherty C, Tosey P. How effective are incident-reporting systems for improving patient safety? A systematic literature review. Milbank Q. 2015;93:826–866. 16. Shojania KG. The frustrating case of incident-reporting systems. Qual Saf Health Care. 2008;17:400–402. 17. Jacobson JO, Zerillo J, Mulvey TM, et al. Development of a taxonomy for characterizing medical oncology–related patient safety and quality incidents: a novel approach. BMJ Open Quality. 2022;11:e001828. 18. Arain M, Campbell MJ, Cooper CL, et al. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med Res Methodol. 2010;10:67. 19. Bagian JP. RCA2: Improving Root Cause Analyses and Actions to Prevent Harm. National Patient Safety Foundation: Boston MA; 2015. 20. Braithwaite J, Westbrook MT, Travaglia JF, et al. Cultural and associated enablers of, and barriers to, adverse incident reporting. Qual Saf Health Care. 2010;19:229–233. 21. Hutchinson A, Young TA, Cooper KL, et al. Trends in healthcare incident reporting and relationship to safety and quality data in acute hospitals: results from the National Reporting and Learning System. Qual Saf Health Care. 2009;18:5–10. 22. Mahajan RP. Critical incident reporting and learning. Br J Anaesth. 2010;105:69–75. 23. Tricarico P, Castriotta L, Battistella C, et al. Professional attitudes toward incident reporting: can we measure and compare improvements in patient safety culture? International J Qual Health Care. 2017;29:243–249. 24. Reason JT, Carthey J, de Leval MR. Diagnosing “vulnerable system syndrome”: an essential prerequisite to effective risk management. Qual Health Care. 2001;10(suppl 2):ii21–ii25. 25. Asan O, Carayon P. Human factors of health information technology—challenges and opportunities. Int J Hum Comput Interact. 2017;33:255–257. 26. Carayon P, Hoonakker P. Human factors and usability for health information technology: old and new challenges. Yearb Med Inform. 2019;28:71–77. 27. Cresswell KM, Blandford A, Sheikh A. Drawing on human factors engineering to evaluate the effectiveness of health information technology. J R Soc Med. 2017;110:309–315. 28. Gibbons MC, Lowry SZ, Patterson ES. Applying human factors principles to mitigate usability issues related to embedded assumptions in health information technology design. JMIR Hum Factors. 2014;1:e3. 29. Patterson ES. Workarounds to intended use of health information technology: a narrative review of the human factors engineering literature. Hum Factors. 2018;60:281–292. 30. Waterson P, Hoonakker PL, Carayon P. Special issue on human factors and the implementation of health information technology (HIT): comparing approaches across nations. Int J Med Inform. 2013;82:277–280. 31. Zayas-Caban T, White PJ. The national health information technology human factors and ergonomics agenda. Appl Ergon. 2020;86:103109. 32. Ginsburg G. Human factors engineering: a tool for medical device evaluation in hospital procurement decision-making. J Biomed Inform. 2005;38:213–219. 33. Chera BS, Mazur L, Buchanan I, et al. Improving patient safety in clinical oncology: applying lessons from normal accident theory. JAMA Oncol. 2015;1:958–964. 34. McLeod RW. Human factors in barrier management: hard truths and challenges. Process Saf Environ Protect. 2017;110:31–42. 35. Jackman DM, Foster E, Hamilton JM, et al. Early findings on the use of clinical pathways for management of unwarranted variation in cancer care. Am J Med Qual. 2021. 36. Ezzell G, Chera B, Dicker A, et al. Common error pathways seen in the RO-ILS data that demonstrate opportunities for improving treatment safety. Pract Radiat Oncol. 2018;8:123–132.
留言 (0)