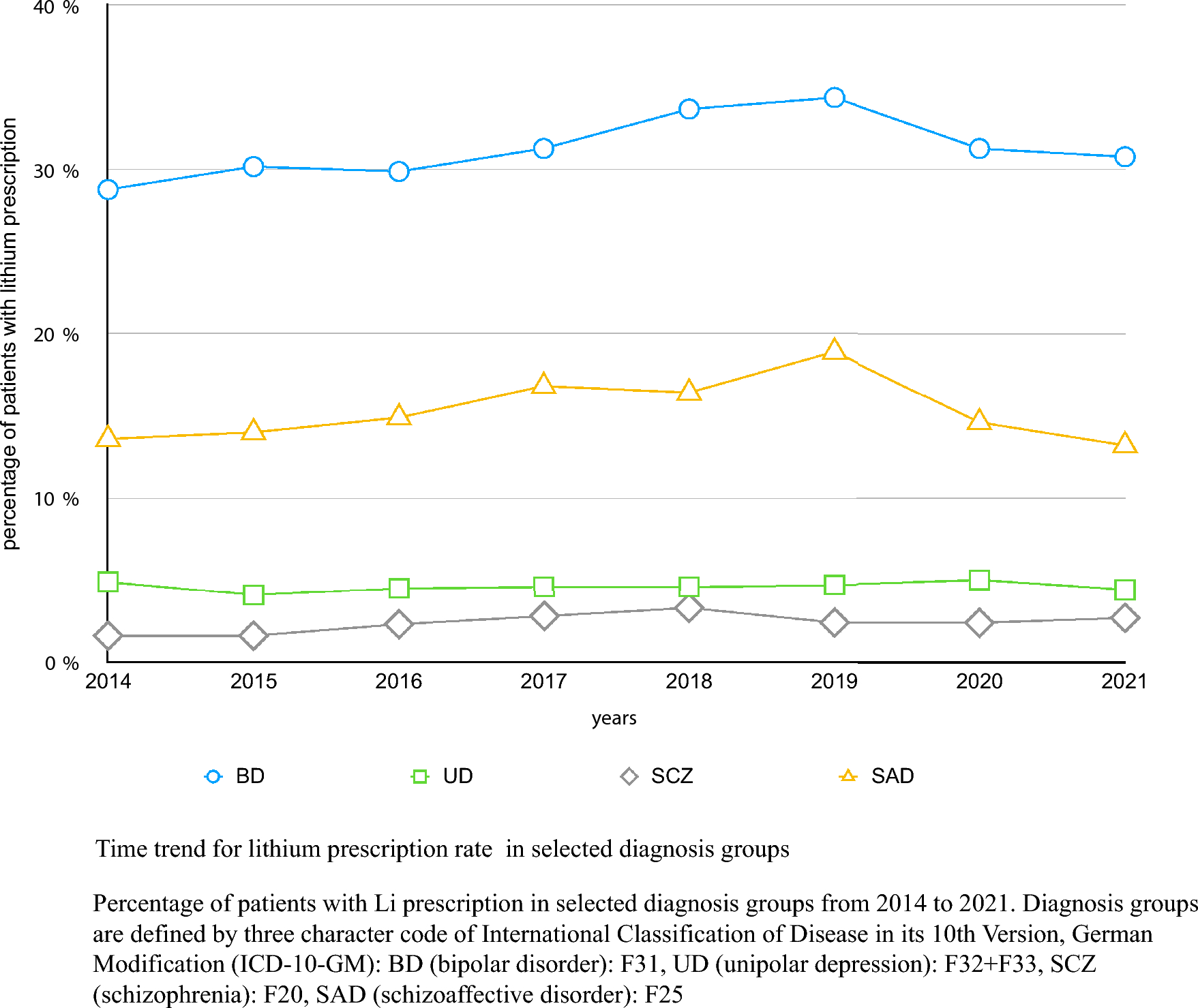
Despite the fact that lithium is consistently ranked as the first choice medication for the long-term treatment of bipolar disorders in international guidelines lithium prescriptions are declining in many countries (Malhi et al. 2023). Alterations of renal function from lithium have been well described for a very long time. Close to a century before Cade’s first seminal report on the efficacy of lithium in treating acute mania (Cade 1949), the diuretic effect of lithium (clinically manifested as polyuria) was noted in a number of reports in the 1860s (summarized in Johnson, 1980), suggesting its use as a clinical diuretic in disorders such as gout. In 1977, ‘the kidney scare” from lithium emerged from preliminary biopsy studies of selected lithium- treated patients which showed clear evidence of structural renal damage, primarily in the form of interstitial nephritis (with scarring of the interstitium, tubular destruction and relative preservation of glomeruli [Hestbech et al. 1977]). As noted by Schou and Vestergaard three years later, clinicians were appropriately concerned about these findings, asking “are we buying the mental health of lithium-treated manic-depressive patients at the expense of their kidney function and survival? Should we perhaps stop using lithium?” (Schou and Vestergaard, 1980). Their answer was, not surprisingly “no”. After acknowledging the data available at that time on both polyuria and potential morphological kidney changes during lithium treatment, they appropriately recommended that these effects do not justify radical changes in the use of lithium. Surprisingly, they did not consider monitoring of renal function such as serum creatinine determinations mandatory.
Now, forty three years later, we have learned a great deal more about the renal effects of lithium and the potential risks of long term renal damage. Yet, the questions generated almost half a century ago are still relevant and will be addressed in this paper:
1)
What is the risk of polyuria among lithium-treated patients?
2)
What is the risk of mild to moderate renal damage from lithium as measured by the estimated glomerular filtration rate (eGFR)?
3)
What is the relationship between polyuria/nephrogenic diabetes insipidus and the development of chronic kidney disease (CKD) among a lithium treated population?
4)
What is the risk of end stage renal disease (ESRD), defined as an eGFR < 15 ml/min, in patients taking lithium?
5)
What is the course of renal function in lithium treated patients who discontinue lithium due to CKD?
Risk of polyuria among lithium-treated patients
Urinary frequency, i.e., polyuria, is the most common side effect of lithium. Estimates of polyuria vary with estimates up to 70% with a range of 20–87% (Goldberg and Ernst 2012; Azab et al. 2015). Nephrogenic diabetes insipidus (NDI), also known as arginine vasopressin resistance (AVP-R), defined as a 24 h urine volume of 3,000 ml/day or more is both measured less frequently and is less prevalent with estimates ranging between 3 and 17% (Damba et al. 2022). Thirst and polyuria are not always well correlated with formally defined NDI, especially in older patients (Rej et al., 2014a). Additionally, patients are often imprecise and even mistaken in their subjective sense of increased urination/polyuria. Although difficult, a formal 24 h urine collection is the definitive method for ascertaining the presence of polyuria. The overall mechanism by which lithium causes NDI is thought to be resistance to antidiuretic hormone (ADH), especially through its effects at the distal tubules and collecting ducts (Davis et al. 2018a; Lerma, 2023). More specifically, lithium accumulates in the principal cells of the collecting duct, reducing the phosphorylation of aquaporin 2 (AQP2), thereby reducing the reabsorption of free water and resulting in the excretion of a more dilute urine. (See Davis et al. 2018a for more details).
Factors that have been reported to increase the risk of lithium induced polyuria include: duration of lithium treatment; serum lithium level; and number of episodes of lithium intoxication. It is thought that the polyuria is initially functional (similar to what is seen with alcohol use) and reversible but becomes structural and less reversible with time. It has been estimated that the polyuria is usually reversible in the first 2–6 years of treatment (Schoot et al. 2020). Concomitant use of antipsychotics has been reported to increase the risk of lithium-induced polyuria.
The regimen by which lithium is prescribed may also correlate with polyuria. Both animal studies and studies in clinical populations suggest that lithium induced damage to the renal tubular systems is minimized by regimens that result in a very low daily trough lithium level (Gitlin 1999). Rats treated with lithium at a relatively constant concentration show reduced renal concentrating ability and greater tubular and interstitial scarring on biopsy specimens compared to rats treated with a regimen producing high peaks alternating with low trough lithium concentrations (Plenge et al. 1981). Clinically, low trough levels can best be achieved by once daily administration of non-sustained release lithium carbonate capsules. Thus, even though it is superficially paradoxical, steadier lithium levels across a 24 h period, which would be obtained by a regimen of twice or three times daily lithium administration using a sustained release preparation may result in greater tubular damage and therefore higher rates of polyuria/NDI compared to once daily lithium capsules. Some early studies, however, did not demonstrate improvement in polyuria when patients were switched to a once daily lithium regimen except in those who had been treated with lithium for five years or less (Kusalic et al., 1996), again suggesting the gradual transition from a functional to a structural, less reversible deficit. Therefore, for patients who have been treated for lithium on twice daily regimens for long time periods-e.g. ten years or more, switching to a once daily regimen may not be beneficial. Since CNS lithium levels vary far less throughout a 24 h period than does the serum level, the high peak/low trough pharmacokinetic curve does not interfere with lithium’s efficacy.
For patients with lithium induced polyuria which is symptomatically distressing and functionally impairing-e.g. sleep disruption due to recurrent nocturia, both amiloride (Batlle et al. 1985) and thiazide diuretics can be helpful. Amiloride inhibits the uptake of lithium in the principal cells of the epithelial sodium-channel while thiazides reduce distal delivery of tubular fluid resulting from increased proximal sodium and water uptake (Schoot et al. 2020). Thiazides increase serum lithium levels, thereby typically requiring a decrease in daily lithium dose to maintain constant levels.
Risk of renal damage (CKD) as measured by eGFR
Although polyuria is distressing and may decrease quality of life-especially in patients with marked nocturia disrupting sleep- as long as patients respond to thirst and have access to sufficient liquids to stay hydrated, it is not a substantial health risk. However, with progressive scarring from the primarily interstitial disease associated with long term lithium use, glomerular function may begin to be compromised. Most but not all studies use CKD stage 3 defined as eGFR < 60 ml/minutes as the cutoff when dichotomizing renal function. Table 1 presents current classification of chronic kidney disease. Two important confounding factors are bipolar disorder itself and age. Bipolar disorder itself is associated with a decrease in average life span and specifically in rates of mild to moderate CKD as well as end stage renal disease (Kessing et al. 2015). Normal aging is also associated with the development of mild to moderate CKD-3. Normal age-related renal function deterioration has been estimated as decreasing eGFR of 0.4 ml/minute/year (Wetzel et al., 2007; Hill et al. 2016).
Table 1 Stages of Chronic Kidney DiseaseA number of recent reviews have surveyed the field, addressing the rate of CKD stage 3 in lithium treated patients and compared them to either age matched controls or to patients treated with other mood stabilizing agents (Lerma 2023; Schoretsanitis et al., 2021; Damba et al. 2022; Schoot et al. 2020). A recent estimate of the rate of CKD stage 3 in lithium treated patients was 26% (Schoretsanitis et al., 2021). A review of 15 papers found that all 15 studies found a positive association between CKD stage 3 and lithium with cumulative incidences ranging between 2 and 40% (Damba et al. 2022). Two studies each estimated the rate of CKD-3 was 30% higher in lithium treated patients compared to a control population (Tondo et al. 2017; Van Alphen et al. 2021). Another review estimated that the risk of CKD Stages 3–5 was five fold higher in patients on long term lithium treatment (Schoretsanitis et al., 2021). Most, but not all studies (Kessing et al. 2015; Bosi et al. 2023) found that lithium was associated with higher rates of CKD 3 compared to other mood stabilizing agents.
Other than age (which is a risk factor for CKD 3 for all populations), the most consistent risk factor for lithium-induced renal disease is length of exposure to lithium (Hojlund et al. 2022). Despite occasional reports of lithium induced CKD after relatively shorter exposures-i.e., years, not decades (Damba et al. 2022; Gitlin 2023), most patients with CKD have been on lithium for twenty years or more. One recent study demonstrated that the average annual decline in eGFR in lithium treated patients differed from a control population only after ten years of lithium exposure (Fransson et al. 2022). Other risk factors found in most but not all studies are episodes of lithium toxicity, higher lithium levels, the use of other psychotropic medications and comorbid medical disorders associated with renal damage such as diabetes mellitus and hypertension (Damba et al. 2022; Hojlund et al. 2022). Other potential risk factors recently identified are female sex (which increases the risk for CKD generally) and a history of migraines (Hayes et al. 2021).
Although virtually all Practice Guidelines recommend regular (between every three months to every year, depending on the guidelines) monitoring of renal function, in clinical practice, monitoring of lithium levels and renal function in lithium treated patients may be far less frequent. As one example, in a French study, during an eight year period, of 1179 lithium treated patients, 41% had no creatinine measurement (Bassilios et al. 2008). The overall recommendations for lower lithium levels-0.6-0.8 mEq/ml vs. 0.8-1.0mEq/ml- should also be the goal for most patients. Even one lithium level > 1.0 mEq/L has been reported to be associated with a lower eGFR for three months (Kirkham et al. 2014). Whether this reflects a transient or a longer term effect on renal function is unknown.
Relationship between polyuria/ nephrogenic Diabetes insipidus and the development of chronic Kidney Disease (CKD)
Since the mechanism by which lithium causes both polyuria/NDI and CKD are presumed to be the same-interstitial nephritis- it may equally be assumed that the presence of polyuria/NDI would be a strong risk factor for the development of CKD. Surprisingly, this has been rather infrequently studied. One study found a correlation between low urine specific gravity (a marker for NDI) with long term renal decline as measured by a lower eGFR (Sajadi et al., 2016). Neither of the most recent comprehensive reviews evaluated polyuria as a predictor of CKD in lithium treated patients. (Schoretsanitis et al., 2021; Damba et al. 2022). An earlier review simply stated that “polyuria only weakly predicts increasing creatinine or reduced kidney function” (Azab et al. 2015). Many clinicians have anecdotally seen patients who have substantial and distressing polyuria but whose eGFR is normal (> 80 ml/min). Of note, some bipolar patients may have psychogenic polydipsia in which the polydipsia is primary and the polyuria is secondary, whereas with lithium the polyuria is primary. Whether this reflects the relative preservation of glomeruli compared to tubular damage consistent with interstitial nephritis or is the consequence of additional factors such as psychogenic polydipsia is unknown. Of note, some bipolar patients may have psychogenic polydipsia in which the polydipsia is primary and the polyuria is secondary whereas with lithium, the polyuria is primary.
Risk of end stage renal Disease (ESRD)
Even though lithium substantially increases the risk of CKD Stage 3, if the renal insufficiency stays static and does not progress further, the risk/benefit ratio would overwhelmingly favor the continued use of lithium. Thus, the most important question in exploring the relationship between lithium and renal function is whether lithium can cause severe renal disease (typically defined as CKD stage 4–5) and/or true end stage renal disease (ESRD), typically defined as an eGFR < 15 ml/min and leading to either renal dialysis or transplantation. A number of studies, cross-sectional as well as longitudinal studies (Aiff et al., 2014a; Aiff et al., 2014b; Aiff et al. 2015; Bendz et al. 2010; Close et al. 2014: Rej et al., 2014b; Roxanas et al. 2014), supplemented by small case series (Gitlin 1993, 2023: Azab et al. 2015) have examined this issue.
The most persuasive data are those from the Swedish cohort of patients on either dialysis or renal transplantation in two geographical areas, totaling 2.8 million inhabitants (Aiff et al., 2014a; Aiff et al., 2014b; Aiff et al. 2015). ESRD was more prevalent among lithium users than non-lithium users with a risk ratio of 7.8 (Aiff et al., 2014a). Consistent with other earlier studies, the lithium/ESRD patients had been treated for a very long time with a mean time of 27 years (12–39). A follow-up study, however, suggested that the lower lithium levels used in more recent cohorts may substantially reduces this risk (Aiff et al., 2014b). In a follow-up of patients who started lithium during the observation period, 5% had progressed to CKD 4–5 (Aiff et al. 2015). As acknowledged by the authors (Aiff et al., 2014a; Aiff et al., 2014b; Bendz et al. 2010), patients in these studies may be misclassified, either because they did not disclose or forgot about their lithium treatment or escaped registration in the Swedish Renal Registry, thereby making their findings less definitive. Additionally, although many of these studies (Aiff et al., 2014a; Aiff et al., 2014b; Bendz et al. 2010) attempted to examine potential factors for ESRD other than lithium in their study population, it must be acknowledged that other risk factors such as other medications, the effect of psychiatric disorders or some medical comorbidities might still explain some of the findings.
A few case series have highlighted the vulnerability of short term follow-up studies in missing what are long term clinical complications (Azab et al. 2015; Gitlin 2023). Although the nature of these case series preclude estimating reliable probabilities of ESRD from lithium, they demonstrate that some lithium treated patients, regardless of whether they continue lithium may, even decades later, show progressive renal insufficiency, potentially leading to ESRD, dialysis or renal transplantation.
Finally, one recent study demonstrated, not surprisingly, that individuals with higher serum creatinine before beginning lithium treatment were far more likely to progress to CKD 4–5 vs. those with normal serum creatinine level pre-lithium (48% vs. 10%, p < .001, with a hazard ratio of 6.7) (Golic et al. 2021).




留言 (0)