This study illustrated that preoperative sleep disorders were independently correlated with PD, in addition to the usual risk factors.
Delirium is frequently encountered in the ICU. Precipitating factors related to the treatment include: respiratory failure, shock, metabolic disturbances, prolonged mechanical ventilation, pain, immobility, sedatives and adverse environmental conditions impairing vision, hearing, and sleep [17]. Postoperative delirium was also associated with baseline conditions in ICU patients [18]. The management of ICU delirium has historically been challenging, as very few pharmacological options have demonstrated efficacy in treating delirium once it develops. However, it is difficult to ensure that the anesthesiologist involved in the assessment of a patient’s postoperative delirium is completely unaware of whether the patient is an ICU patient, because the conscious state of the patient admitted to the ICU determines the need for the patient to use the ICU-CAM to assess delirium. ICU admission as a risk factor may therefore be biased.
Evidence suggests that undernutrition negatively impacts health-related quality of life and postoperative outcomes [19, 20]. Elderly patients with proximal femoral fracture are often prone to metabolic disorders, low calorie consumption, impaired nutrition and concomitant cerebrovascular disease leading to impaired nutritional intake [21]. However, there was no significant difference in BMI or the Albumin level between the two groups. A larger sample size may be needed.
Risk factors for PD can be roughly divided into two categories: predisposing factors and precipitating factors. The predisposing factors include advanced age, dementia, cognitive impairment, multiple medical diseases, hearing and visual impairment, and history of alcohol consumption. The precipitating factors include pain, depression, anemia, infection, malnutrition, activity limitation, hypoxemia, dehydration and electrolyte disturbances, acid-base imbalance, urinary retention and constipation, medications (anticholinergic drugs, etc.) and sleep disorders.
The mechanisms by which sleep disorders cause cognitive and behavioral dysfunction are not well understood. Both anxiety, depression and sleep apnea (OSA) can lead to sleep disorders. Chronic insomnia caused by anxiety and depression is associated with impairment of alertness, orientation, and behavioral control [22, 23]. A previous study found that chronic intermittent hypoxemia and hypercapnia that result from OSA can also impair attention, memory, and cognition [24]. It has been reported that a large amount of cortisol production induced by hypothalamic‒pituitary‒adrenal axis hyperexcitability is transferred to the central nervous system, leading to apoptosis of neurons in the hippocampal area through activation of the brain-derived neurotrophic growth factor-tropomyosin-related kinase B signaling pathway, which may be a possible mechanism that explains how sleep disorders influence cognitive and behavior dysfunction [25]. Another study illustrated that hypoxemia and hypercapnia caused by long-term OSA can also damage vascular endothelial cells, improve the sensitivity of the vasoconstrictive response, produce an oxidative stress response leading to a hypercoagulable state, and increase the risk of vascular dementia [26]. Moreover, another study found that neuronal apoptosis induced by sleep disorders, related to autonomic nervous system imbalance, may also be the mechanism. Therefore, the relevance of studying the impact of preoperative sleep quality on PD for patients is clear.
In the current study, we found that ASA classification, age, preoperative albumin level, preoperative hemoglobin level, operation type, preoperative coronary heart disease, and postoperative ICU admission may be risk factors associated with PD through univariate analysis. However, none were determined because of their interaction with each other. We used multiple logistic regression models to adjust for covariates, and the models showed that preoperative sleep disorders and postoperative ICU admission were reliable independent risk factors.
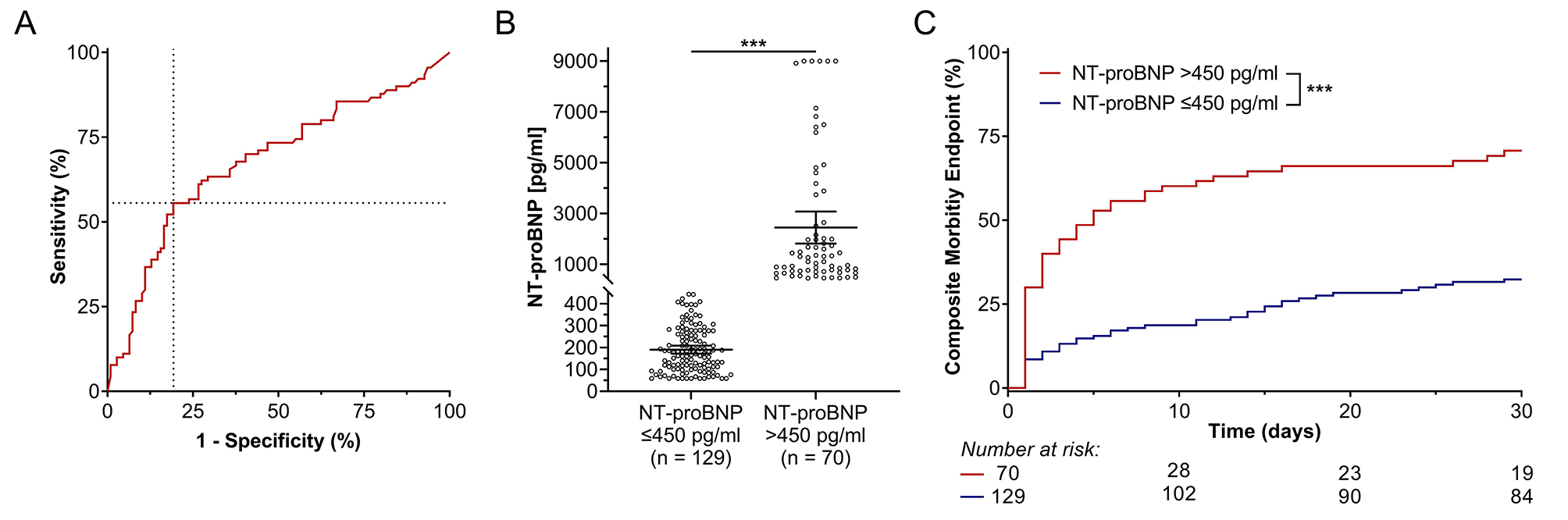
The AUC generated from the ROC curve can predict the diagnostic value of a risk factor for the outcome. An AUC greater than 0.7 means that the risk factor has a certain accuracy in predicting the outcome. The ROC curve was used to observe the effect of the preoperative PSQI score on the incidence of PD, and the AUC obtained was 0.808, indicating that the preoperative PSQI score is a diagnostic factor for PD. The results showed that the PSQI had certain diagnostic value for PD.
Our study has some advantages in demonstrating that preoperative sleep disorders are associated with PD. First, prospective observational studies can avoid bias caused by retrospective studies. Second, the preoperative sleep quality of patients was assessed by the PSQI, which has a sensitivity of 89.6% and a specificity of 86.5% for the judgment of sleep quality. It can analyze sleep disorders caused by anxiety, depression and breathing problems, and describe sleep conditions comprehensively and specifically. Third, the program of general anesthesia was standardized to decrease the possibility of a narcotic administration bias.
This study has several limitations. First, since this study included elderly patients, subacute delirium may be misdiagnosed as a deconditioning postoperative event. Delirium could be underestimated when symptoms involve hypoactive conditions. We are unsure of how a higher incidence of PD could influence the outcome. Second, the PSQI and CAM are self-report questionnaires for sleep quality and delirium, so there must be some bias in the diagnosis of SPD and PD. Polysomnography, electroencephalography and blood tests may help. Third, this study has a small sample size and a short research time. Studies with larger sample sizes are needed.


留言 (0)