
記住我

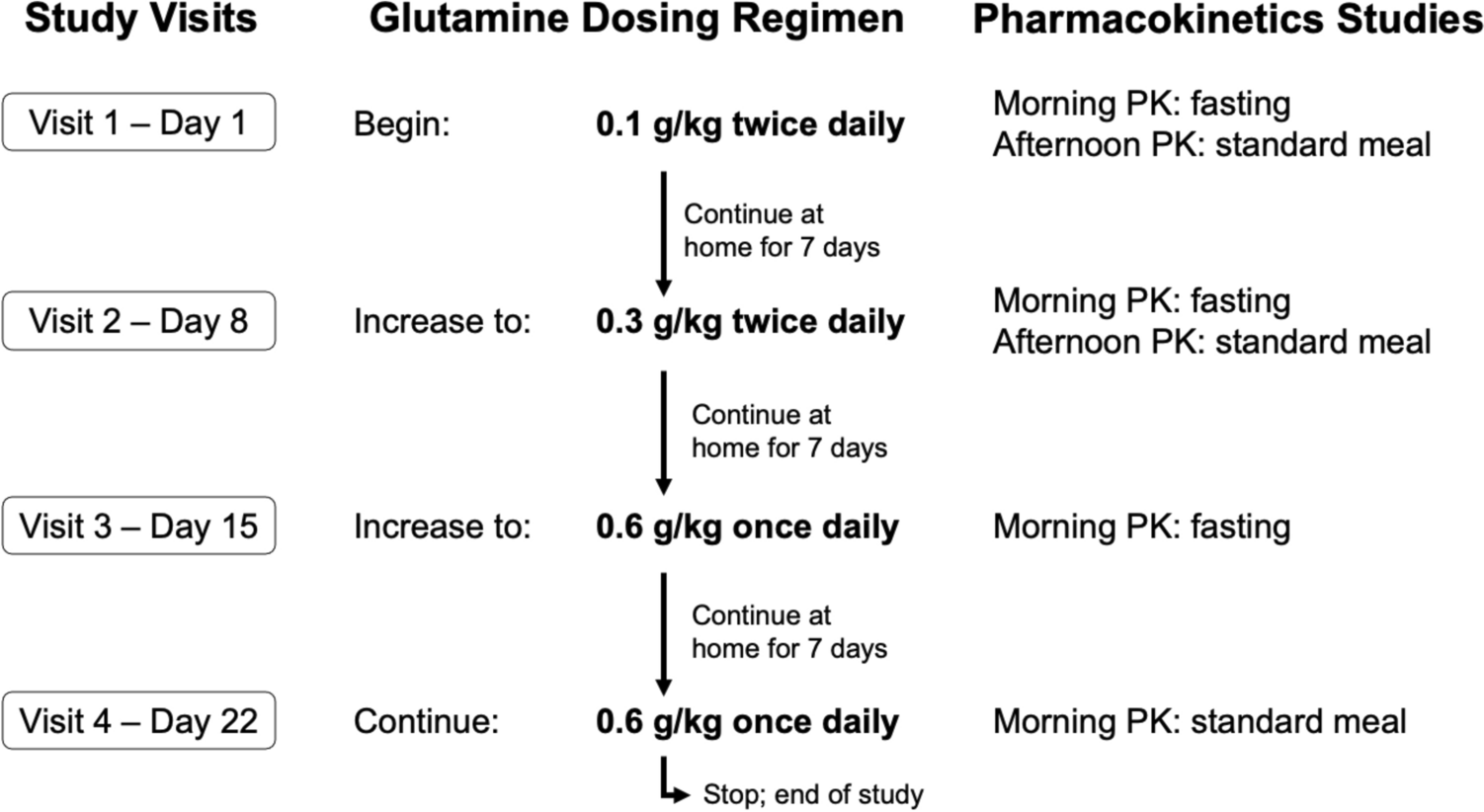
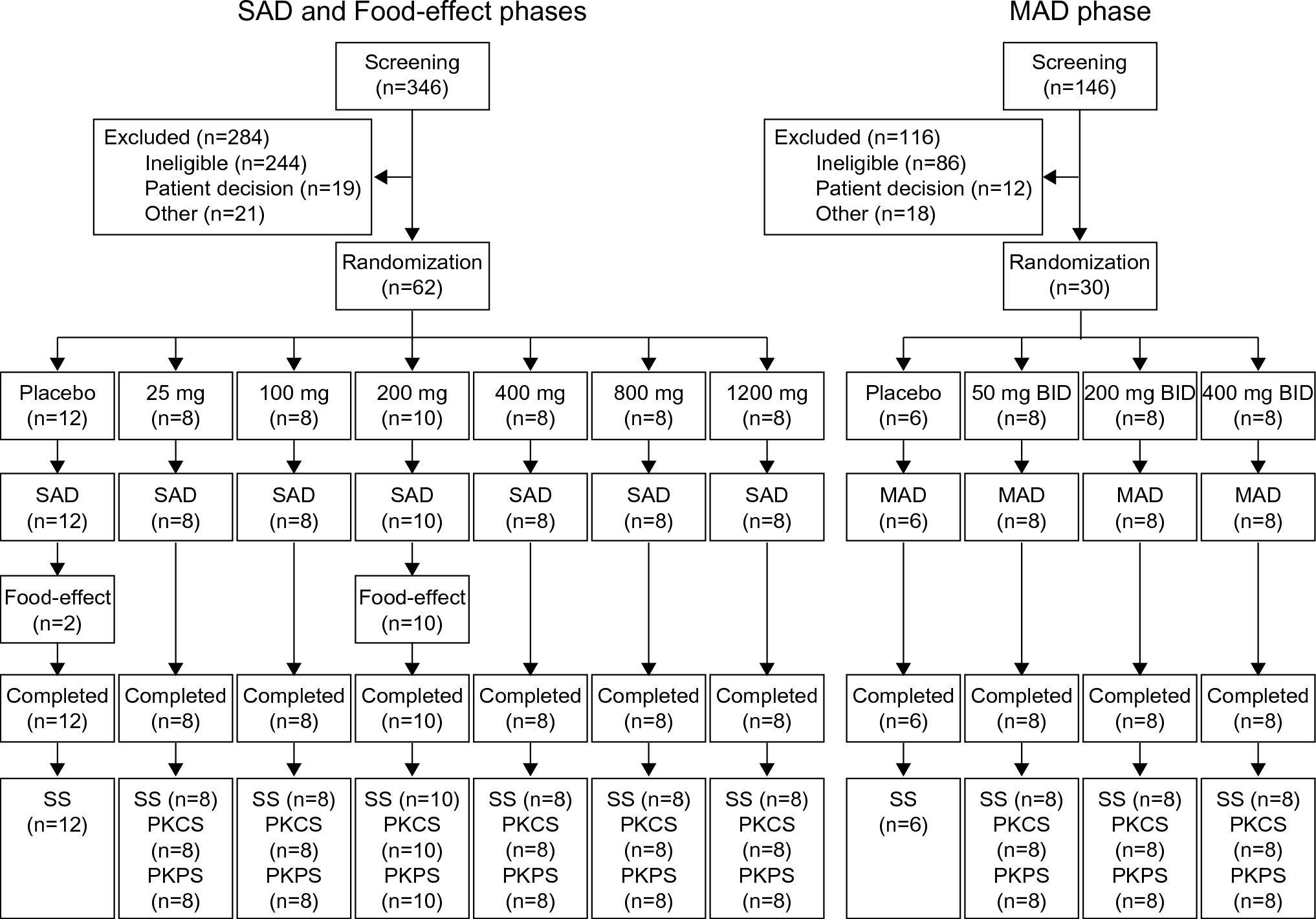

This was a two-part, Phase 1, multicenter, randomized, placebo-controlled, single-blind study (ClinicalTrials.gov: NCT04988152; Fig. 1). In Part 1, healthy Japanese and Caucasian volunteers were randomized (ratio 4:1) to receive a single 500 mg IV 30-min infusion of sotrovimab or matching placebo on Day 1. Part 2 involved a different group of healthy volunteers to Part 1, and commenced after enrollment was completed for Part 1; healthy Japanese and Caucasian volunteers were randomized to receive a single 500 mg IM dose of sotrovimab or matching placebo (ratio 4:1) on Day 1, administered as two 4-mL injections (one in each dorsogluteal injection site).
Fig. 1
Study design. EOS end of study, IM intramuscular, IV intravenous, PK pharmacokinetics
2.1 ParticipantsEnrollment occurred at two Phase 1 clinical units in the USA. Healthy volunteers could be included if they were capable of giving informed consent, were aged 18 to ≤ 65 years, and had a body mass index (BMI) between 18 and 29.9 kg/m2. Participants aged 55 years or older were required to have received all doses in a primary SARS-CoV-2 vaccine series at the time of signing informed consent. All participants were required to test negative for COVID-19, determined by two consecutive SARS-CoV-2 negative reverse transcriptase polymerase chain reaction tests. Female participants were required not to be pregnant or breastfeeding.
Japanese participants had to meet all of the following criteria: be of Japanese ancestry, defined as having been born in Japan and being descendants of four ethnically Japanese grandparents and two ethnically Japanese parents; hold a Japanese passport or identity papers; be able to speak Japanese; and have lived outside of Japan for fewer than 10 years at the time of screening. Caucasian participants had to be of Caucasian ancestry, as evidenced by appearance and verbal confirmation of familial heritage (two Caucasian parents and four Caucasian grandparents).
Participants were excluded from the study if they had a history or presence of cardiovascular, respiratory, hepatic, renal, gastrointestinal, endocrine, hematologic, or neurological disorders capable of significantly altering the absorption, metabolism, or elimination of drugs; or constituting a risk when taking the study intervention or interfering with the interpretation of data; lymphoma, leukemia, or any malignancy within the past 5 years, except for basal cell or squamous epithelial carcinomas of the skin that had been resected with no evidence of metastatic disease for 3 years, or breast cancer within the past 10 years; presence of hepatitis B surface antigen, a hepatitis C antibody test result, or a hepatitis C ribonucleic acid test result at screening or within 3 months prior to the first dose of study intervention, or a positive human immunodeficiency virus antibody test. Prohibited prior or concomitant therapy included treatment with biological agents (such as mAbs, including marketed drugs) within 3 months or five half-lives (whichever was longer) prior to dosing, convalescent plasma from a recovered COVID-19 patient, and an anti-SARS-CoV-2 mAb within the last 3 months.
Participants were admitted to the unit on Day − 1, following screening between Day − 1 and Day − 28. Dosing took place on Day 1, and participants remained at the unit for the first 3 days. Following discharge, they returned for follow-up safety assessments and blood sampling up to Week 18. Blood samples were collected on Days 1, 2, 3, 8, 15 (± 1 day), 29 (± 2 days), 43 (± 3 days), 57 (± 4 days), 85 (± 7 days), and Day 127 (± 7 days).
2.2 Objectives and EndpointsThe primary objectives in Part 1 were to assess the PK, safety, and tolerability of sotrovimab administered via IV infusion in healthy Japanese and Caucasian participants through Day 29 (in line with the pivotal COMET-ICE efficacy study [7]). The primary objectives in Part 2 were to assess the PK, safety, and tolerability of sotrovimab administered via IM injections in healthy Japanese and Caucasian participants through Day 29.
The primary PK endpoints were maximum observed serum concentration (Cmax), area under the serum concentration-time curve from Day 1 to Day 29 (AUCD1–29), time to Cmax (Tmax), and serum concentration at Day 29 (CD29) of sotrovimab were observed. Measurement of sotrovimab serum concentration was performed using a validated electrochemiluminescence immunoassay method (lower limit of quantification 0.1 μg/mL). The primary safety endpoints included occurrence of adverse events (AEs), serious AEs (SAEs), and AEs of special interest (AESI; infusion-related reactions, including hypersensitivity reactions, injection-site reactions, immunogenicity-related adverse drug reactions, and AEs potentially related to antibody-dependent disease enhancement) through Day 29. Severity of AEs was graded according to the Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events, version 2.1 (July 2017). Clinically significant electrocardiogram (ECG) abnormalities, vital signs, and laboratory parameters were also evaluated.
Secondary objectives were to assess PK (Cmax, area under the plasma concentration-time curve from time zero to infinity [AUCinf], area under the concentration-time profile to the last measurable concentration [AUClast], Tmax, time of last analytically quantifiable concentration [Tlast], terminal half-life [t½], as data permit) and safety through Week 18. In addition, AUCinf following IV and IM administration (absolute bioavailability) was intended to be assessed; however, AUClast was used instead, due to the number of participants with the extrapolated portion of AUCinf as a percent (%AUCextrap) > 20 %.
Immunogenicity (the presence of antidrug antibodies [ADAs]) through Day 29 and Week 18 was an exploratory endpoint. Antibodies to sotrovimab were evaluated in serum samples collected from all participants. Antidrug antibodies were assessed using a validated, multi-tiered approach, consisting of screening, confirmation, and titration assays, to evaluate anti-sotrovimab antibodies.
2.3 AssaysSotrovimab concentrations in serum were determined via a validated electro-chemiluminescent (ECL) method, which used anti-idiotypic antibodies specific to sotrovimab for capture and detection. Human serum samples were minimally diluted 25-fold with assay buffer (1 % bovine serum albumin in phosphate-buffered saline [PBS]) prior to analysis. The diluted serum samples were added to an Meso-scale discovery (MSD) High Bind plate (ECL capable) adsorbed with AbD34205-mu-IgG2a capture antibody and ruthenylated-AbD42688-rFab antibody to detect sotrovimab. A fixation step (freshly prepared 1 % formaldehyde in PBS) was applied, followed by MSD read buffer. The assay plate was then read using an MSD ECL plate reader. The quantifiable analytical range for the method was 100 to 10,000 ng/mL.
A three-tier approach (screen, confirm, titer) was used to detect any ADA to sotrovimab. Validated ECL bridging assays were used to analyze the samples. The cut point factors of 1.300 and 1.548 for the screen and titer assay, respectively, and the confirmatory cut point of 32.347 % were determined statistically using 50 lots of COVID-19-positive human serum. The screening and confirmatory sensitivity were established to be 22.970 and 31.812 ng/mL, respectively, using an anti-idiotype antibody to sotrovimab as positive control.
2.4 Statistical AnalysisNo formal statistical technique was used to calculate the study sample size, and no hypothesis-testing was conducted. Sample size was based on sufficiency to adequately estimate the ratio of exposures between Japanese and Caucasian participants, and IV and IM administration routes.
The PK analysis set included all participants in the safety analysis set who had at least one PK observation available. The safety analysis set included all randomized participants who were exposed to the study treatment.
Pharmacokinetic parameters were calculated using standard non-compartmental methods. Pharmacokinetic comparisons through Day 29 between Japanese and Caucasian participants were made using an analysis of covariance (ANCOVA) model with loge-transformed Cmax or AUCD1–29 as dependent variables and adjusting for loge-transformed body weight (to incorporate allometry). The geometric least squares (LS) means ratio of Cmax and AUCD1–29 (Japanese and Caucasian participants) and associated 90 % confidence intervals (CIs) were calculated. Pharmacokinetic comparisons through Week 18 were made in a similar way, and geometric LS means ratio of AUClast (Japanese and Caucasian participants) and associated 90 % CIs were calculated.
An exploratory comparison of bioavailability (AUClast ratio) following a single IM dose of 500 mg sotrovimab (Part 2) relative to the single IV dose of 500 mg sotrovimab (Part 1) was performed using an ANCOVA model, with loge-transformed AUClast as a dependent variable and adjusting for ethnicity and body weight (loge-transformed), and included all participants.
Safety data were summarized using frequency and percentages.
留言 (0)