
記住我






The global burden of musculoskeletal (MSK) pain is high,9 and its impact on disability exceeds that of other noncommunicable diseases,11 resulting in enormous direct, indirect, and intangible costs.7 Among MSK pain conditions, low back pain (LBP) is the most common, affecting around a third of people globally every year.28,31 Accordingly, LBP is also a leading cause of disability,12,59 which is projected to increase due to ageing populations.40
Many people with LBP experience ongoing low-grade pain that alternates with periodic flare-ups,19,34 and co-occurring pain in other body sites alongside persistent LBP is common.27,29,44,48,52 A recent systematic review of observational studies found that people with persistent LBP often report co-occurring axial, extremity, and multisite pain48; however the included studies were heterogeneous and the assessment of co-occurring pain differed substantially between the included studies and none assessed long-term trends. Hence, there is a knowledge gap concerning the prevalence and long-term patterns of persistent LBP with co-occurring MSK pain in the general adult population. Moreover, distinct subgroups with different anatomical pain patterns (ie, phenotypes) may exist on the continuum between LBP only and widespread, persistent MSK pain with LBP as 1 component.15 Identifying LBP phenotypes is relevant because co-occurring MSK pain is associated with more negative consequences, such as reduced workability, increased healthcare utilization, and poorer response to treatment compared with single-site MSK pain.2,6,19,20,26,29,43,48 However, counting the number of pain sites may be too simplistic because certain pain sites or pain patterns among people with persistent LBP may have diverse consequences and affect prognosis or treatment outcomes differently.27 Distinct LBP phenotypes may have features requiring a stratified care approach,53 and including them in the management of LBP rather than approaching LBP as a single entity could offer the possibility of larger treatment effects. Knowledge about LBP phenotypes may contribute to the field by informing future studies, clinical practice, and health policy, which in turn could lead to better use of resources30,41 and improved patient outcomes.22
The Norwegian population-based HUNT Study3,36 provides rich data from consecutive cross-sectional surveys that allow us to investigate the prevalence and pattern of persistent LBP and co-occurring MSK pain and its consistency in the general population over 3 decades. The objectives of this study were therefore 2-fold: (1) to describe the prevalence of co-occurring persistent MSK pain among people with persistent LBP and (2) to identify patterns of persistent LBP with co-occurring MSK pain and the temporal stability of these patterns across time.
2. Methods 2.1. Study design, setting, and populationThe HUNT Study is a population-based study consisting of 4 consecutive surveys inviting all inhabitants in the Nord-Trøndelag region in Norway aged 20 years or older. The current study use data from the 3 latest surveys where information on MSK pain was collected (HUNT2, 1995-1997; HUNT3, 2006-2008; and HUNT4, 2017-2019). In total, 65,237 (69.5%) participated at HUNT2 of the 93,898 who were invited, whereas the corresponding numbers at HUNT3 and HUNT4 were 50,807 (54.1%) of 93,860 and 56,042 (54.0%) of 103,800, respectively. We selected all participants from each survey who had information on persistent MSK pain and reported having persistent LBP pain (ie, 15,375 participants in HUNT2, 10,024 in HUNT3, and 10,647 in HUNT4). These represent 27,607 unique individuals with persistent LBP of whom 20,706 reported LBP in only one of the HUNT2, HUNT3, or HUNT4 surveys, whereas 6901 reported LBP in at least 2 of the surveys.
To arrive at this sample size with complete information, we excluded 458 individuals who reported MSK pain without specifying the pain site, 153 individuals with chest pain only, and 190 individuals from HUNT4 with missing information on age. Detailed descriptions of HUNT Study participation, data collection procedures, and sample characteristics can be found in previous publications.3,36 The Trøndelag Health Study (HUNT) is a collaboration between HUNT Research Centre (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology NTNU), Trøndelag County Council, Central Norway Regional Health Authority, and the Norwegian Institute of Public Health. Further information about the HUNT Study can be found at https://www.ntnu.edu/hunt.
2.2. Data collection and variables 2.2.1. Low back pain and co-occurring musculoskeletal painQuestions on MSK pain were adopted from the Standardized Nordic Questionnaire, commonly used to measure MSK complaints with acceptable reliability25,37 and sensitivity.17,49 At HUNT2, participants were asked, “During the last year, have you had pain and/or stiffness in your muscles and limbs that have lasted for at least 3 consecutive months?”, whereas at HUNT3 and HUNT4, participants were asked, “In the last year, have you had pain or stiffness in muscles or joints that have lasted at least 3 consecutive months?”. Response options were “yes” and “no.” Participants who responded “yes” were defined as having persistent MSK pain. People who answered “yes” were asked to indicate the affected body area, ie, lower back, upper back, neck, shoulders, elbows, wrists or hands, hips or thighs, knees, and ankles or feet, with the option of checking all relevant areas. For this study, we included participants who reported persistent LBP, and this was regarded as the primary pain site, whereas co-occurring MSK pain was defined as pain reported in sites additional to LBP.
2.2.2. Other variablesInformation on demographics and health-related characteristics was obtained from each HUNT survey questionnaire. The level of education was dichotomized into “higher” (university/college >4 years and ≤4 years) and “lower” education (primary school/high school/vocational school). Body mass index (BMI) was calculated as weight divided by the square of height (kg/m2) using data from standardized measurements obtained at the clinical examinations. Symptoms of anxiety and/or depression were assessed by the Hospital Anxiety and Depression Scale (HADS) using a cutoff score of ≥8 on either the anxiety or the depression scale.8 Three questions assessed sleep problems: difficulty falling asleep at night, waking up too early, and inability to fall asleep again. Participants were classified as having “poor sleep” if they answered “several times a week” to at least one of the questions.56 Long-term health conditions were assessed by the question, “Do you suffer from any long-term illness or injury of a physical or psychological nature that impairs your functioning in your everyday life?” with response options “yes” or “no.” Self-rated health was evaluated by the question “How is your health at the moment?”, and the 4 response options were dichotomized into 2 groups, “very good or good” and “not so good or poor.”
2.3. Statistical analysisDescriptive statistics are reported as proportions for categorical variables and means with standard deviations for continuous variables. Prevalence of co-occurring MSK pain alongside persistent LBP is presented as proportions with 95% confidence intervals (CIs). To enable comparisons of prevalence estimates across the 3 HUNT surveys, all estimates were standardized according to the age distribution at HUNT2 using direct standardization within the categories 19 to 29, 30 to 49, 50 to 69, and ≥70 years.
Latent class analysis (LCA) was used to identify phenotypes of people reporting persistent LBP combined with the 9 possible co-occurring pain sites. Latent class analysis uses a data-driven probabilistic approach to explore and identify unobserved subgroups or latent classes in a population with shared scoring patterns based on observed (categorical) indicators.14,35 Class enumeration was decided using statistical fit indices, classification diagnostics, interpretability, and utility.47 We started with a 1-class LCA model and added another class for each successive model (at a 4-class model in HUNT2 and HUNT3 and an 8-class model in HUNT4) and then compared model fit information. With this large sample population, Bayesian information criterion (BIC) was used to select the optimal number of latent classes,46,60 ie, lower values indicate superior fit, and checking for a reduction or plateauing in values for each added class.47,55 We further assessed log-likelihood values and likelihood-ratio χ2 statistics with P values to evaluate whether adding classes improved the model fit.46 The relative sizes of phenotypes in each class model were then compared, and the total average posterior probability was assessed for each model using 0.8 as threshold.60 We then compared the average posterior probability for each class with classification probabilities belonging to other classes to evaluate phenotype distinctiveness. Therefore, the final model for each survey was selected based on statistical measures and qualitative evaluation of the clinical meaningfulness of the resulting phenotypes.55 Descriptive demographics and health-related characteristics of the identified LCA phenotypes are presented as proportions or means with standard deviations.
All analyses were performed using Stata version 17.0 (StataCorp LLC).
2.4. EthicsThe Regional Committee for Ethics in Medical Research (ref no. 27216 REK Midt) approved this study, and all participants provided written informed consent.
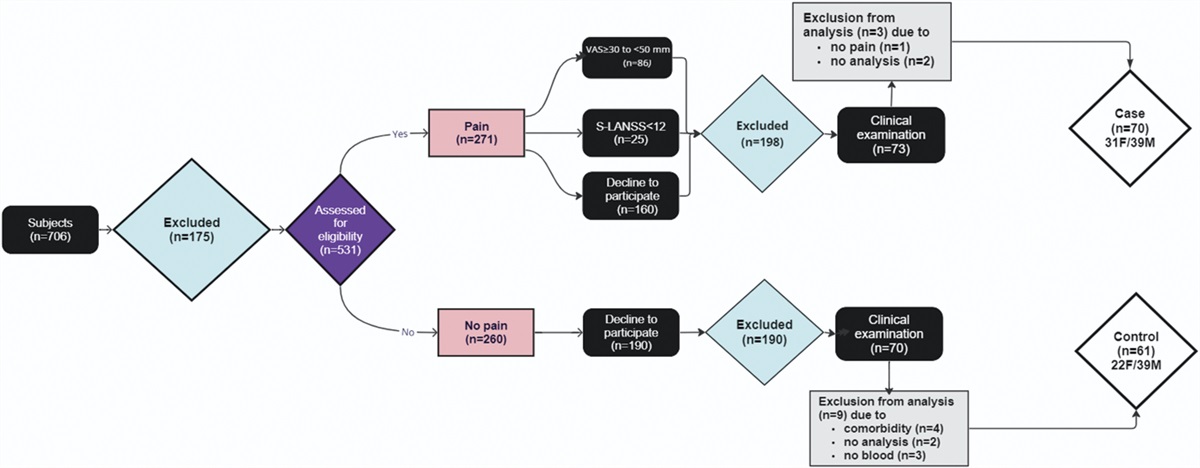
3. Results 3.1. ParticipantsAmong participants with information on persistent MSK pain and LBP in HUNT2, HUNT3, and HUNT4, 15,375 (24.5%) reported persistent LBP in HUNT2, 10,024 (25.7%) in HUNT3, and 10,647 (26.3%) in HUNT4. Co-occurring MSK pain alongside LBP was common and reported by 13,763 (89.6%) in HUNT2, 9081 (90.6%) in HUNT3, and 9750 (91.6%) in HUNT4, corresponding to persistent LBP only by 1612 (10.5%), 943 (9.4%), and 897 (8.4%) in HUNT2, HUNT3, and HUNT4, respectively (Fig. 1).
 Figure 1.:
Figure 1.: Flow and selection of participants with complete information on persistent musculoskeletal pain in HUNT2, HUNT3, and HUNT4. coMSK, co-occurring musculoskeletal; LBP, low back pain; MSK, musculoskeletal; MSKQ, Musculoskeletal Pain Questionnaire.
3.2. Prevalence and time trend of co-occurring persistent musculoskeletal pain alongside persistent low back painOverall, the prevalence of co-occurring MSK pain among participants with persistent LBP was very similar across the 3 surveys with co-occurring MSK pain in the neck (64%-65%), shoulders (62%-67%), and hips or thighs (53%-57%) being most common. Furthermore, in all 3 surveys, having co-occurring persistent MSK pain was more common than having persistent LBP only, ie, the prevalence of LBP only was ∼9% to 10% across surveys (Fig. 2 and Table S1, available at https://links.lww.com/PAIN/B874).
 Figure 2.:
Figure 2.: Age-standardized prevalence using the HUNT2 distribution of co-occurring persistent musculoskeletal pain among participants in HUNT2, HUNT3, and HUNT4 with persistent low back pain. LBP, low back pain; MSK, musculoskeletal.
3.3. Latent classes 3.3.1. Model selection and latent classes of co-occurring musculoskeletal pain in people with persistent low back painA 4-class LCA model was considered the model that best represented the data with sensible class distribution and clear phenotype distinctiveness, hence the preferred model for all 3 study samples (Table S2, available at https://links.lww.com/PAIN/B874). Across the 3 HUNT surveys, phenotype 1 has a high probability of LBP and low probability of co-occurring MSK pain and was labelled “LBP only.” Phenotype 2 has a high probability of LBP with neck and shoulder pain and was labelled “LBP with neck or shoulder pain.” Phenotype 3 has a high probability of LBP together with lower extremity pain (hips/thighs, knees, and ankles/feet), which in HUNT3 and HUNT4 also includes a higher probability of pain in wrists or hands (0.51 and 0.65, respectively) and hence labelled “LBP with lower extremity and wrists or hands pain.” Finally, phenotype 4 had a high probability of pain in all other sites additional to LBP and therefore labelled “LBP with multisite pain.” The weighted probability of belonging to each phenotype across the surveys was 35% for “LBP only,” 32% for “LBP with neck or shoulder pain,” 14% for “LBP with lower extremity or wrist or hand pain,” and 18% for “LBP with multisite pain” (Fig. 3 and Table 1).
 Figure 3.:
Figure 3.: Latent class phenotypes of persistent musculoskeletal pain co-occurring with persistent low back pain in HUNT2, HUNT3, and HUNT4. Shading indicates class-specific posterior probabilities for co-occurring musculoskeletal pain among people with persistent low back pain. Numbers indicate the relative size of latent classes and conditional item response probability.
Table 1 - Latent class-specific posterior probability of phenotypes of persistent musculoskeletal pain co-occurring with persistent low back pain in HUNT2, HUNT3, and HUNT4 in the final model. Musculoskeletal pain sites HUNT2 HUNT3 HUNT4 Pheno1 Pheno2 Pheno3 Pheno4 Pheno1 Pheno2 Pheno3 Pheno4 Pheno1 Pheno2 Pheno3 Pheno4 Low back 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 Upper back 0.09 0.38 0.14 0.72 0.11 0.47 0.15 0.77 0.11 0.44 0.13 0.67 Neck 0.13 0.94 0.25 0.95 0.17 0.93 0.38 0.97 0.20 0.97 0.33 0.97 Shoulders 0.15 0.94 0.33 1.00 0.17 0.85 0.44 1.00 0.20 0.86 0.42 0.97 Elbows 0.04 0.15 0.19 0.71 0.04 0.12 0.22 0.74 0.04 0.12 0.18 0.55 Wrists or hands 0.08 0.28 0.47 0.91 0.07 0.24 0.51 0.93 0.10 0.34 0.65 0.89 Hips or thighs 0.32 0.41 0.68 0.89 0.35 0.41 0.62 0.92 0.31 0.44 0.57 0.87 Knees 0.15 0.26 0.72 0.92 0.19 0.28 0.74 0.91 0.22 0.30 0.64 0.88 Ankles or feet 0.09 0.17 0.63 0.89 0.10 0.18 0.62 0.83 0.10 0.21 0.56 0.81 Relative size of latent classes 0.34 0.33 0.13 0.20 0.36 0.34 0.15 0.16 0.35 0.30 0.17 0.18 Average posterior probability 0.87 0.88 0.76 0.89 0.86 0.84 0.71 0.88 0.84 0.79 0.76 0.84 Total average posterior probability 0.87 0.83 0.81Numbers in bold indicate a probability of ≥0.50 for belonging to the specific phenotype.
Pheno, phenotype.
In the “LBP-only” phenotype, the female to male ratio is about equal, with more women in the “LBP with neck or shoulder pain” and “LBP with lower extremity and wrists or hands pain” phenotypes and a markedly higher proportion of women (75%-80%) in the “LBP with multisite pain” phenotype. The level of education in the Norwegian population increased during the 3 decades, and in HUNT4, the highest level of education is found for phenotype 2, “LBP with neck or shoulder pain.” Individuals in phenotype 3, “LBP with lower extremity pain and wrist or hand pain,” are slightly older than the other phenotypes. Body mass index is highest in phenotypes 3 and 4 in HUNT2 and HUNT3 and phenotypes 1 and 4 in HUNT4. People classified in phenotype 4, “LBP with multisite pain,” have more ill health, higher BMI, worse mental health, more sleep problems, more other long-term conditions, and poorer self-rated health (Table S3, available at https://links.lww.com/PAIN/B874).
4. DiscussionBoth the prevalence of co-occurring MSK pain among people with persistent LBP and phenotypic pain patterns have been stable in the adult Norwegian population over the past 3 decades. About 9 of 10 adults with persistent LBP experience co-occurring persistent MSK pain, most commonly in the neck, shoulders, and hips or thighs. These findings support that persistent LBP seldom presents itself as a single-site pain condition and that people can be classified into stable clinically meaningful pain phenotypes that may have relevance for stratified clinical care approaches.
Although LCA has been used in previous studies to model different patterns related to MSK pain, we are only aware of 2 previous population-based studies using this approach.27,54 Schmidt and Baumeister54 used pain in 13 body sites, including headache, stomach, face, and chest, as indicators in their LCA and identified 7 pain patterns. Their analysis was based on the prevalence of any multisite pain in the previous 7 days, whereas the present study used LBP as an index pain site alongside other persistent MSK pain. Hartvigsen et al.27 grouped the LCA according to primary pain sites and complaints during the previous 2 weeks. They identified 3 latent classes for LBP: LBP only, spinal pain, and a multisite pain class, which is similar to our study with the “LBP-only phenotype” and the “LBP with neck and shoulder pain,” also found in the previously mentioned systematic review reporting LBP co-occurring with axial pain48 and an expected finding.39 Although we did not confirm earlier reports of localized LBP being more frequent among men,13 we found that the proportion of women and individuals with poor overall health was markedly higher within the “LBP with multisite pain” phenotype, which is in line with previous studies.13,16,44,48 It is unclear why LBP with the lower extremity class was not detected in the study by Hartvigsen and co-authors; however, the smaller sample size (n = 584) could have masked this class.47 The phenotype “LBP with lower extremity and wrist or hand pain” may indicate a link to osteoarthritis which increases with age,33,58 as people classified to this phenotype were slightly older than in the other phenotypes and the wrist or hand involvement became more obvious from HUNT2 to HUNT3 and HUNT4. Hand osteoarthritis itself has been linked to higher age,24 whereas the onset of multijoint osteoarthritis is not necessarily associated with increasing age.5 Finney et al.21 reported that for people 45 years and older, pain in the hip, knee, foot, and hand was most prevalent and pointed toward a possible link to osteoarthritis. Similarly, another UK study on osteoarthritis found multiple involvements of lower extremity pain in the hip, knee, and/or foot among the elderly.50 In contrast to our analysis, these studies did not measure LBP as part of their pain clusters which is not uncommon in osteoarthritis research.
Our results have implications for future LBP and MSK prevalence studies as they should incorporate co-occurring pain sites for better precisions of estimates of the overall burden of MSK pain. In the Global Burden of Disease study (GBD), there is considerable uncertainty about the global estimates of LBP prevalence,57 and prevalence and burden are estimated based on prevalent single-site cases under noncommunicable diseases.59 The adjustment for comorbidity in the GBD assumes an independent distribution of comorbid conditions despite known correlations between certain disorders,32 and there is no consideration of co-occurring MSK pain when estimating the burden of LBP.
Knowing the extent of health problems is essential for understanding a population's healthcare needs. Hence, the findings of this study may be helpful for public health planning. In addition, public health promotion initiatives may use the knowledge of these consistent LBP phenotypes for long-term strategies focusing on secondary and tertiary prevention, suggested in the literature previously for LBP,1,4 while shifting beliefs in the population away from expecting a cure toward more realistic prospects of acceptance of MSK pain as an inevitable part of life.
Finally, guidelines for LBP management are targeted at LBP only, but with the high prevalence of co-occurring MSK pain, this single-site pain approach is too narrow. Musculoskeletal conditions share several similar characteristics, and a management approach based on standard prognostic factors across MSK conditions has been suggested.42,45 However, it could be that the prognostic factors affect LCA-derived LBP phenotypes differently and that different management strategies may be more beneficial. The different LBP phenotypes may be associated with a higher risk of lost work time, long-term sick leave, and disability pension that could be addressed. In future studies, a possible within-individual transition between LBP phenotypes and the characteristics of those who change should be investigated.
4.1. Strengths and limitationsA major strength of this study is the large population-based sample with a broad age range,3 raising the likelihood of a representative sample.23 Moreover, the consecutive surveys allowed us to evaluate the consistency of pain patterns at the population level over more than 20 years and through 3 decades. Previous studies have explored co-occurring MSK pain sites in more limited body regions or focused on the number of pain sites, whereas we had information on persistent co-occurring pain from 9 different body sites.
Our study has several limitations. First, although the sample is considered representative of Norway as a whole, there are no larger cities and a low immigrant proportion that may limit the generalizability of the results to other populations.3 Second, although socioeconomic inequalities in health are comparable to other northern European populations,3,38 attrition in HUNT3 and HUNT4 could be due to selective participation among people with high socioeconomic positions and better health3 (“healthy volunteer” effect) and thus underestimate MSK pain and LBP prevalence. Third, between HUNT2 and HUNT3, there was a change in the MSK pain questionnaire (ie, included a pain drawing and locations of the MSK questions were altered) and a decrease in the response rate from 70% in HUNT2 to 42% in HUNT3.25 Still, there may be a chance of reporting bias and overestimating MSK pain as HUNT3 participants reported more MSK pain than nonparticipants.38 Nevertheless, the fact that we included participants with data from 3 consecutive population-based surveys strengthens the confidence in our results. Fourth, the prevalence of MSK pain was derived from questionnaire data. However, the questionnaire data on LBP in HUNT4 did not differ substantially from diagnostic codes in the Norwegian Registry for Primary Health Care,3 and good agreement (kappa 0.63) was found between interview and questionnaire data for persistent MSK pain in HUNT3.25 Fifth, there is a potential for measurement error as people are asked to report MSK pain lasting for at least 3 consecutive months during the last year, which is longer than the recommended “past 4 weeks.”18 The recall of pain is also related to more than duration alone; for instance, current pain status can influence reporting of previous pain.10,51 Sixth, we only had information on the anatomical location of MSK pain and had no data on, for example, intensity, distress, and level of disability. Finally, we do not know the degree of potential overlap between pain sites, referred pain, neuropathic pain, and other underlying diseases.
5. ConclusionCo-occurring MSK pain alongside persistent LBP is very common, and our data show that the prevalence and patterns of co-occurring MSK pain have been consistent over 3 decades. In addition, 4 LCA-derived phenotypes of distinct MSK pain site patterns among people with persistent LBP seem stable over time in the general population.
Conflict of interest statementThe authors have no conflict of interest to declare.
Appendix A. Supplemental digital contentSupplemental digital content associated with this article can be found online at https://links.lww.com/PAIN/B874.
AcknowledgementsThis project is part of CKØ’s doctoral research. Her doctoral research fellowship position is at SDU and her fellowship is funded by the Danish Chiropractic Research Foundation, the research foundation ELiB in Norway, the European Centre for Chiropractic Excellence (ECCRE), and a Faculty Scholarship from the University of Southern Denmark.
Professor Werner Vach is acknowledged for his valuable contribution at the start of this project of introducing and explaining LCA in STATA, Afsaneh Mohammadnejad for her biostatistical input to the direct standardization of prevalence estimates, and Nikita Knarberg Doktor for her graphic drawings of the LCA-derived phenotypes.
Data availability statement: The data supporting the findings of this study are available from Professor Paul Jarle Mork ([email protected]) at the Norwegian University of Science and Technology (NTNU).
References [1]. Ardakani EM, Leboeuf-Yde C, Walker BF. Failure to define low back pain as a disease or an episode renders research on causality unsuitable: results of a systematic review. Chiropr Man Ther 2018;26:1. [2]. Artus M, Campbell P, Mallen CD, Dunn KM, van der Windt DAW. Generic prognostic factors for musculoskeletal pain in primary care: a systematic review. BMJ Open 2017;7:e012901. [3]. Åsvold BO, Langhammer A, Rehn TA, Kjelvik G, Grøntvedt TV, Sørgjerd EP, Fenstad JS, Heggland J, Holmen O, Stuifbergen MC, Vikjord SAA, Brumpton BM, Skjellegrind HK, Thingstad P, Sund ER, Selbæk G, Mork PJ, Rangul V, Hveem K, Næss M, Krokstad S. Cohort profile update: the HUNT study, Norway. Int J Epidemiol 2023;52:e80–91. [4]. Axén I, Leboeuf-Yde C. Trajectories of low back pain. Best Pract Res Clin Rheumatol 2013;27:601–12. [5]. Badley EM, Wilfong JM, Yip C, Millstone DB, Perruccio AV. The contribution of age and obesity to the number of painful joint sites in individuals reporting osteoarthritis: a population-based study. Rheumatol Oxf Engl 2020;59:3350–7. [6]. Bayattork M, Jakobsen MD, Sundstrup E, Seidi F, Bay H, Andersen LL. Musculoskeletal pain in multiple body sites and work ability in the general working population: cross-sectional study among 10,000 wage earners. Scand J Pain 2019;19:131–7. [7]. Bevan S. Economic impact of musculoskeletal disorders (MSDs) on work in Europe. Best Pract Res Clin Rheumatol 2015;29:356–73. [8]. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 2002;52:69–77. [9]. Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain—where to from here? Am J Public Health 2019;109:35–40. [10]. Brauer C, Thomsen JF, Loft IP, Mikkelsen S. Can we rely on retrospective pain assessments? Am J Epidemiol 2003;157:552–7. [11]. Briggs AM, Cross MJ, Hoy DG, Sànchez-Riera L, Blyth FM, Woolf AD, March L. Musculoskeletal health conditions represent a global threat to healthy aging: a report for the 2015 world health organization world report on ageing and health. Gerontologist 2016;56:S243–55. [12]. Chen S, Chen M, Wu X, Lin S, Tao C, Cao H, Shao Z, Xiao G. Global, regional and national burden of low back pain 1990-2019: a systematic analysis of the Global Burden of Disease study 2019. J Orthop Transl 2022;32:49–58. [13]. Coggon D, Ntani G, Walker-Bone K, Palmer KT, Felli VE, Harari R, Barrero LH, Felknor SA, Gimeno D, Cattrell A, Vargas-Prada S, Bonzini M, Solidaki E, Merisalu E, Habib RR, Sadeghian F, Kadir MM, Warnakulasuriya SS, Matsudaira K, Nyantumbu B, Sim MR, Harcombe H, Cox K, Sarquis LMM, Marziale MH, Harari F, Freire R, Harari N, Monroy MV, Quintana LA, Rojas M, Harris EC, Serra C, Martinez JM, Delclos G, Benavides FG, Carugno M, Ferrario MM, Pesatori AC, Chatzi L, Bitsios P, Kogevinas M, Oha K, Freimann T, Sadeghian A, Peiris-John RJ, Sathiakumar N, Wickremasinghe AR, Yoshimura N, Kelsall HL, Hoe VCW, Urquhart DM, Derrett S, McBride D, Herbison P, Gray A, Salazar Vega EJ. Epidemiological differences between localized and nonlocalized low back pain. Spine 2017;42:740–7. [14]. Collins LM, Lanza ST. Latent class and latent transition analysis: with applications in the social, behavioral, and health sciences. 1st ed. Hoboken, NJ: Wiley, 2009. [15]. Croft P. Picking targets in fog: the pluses and minuses of defining chronic widespread pain. PAIN 2016;157:514–5. [16]. Davies H, Crombie I, Macrae W. Where does it hurt? Describing the body locations of chronic pain. Eur J Pain Lond Engl 1998;2:69–80. [17]. Descatha A, Roquelaure Y, Chastang JF, Evanoff B, Melchior M, Mariot C, Ha C, Imbernon E, Goldberg M, Leclerc A. Validity of Nordic-style questionnaires in the surveillance of upper-limb work-related musculoskeletal disorders. Scand J Work Environ Health 2007;33:58–65. [18]. Dionne CE, Dunn KM, Croft PR, Nachemson AL, Buchbinder R, Walker BF, Wyatt M, Cassidy JD, Rossignol M, Leboeuf-Yde C, Hartvigsen J, Leino-Arjas P, Latza U, Reis S, Gil Del Real MT, Kovacs FM, Oberg B, Cedraschi C, Bouter LM, Koes BW, Picavet HSJ, van Tulder MW, Burton K, Foster NE, Macfarlane GJ, Thomas E, Underwood M, Waddell G, Shekelle P, Volinn E, Von Korff M. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine 2008;33:95–103. [19]. Dunn KM, Hestbaek L, Cassidy JD. Low back pain across the life course. Best Pract Res Clin Rheumatol 2013;27:591–600. [20]. de Fernandes RCP, Burdorf A. Associations of multisite pain with healthcare utilization, sickness absence and restrictions at work. Int Arch Occup Environ Health 2016;89:1039–46. [21]. Finney A, Dziedzic KS, Lewis M, Healey E. Multisite peripheral joint pain: a cross-sectional study of prevalence and impact on general health, quality of life, pain intensity and consultation behaviour. BMC Musculoskelet Disord 2017;18:535. [22]. Foster NE, Hill JC, Hay EM. Subgrouping patients with low back pain in primary care: are we getting any better at it? Man Ther 2011;16:3–8. [23]. Fox MP, Murray EJ, Lesko CR, Sealy-Jefferson S. On the need to revitalize descriptive epidemiology. Am J Epidemiol 2022;191:1174–9. [24]. Green DJ, Jordan KP, Protheroe J, van der Windt DA. Development of hand phenotypes and changes in hand pain and problems over time in older people. PAIN 2016;157:569–76. [25]. Hagen K, Linde M, Heuch I, Stovner LJ, Zwart J-A. Increasing prevalence of chronic musculoskeletal complaints. A large 11-year follow-up in the general population (HUNT 2 and 3). Pain Med 2011;12:1657–66. [26]. Hallman DM, Holtermann A, Björklund M, Gupta N, Nørregaard Rasmussen CD. Sick leave due to musculoskeletal pain: determinants of distinct trajectories over 1 year. Int Arch Occup Environ Health 2019;92:1099–108. [27]. Hartvigsen J, Davidsen M, Hestbaek L, Sogaard K, Roos EM. Patterns of musculoskeletal pain in the population: a latent class analysis using a nationally representative interviewer-based survey of 4817 Danes: patterns of musculoskeletal pain in the population. Eur J Pain 2013;17:452–60. [28]. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M, Buchbinder R, Hartvigsen J, Cherkin D, Foster NE, Maher CG, Underwood M, van Tulder M, Anema JR, Chou R, Cohen SP, Menezes Costa L, Croft P, Ferreira M, Ferreira PH, Fritz JM, Genevay S, Gross DP, Hancock MJ, Hoy D, Karppinen J, Koes BW, Kongsted A, Louw Q, Öberg B, Peul WC, Pransky G, Schoene M, Sieper J, Smeets RJ, Turner JA, Woolf A. What low back pain is and why we need to pay attention. Lancet 2018;391:2356–67. [29]. Hartvigsen J, Natvig B, Ferreira M. Is it all about a pain in the back? Best Pract Res Clin Rheumatol 2013;27:613–23. [30]. Hill JC, Garvin S, Bromley K, Saunders B, Kigozi J, Cooper V, Lewis M, Protheroe J, Wathall S, Chudyk A, Dunn KM, Birkinshaw H, Jowett S, Hay EM, van der Windt D, Mallen C, Foster NE. Risk-based stratified primary care for common musculoskeletal pain presentations (STarT MSK): a cluster-randomised, controlled trial. Lancet Rheumatol 2022;4:e591–e602. [31]. Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, Woolf A, Vos T, Buchbinder R. A systematic review of the global prevalence of low back pain. Arthritis Rheum 2012;64:2028–37. [32]. James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, Abdollahpour I, Abdulkader RS, Abebe Z, Abera SF, Abil OZ, Abraha HN, Abu-Raddad LJ, Abu-Rmeileh NME, Accrombessi MMK, Acharya D, Acharya P, Ackerman IN, Adamu AA, Adebayo OM, Adekanmbi V, Adetokunboh OO, Adib MG, Adsuar JC, Afanvi KA, Afarideh M, Afshin A, Agarwal G, Agesa KM, Aggarwal R, Aghayan SA, Agrawal S, Ahmadi A, Ahmadi M, Ahmadieh H, Ahmed MB, Aichour AN, Aichour I, Aichour MTE, Akinyemiju T, Akseer N, Al-Aly Z, Al-Eyadhy A, Al-Mekhlafi HM, Al-Raddadi RM, Alahdab F, Alam K, Alam T, Alashi A, Alavian SM, Alene KA, Alijanzadeh M, Alizadeh-Navaei R, Aljunid SM, Alkerwi A, Alla F, Allebeck P, Alouani MML, Altirkawi K, Alvis-Guzman N, Amare AT, Aminde LN, Ammar W, Amoako YA, Anber NH, Andrei CL, Androudi S, Animut MD, Anjomshoa M, Ansha MG, Antonio CAT, Anwari P, Arabloo J, Arauz A, Aremu O, Ariani F, Armoon B, Ärnlöv J, Arora A, Artaman A, Aryal KK, Asayesh H, Asghar RJ, Ataro Z, Atre SR, Ausloos M, Avila-Burgos L, Avokpaho EFGA, Awasthi A, Ayala Quintanilla BP, Ayer R, Azzopardi PS, Babazadeh A
留言 (0)