Female hypospadias is characterized by ectopic dorsal location of the external urethral opening, which is a rare congenital malformation. It is defined as female urethral opening on the anterior vaginal wall (proximal to the hymenal ring) anywhere between the introitus and the vaginal fornix [2]. Solov’ev classified this entity as follows: (a) vestibular (partial), (b) vestibulovaginal (subtotal) and (c) vaginal (total) types [6]. Knight H. M. reported clinical classification which consists of complete (type 1) and incomplete (type 2); urethral subtypes are IIa, short wide, and IIb, normal urethral diameter [7]. Three groups have been divided by Blum: (1) a longitudinal communication between the posterior urethral wall and the anterior vaginal wall; (2) a persistent urogenital sinus, where the vagina enters into the urethra but the hymen lies deep in the urogenital sinus; and (3) the urethra opening into the vagina proximal to a normal hymen [8]. Other differential diagnosis would be a cloaca or posterior cloaca. In a cloaca, the urogenital and rectum join to form a single canal and can be identified as a single perineal opening without a normal anus. In a posterior cloaca, the urogenital canal opens into the anterior wall of a normally located anorectum.
Hypospadias occurs in both sexes with a male gender preference. True pathoetiology of female hypospadias remains obscure [2]. Lower part of the urogenital sinus forms the common origin of the distal part of vagina and urethra. Abnormal development of these structures may result in female hypospadias [9]. Female hypospadias may coexist with other congenital urogenital septal defect, such as vaginal atresia, vaginal septum and bicornuate uterus [2]. Association with other anomalies like urethral duplication, 46XX disorders of sexual development (DSD), cloacal malformation and non-neurogenic neurogenic bladder has been reported [1, 10]. In this case report, patient has isolated female hypospadias without other congenital anomaly, which is very rare.
Yogesh suggested that description of female hypospadias should be used for the condition which is external urethral opening located in the lower one-third of the vagina. The entity which is external urethral orifice located in the upper two-thirds of vagina should designate as persistent urogenital sinus [10]. The urethral calibre will decide the prognostic significance. The shorten distance between the external urethral orifice and vaginal vestibule most likely to have normal calibre of urethra and less clinical complaints [10]. Narrower urethral lumen and higher location of the urethral orifice on the anterior vaginal wall, which is closer to the vaginal fornix, frequently result in urinary bladder outlet obstruction like acute urinary retention, hydroureteronephrosis, bladder distention, obstructive nephrolithiasis, and urinary tract infection [10]. Although our patient has short distance of urethral meatus from the perineum (2 mm), she was having severe symptoms of urinary bladder outflow obstruction complicated with acute renal failure. We postulate that this may be due to a urine filled hydrocolpos compressing on to the bladder neck.
Age of presentation may vary from paediatric age group to adults. The clinical presentation of female hypospadias is variable. Patients can be asymptomatic and incidentally discovered due to unsuccessful catheterization of urinary bladder. Patients may present with poor urine stream, post micturition incontinence, vaginal voiding, recurrent urinary tract infection (UTI), urethral syndrome and dyspareunia [2]. Postpartum stress incontinence, total incontinence after delivery, detrusor sphincter dyssynergia, and vaginal voiding which leads to urinary leakage secondary to frequent intense sphincter contraction as well as vaginal stone formation have been reported in patient with female hypospadias [2]. Sexual intercourse may worsen urethral syndrome and UTI. Hill et al. reported fibrosis secondary to urethral surgery or atrophic vaginitis as other acquired causes of female hypospadias in the adult age group [9].
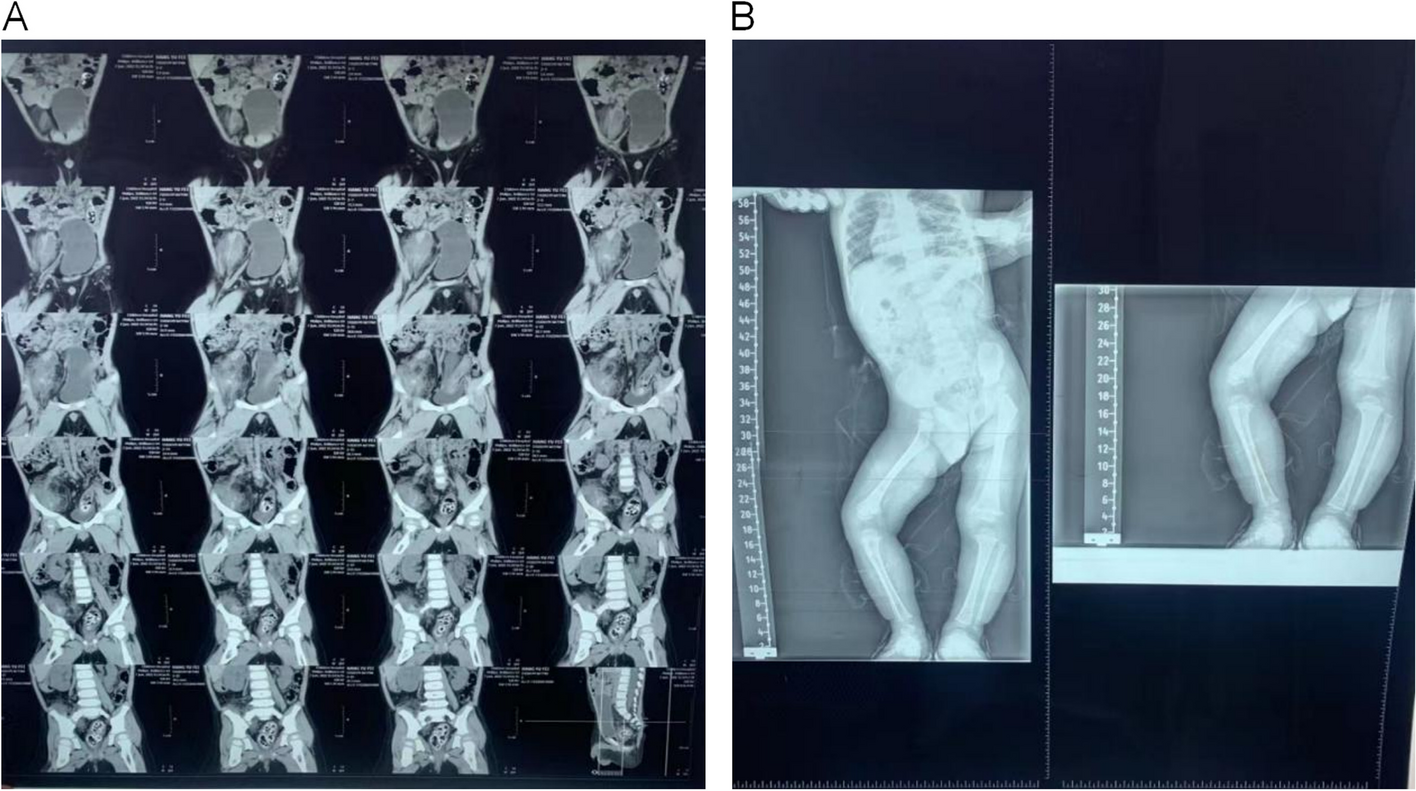
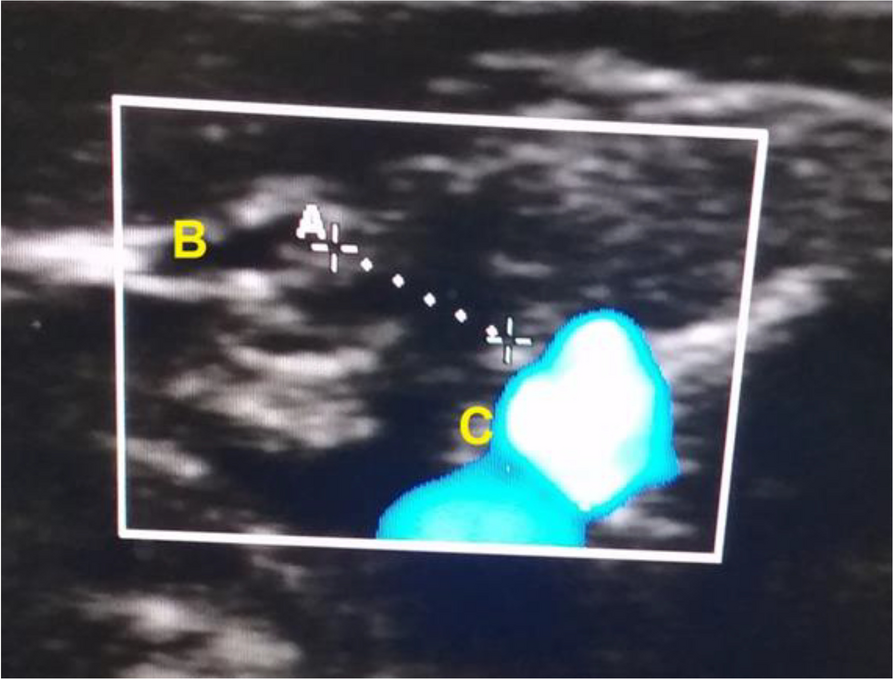
Antenatal scan may reveal normal study of KUB or mild and non-specific renal pelviectasis. Abdominal radiograph may show non-specific features and is not helpful for diagnosis of FH. Ultrasound abdomen should be the first diagnostic modality. Ultrasound may show bilateral hydroureteronephrosis with distended urinary bladder in FH patient represented with lower urinary tract obstruction. Concomitant urolithiasis, internal debris in pelvicalyceal system and thickened urinary bladder wall can occur together in view of prolonged urine stasis. The degree of obstructive uropathy is most likely related to calibre of the external urethral orifices. We proposed that larger urethral opening results to lesser degree of obstructive uropathy. In addition, ultrasound can help to assess other genital abnormality.
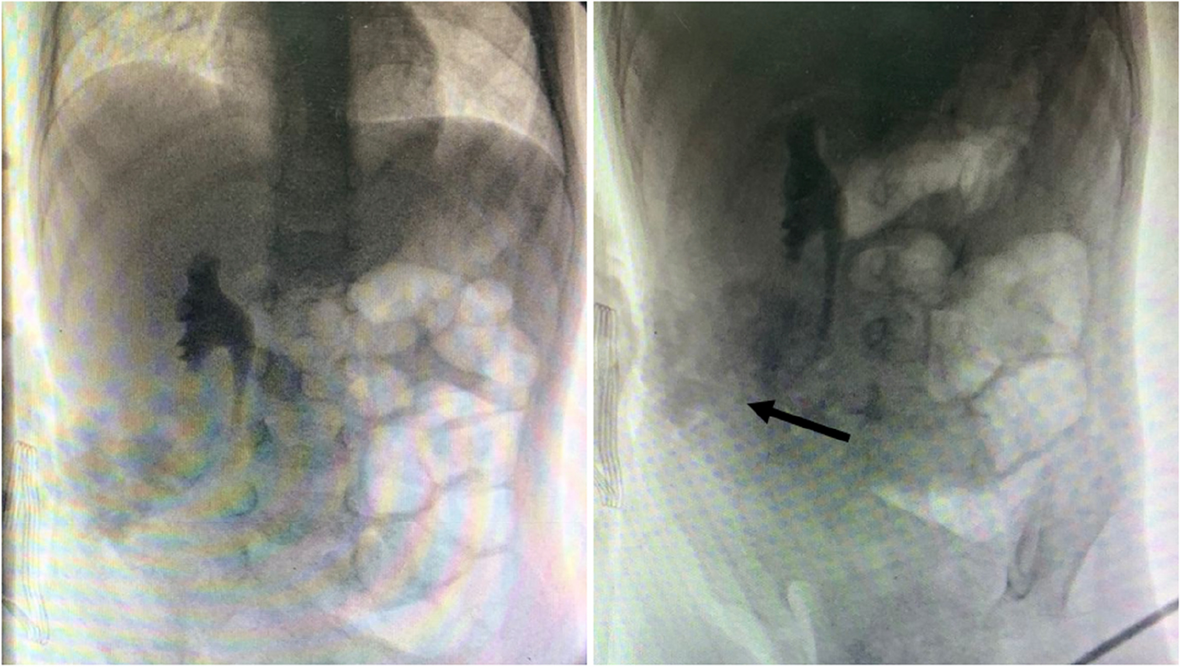
Antegrade cystogram via a suprapubic catheter could reveal an abnormal course of the urethra leading into the vagina. Genitogram may show opacification of the vagina without delineating the urethra. In the case of this patient, cystogram and genitogram failed to delineate the communication between the urinary bladder. Therefore, negative findings of cystogram and genitogram cannot totally exclude the diagnosis of FH. Computed tomography is less suitable to delineate the soft tissue plane between the pelvic organs. Furthermore, unnecessary radiation exposure should be avoided in children. MRI would be a more suitable modality to demonstrate the anatomy of the bladder, urethra and vagina. Advancement in 3D reconstruction technologies could enable clinicians to differentiate various urogenital anomalies [11]. MRI was not done in our patient due to financial constrains faced by her parents.
In this instance, a cystovaginoscopy was needed to map out the anatomy of her genitourinary system and come to a conclusion of FH.
There are various methods to repair female hypospadias. All variants of FH may be surgically corrected by transposition of the external opening of the urethra from the vagina to the perineum in sub clitoris location. Amilal Bhat et al. reported that vaginal flap urethroplasty with stone removal was performed in a case of FH with vaginal stones [2]. In case of aplasia or hypoplasia of urethra, tubularization of anterior vaginal strip to construct the urethra was reported [12]. Meatoplasty [13], construction of urethra from vaginal wall with buttock flap [14] or perineal flap [15] as well as pedicle flap of labial and bulbocavernosus muscle [10] could be other surgical methods. In our patient, due to the superficial location of the metal opening in relation to the perineum, an anterior meatoplasty was adequate to transpose the meatus to the surface and anteriorly. A longitudinal incision was on the anterior vaginal wall up to the meatal opening, and the incision was sutured transversely.



Comments (0)