
記住我
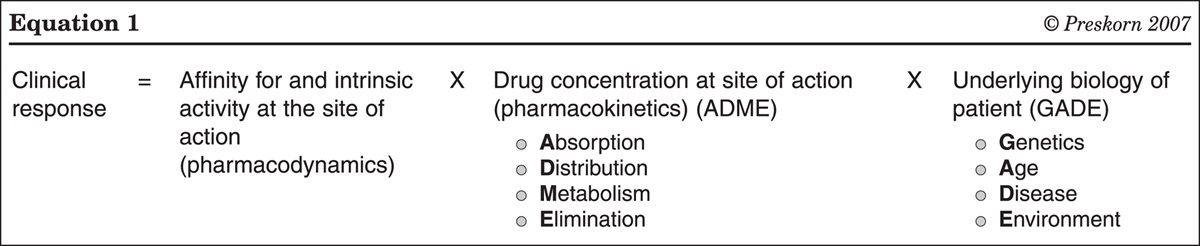

People with schizophrenia have higher premature mortality with a life expectancy of 15 to 20 years less than the general population,1,2 and the mortality gap does not seem to be narrowing over time.3,4 Although suicides and other unnatural causes are higher in this group, premature mortality is mainly attributed to preventable physical diseases and medical conditions, especially cardiovascular disease (CVD).1,2,5 One-third of all natural deaths occurring in people with schizophrenia are attributed to CVD.6
Several factors could be implicated in the etiology of CVD in schizophrenia: the disorder itself (which probably has a genetic basis), the side effects of medications, particularly antipsychotics, unhealthy lifestyle and risky behaviors, and poor primary and secondary prevention of CVD.7–15 Compared with the general population, people with schizophrenia are more likely to be overweight and to have diabetes mellitus, dyslipidemia, and metabolic syndrome.16–20
A wealth of information is available on treating the physical comorbidities of people with severe mental disorders and how to deal with medication side effects.9,21–24 Likewise, many behavioral and pharmacological interventions to improve cardiovascular risk factors (CVRFs) are available. However, despite favorable results for some variables, such as weight loss, improvement in glucose and lipid levels, and smoking cessation, an impact on overall cardiovascular risk (CVR) has not been reported.25–27 Evidence concerning multimodal interventions for CVD management is scarce.28 In a study carried out in England by Osborn et al29 that focused on improving cholesterol levels and CVR through promoting a healthy lifestyle and behavior and adherence to medication, no significant differences were observed between the groups after 12 months. In another multifaceted intervention conducted in Maryland by Daumit et al,30 with an intervention that included behavioral counseling, care coordination, and care management, the CVR score was significantly reduced after 18 months. A third research study carried out in Catalonia by Torralbas-Ortega et al31 aimed at promoting healthy habits and improving CVR through a short psychoeducational intervention found no significant improvements in the different variables studied after 1 year.
In this article, we describe a pilot clinical trial of a patient-centered multifactorial intervention aimed at improving CVR in people with schizophrenia.
METHODS Study Design and ParticipantsWe designed a 2-arm, parallel, randomized clinical trial at the Osona Mental Health Center belonging to the public health system in the province of Barcelona (Catalonia), which has a population of 163,702 inhabitants (according to the 2019 census). We included adults 18 years of age and older who had previously been diagnosed with schizophrenia by a psychiatrist according to the International Classification of Diseases (ICD-10), who had not had any health check-ups by the primary care team in the preceding 6 months, and who had at least 1 of the following poorly controlled CVRFs: hypertension, diabetes mellitus, hypercholesterolemia, and tobacco smoking. Target goals and pharmacological management were established for each CVRF according to the 2018 Program of Preventive Activities and Health Promotion of the Spanish Society of Family and Community Medicine (Table 1).32 We excluded people who were institutionalized, had suffered a recent psychiatric relapse (within 3 months before the intervention) with or without hospitalization, were diagnosed with intellectual disabilities or cognitive impairment, had an active substance use disorder or were in a methadone maintenance program, had a previous CVD (including heart failure, peripheral arterial disease, coronary artery disease, or stroke), or had a serious comorbid condition that limited life expectancy.
TABLE 1 - Target Goals and Pharmacological Management for CVRFs CVRF Target goals Pharmacological management Hypertension SBP <140 mm Hg and DBP <90 mm Hg ACEi and ARBs constitute the first line of treatment High BP was also identified: a device was offered to measure BP at home Another antihypertensive was added if BP target was not met Diabetes mellitus Hb1Ac <7% (7%-8% for people over 60 y of age). Metformin constitutes the first line of treatment Prediabetes was also detected if fasting glucose was 100-125 mg/dL and HbA1c ≥6.5% Another anti-diabetic was added if glycaemic target was not met Hypercholesterolemia LDL cholesterol according to CVR: Statins constitute the first line of treatment Very high: LDL <70 mg/dL Consider fibrates or ezetimibe if statins contraindicated High: LDL <100 mg/dL Moderate/low: LDL <115 mg/dL Tobacco smoking Smoking cessation Nicotine replacement therapy, bupropion, or varenicline Target goals and pharmacological management proposed by the Spanish Society of Family and Community Medicine.32ACEi indicates angiotensin-converting enzyme inhibitors; ARBs, angiotensin II receptor blockers; BP, blood pressure; CVR, cardiovascular risk; CVRF, cardiovascular risk factors; DBP, diastolic blood pressure; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure.
The recruitment period began in January 2020 and ended in October 2020. The study was stopped between March and May 2020 (both inclusive) due to the COVID-19 pandemic. The follow-up period was 6 months for all subjects.
Variables and InstrumentsWe collected data on sociodemographic, clinical, laboratory, and anthropometric variables (weight was measured in light clothing and without shoes), current tobacco smoking (self-reported), current psychopharmacological treatment and adherence according to the electronic dispensing register. Adherence was calculated by the proportion of days covered, which is the proportion of days a patient has medication available over 6 months from dispensing data records, considering an optimal value of at least 0.8.33 The prevalence of metabolic syndrome was calculated for each patient at baseline, defined as the presence of at least 3 of the following abnormal components: blood pressure (BP) >130/85 mm Hg, triglycerides >150 mg/dL, glycemia >100 mg/dL, HDL cholesterol <40 mg/dL for men and <50 mg/dL for women, and waist circumference >94.5 cm for men and >89.5 cm for women. Subjects who were receiving pharmacological treatment for hypertension, dyslipidemia, or impaired glucose tolerance/diabetes mellitus were considered to have the respective risk factor.34
The study assessed functionality, quality of life, and CVR with the instruments described below.
FunctionalityFunctionality was evaluated using the Functioning Assessment Short Test (FAST), which is a brief interview designed to be administered by a trained clinician. It consists of 24 items that are grouped into 6 areas: autonomy, work performance, cognitive functioning, finances, interpersonal relationships, and leisure. Each item is scored on a 4-point scale ranging from 0 (no difficulty) to 3 (high difficulty). Total scores are obtained by adding the scores for each item and range from 0 to 72 points. There are no cut-off points, and the higher the value, the greater the difficulty. In this study, we used the Spanish version of this instrument,35 which has recently been validated for its application in patients with schizophrenia, with good psychometric properties in terms of reliability and validity.36
Quality of LifeQuality of life was measured using the EuroQoL-5D Health Questionnaire (EQ-5D), which is a generic instrument in which subjects assess their state of health in 5 dimensions: mobility, personal care, daily activities, pain/discomfort, and anxiety/depression. The second part consists of a visual analogy scale represented by a vertical line of 20 cm in length graded from 0 (worst health state) to 100 (best health state). We used the Spanish version of this instrument (authorization registration number 39571).37
CVRCVR was estimated using the following 2 instruments.
The Framingham algorithm, which was calibrated for the Catalan population (Registre Gironí del Cor, Girona Heart Registry version 3.0, Framingham-REGICOR), estimates the 10-year probability of having a coronary event (eg, angina or myocardial infarction whether fatal or not) in adults 35 to 74 years of age. The risk is considered low if the score is <5%, moderate if the score is 5 to 9.9%, high if the score is 10% to 14.9%, and very high if the score is ≥15%.38–40
The QRISK3 algorithm, version 2018.0, estimates the 10-year probability of having a coronary event (heart attack or stroke) in adults 25 to 84 years of age. It includes specific parameters (eg, second-generation atypical antipsychotic use, diagnosis of a severe mental disorder) and the classical factors included in the Framingham tables. The risk is considered low if the score is <10%, moderate if the score is 10% to 20%, and high if the score is >20%.41
Procedure and VisitsAll subjects attended 3 face-to-face visits, which were carried out by a hospital pharmacist (PhD student) and a mental health nurse. Appointments took place in the outpatient consultation room with access to the institution’s medical history, the shared medical history of Catalonia, and electronic medication administration records.
First Visit (Recruitment and Screening)Written informed consent was obtained from all subjects, and the sociodemographic and physical variables were recorded. A blood test was scheduled, to be carried out at the hospital or at the primary care center (according to the subject’s preference).
If at least 1 poorly controlled CVRF was detected (hypertension, diabetes mellitus, hypercholesterolemia, or tobacco smoking, according to the target goals), the subject was randomized and assigned to the intervention group [Programa d’optimització del RISc CArdiovascular (in Catalan) (PRISCA) group] or to the control group (treatment-as-usual), using a computer-generated random sequence. Subjects whose CVRFs were well controlled were informed and excluded from the follow-up.
Second Visit (Baseline)This visit took place less than a month after the first visit for all subjects.
PRISCA group: participants from the intervention group received a patient-centered, multifactorial cardiovascular risk program according to the therapeutic plan designed for each subject by a multidisciplinary team of health professionals (2 family and community medical doctors, a mental health nurse, a clinical psychiatrist, a psychologist, and a hospital pharmacist). This group identified the CVRF to be improved (according to the target goals in Table 1) and proposed a patient-centered approach that might include different types of interventions. The initial management of the CVRFs was nonpharmacological. Pharmacological treatment was added or optimized if the nonpharmacological measures failed (ie, repeatedly obtaining poorly controlled CVRFs according to the cut-off points listed in Table 1, despite the implementation of hygienic-dietary measures) or if pharmacological treatment (eg, statins, antihypertensives or hypoglycemics) needed to be implemented early in the course of treatment in subjects with a high level of CVR. Any medication that was added to the therapeutic plan required an analysis of relevant interactions with current medication and medical and psychiatric comorbidities and monitoring for side effects and tolerance. The potential interventions that could be implemented are described below. Lifestyle interventions and behavioral counseling: promoting a healthy diet; promoting individualized regular daily physical activity; encouraging participants to quit smoking and report harmful effects, and offering strategies to beat their nicotine addiction. Medication: this was prescribed/optimized for poorly controlled CVRFs (hypertension, diabetes mellitus, hypercholesterolemia, and smoking tobacco) (Table 1), by the family and community physician. Optimization of psychotropic drugs: simplification of the pharmacological treatment, dose optimization, or switching to another drug with a better metabolic profile, with medication prescribed by the psychiatrist based on consensus with the patient’s referring psychiatrist. Monthly motivational intervention: this was carried out by the psychologist to improve adherence, to follow up on any side effects of medication, and to provide positive reinforcement to adhere to the therapeutic plan. The first session took place in a group, while the following sessions were individual (face-to-face or by telephone). Control group: participants from the control group were informed about the results of the screening and they were referred to treatment-as-usual by the primary care team. Final Visit (Closing)All participants in both the PRISCA and control groups were scheduled to attend a third visit 6 months after the baseline visit during which a number of physical, clinical, and analytical parameters were assessed.
All the information gathered at each visit was recorded in the patient’s medical history and shared with specialized and primary care professionals.
OutcomesThe main outcome was an assessment of the efficacy of the multifactorial intervention to improve the CVR score in people with schizophrenia, calculated as the change in CVR score at 6 months compared with the baseline score, using the Framingham-REGICOR function, in each of the study groups. We also calculated change compared with baseline in the secondary variables listed above at 6 months.
Statistical AnalysisA descriptive analysis of the data was carried out with the measures of central tendency (mean) and dispersion (SD) or mean and 95% CI for quantitative variables. Qualitative or categorical variables were described by absolute frequencies and percentages. The analysis was conducted using intention-to-treat principles. Bivariate analyses were performed according to a normal distribution of quantitative variables; the normality of the test was studied using the Kolmogorov-Smirnoff goodness adjustment test, and the quantitative variables were compared using the Student t test if the distribution was normal or the Mann-Whitney U test if it was not. The χ2 test was used to compare the qualitative variables. The level of statistical significance used for the hypothesis tests was 5%. The analysis was performed using the IBM SPSS Statistics program for Windows, version 26.
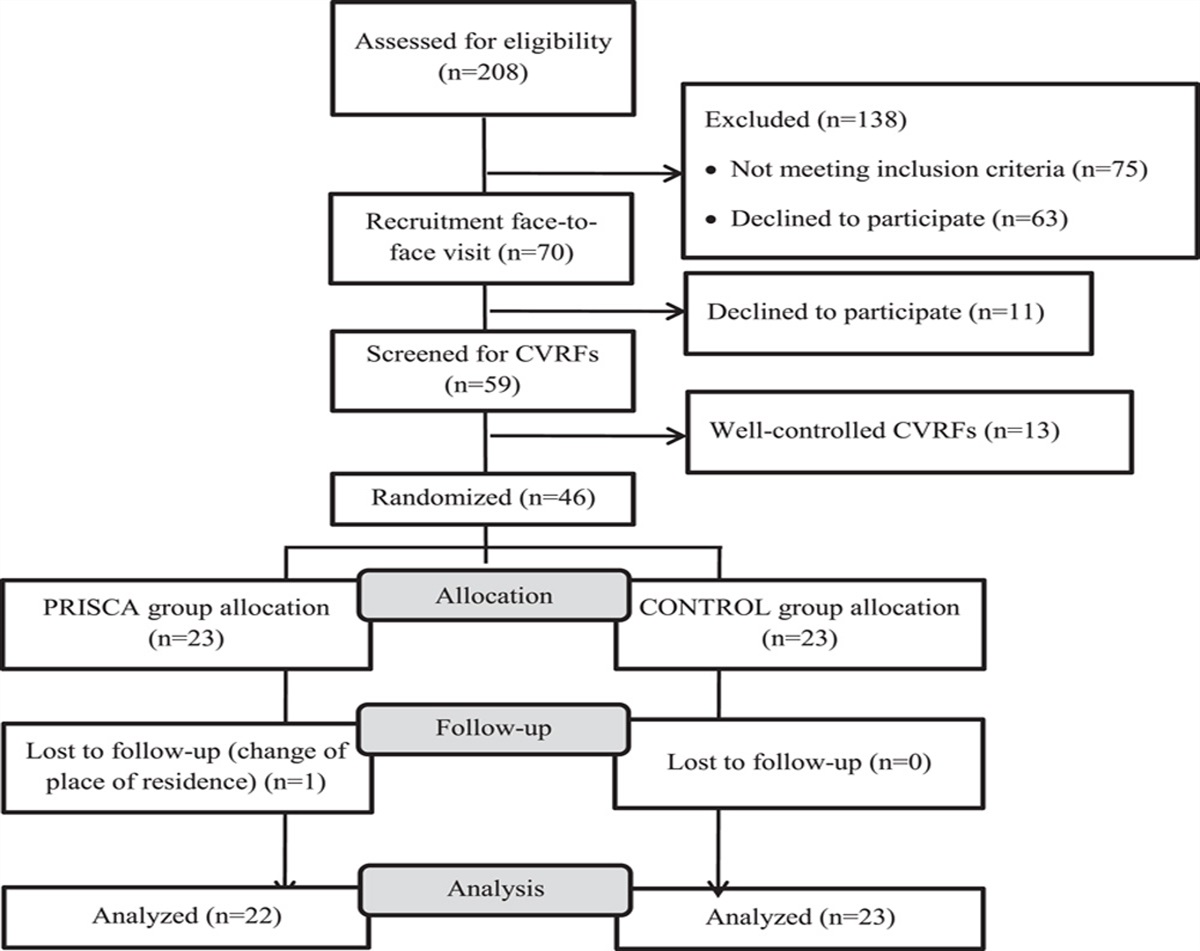
RESULTSOf the 208 potentially eligible patients who were assessed, 70 were invited to participate in the study. Fifty-nine patients were screened for CVRFs, 46 of whom (22.1% of the potentially eligible patients) had at least 1 poorly controlled CVRF and were included in the study and randomly assigned to the PRISCA group (n=23) or the control group (n=23). Figure 1 shows the CONSORT flow chart42 of participants. The mean age of the participants was 52.6 years (SD 11.1 y), 56.5% were men, with a mean body mass index of 30.8 kg/m2 (SD 5.0) and a mean REGICOR score of 4.5% (SD 3.2%). Hypercholesterolemia followed by tobacco smoking were the most prevalent poorly controlled CVRFs in the sample, and 93.5% of the participants were being treated with atypical antipsychotics, with over half receiving clozapine or olanzapine. The baseline characteristics of the participants are shown in Table 2.
 FIGURE 1:
FIGURE 1: Flow chart of participants. CVRFs indicates cardiovascular risk factors; PRISCA, Programa d’optimització del RISc Cardiovascular.
TABLE 2 - Baseline Characteristics of the Participants Total (N=46) PRISCA group (n=23) Control group (n=23) P Age, mean (SD), y 52.6 (11.1) 50.2 (11.3) 55.0 (10.7) 0.182 Male, % 56.5 52.2 60.9 0.337 Cohabitation, % Own family 28.3 30.4 26.1 0.780 Parents 50.0 43.5 56.5 Alone 17.4 21.7 13.0 In a group 4.3 4.3 4.4 Level of education, % None or primary 54.4 43.4 65.2 0.319 Secondary 15.2 17.4 13.0 After 16 y of age 30.4 39.1 21.8 Duration of schizophrenia, mean (SD), y 20.4 (11.1) 18.2 (10.9) 22.6 (11.0) 0.199 No. previous hospitalizations, mean (SD) 1.7 (1.7) 1.6 (1.0) 1.8 (2.2) 0.594 Physical measures, mean (SD) SBP, mm Hg 122.5 (15.5) 120.5 (14.6) 124.5 (16.4) 0.330 DBP, mm Hg 81.5 (9.7) 81.6 (8.8) 81.4 (10.7) 0.144 BMI, kg/m2 30.8 (5.0) 29.6 (3.9) 32.0 (5.7) 0.096 Waist circumference, cm 107.8 (11.2) 106.1 (10.4) 109.6 (12.0) 0.656 Laboratory measures, mean (SD) Glycemia, mg/dL 104.9 (32.7) 98.3 (14.6) 113.4 (45.0) 0.391 HbA1c, % 5.9 (1.6) 5.7 (0.7) 6.2 (2.2) 0.055 Total cholesterol, mg/dL 222.2 (32.5) 222.9 (32.4) 221.6 (33.2) 0.941 LDL cholesterol, mg/dL 137.9 (30.1) 135.6 (31.4) 140.1 (29.3) 0.586 HDL cholesterol, mg/dL 51.4 (13.9) 51.6 (13.3) 51.2 (17.8) 0.476 Triglycerides, mg/dL 177.4 (103.3) 178.7 (73.9) 176.0 (127.9) 0.344 GF, mL/min 81.2 (13.7) 83.0 (12.6) 79.4 (14.8) 0.567 CVR, mean (SD), % REGICOR* 4.5 (3.2) 4.5 (3.6) 4.5 (2.8) 0.457 QRISK3 10.8 (8.8) 8.7 (8.5) 12.9 (8.7) 0.921 Patients with MetS, % 44.4 39.1 50.0 0.333 Criteria for enrollment in the study, % Hypertension/High BP 21.7 17.4 26.1 0.361 DM/prediabetes 10.9 8.7 13.0 0.500 Hypercholesterolemia 84.8 82.6 87.0 0.500 Tobacco smoking 39.1 39.1 39.1 0.618 Psychotropic medication,† % Any atypical antipsychotic (oral or LAI) 93.5 95.7 91.3 0.600 Clozapine or olanzapine 58.7 65.2 52.2 0.275 Mood stabilizers 8.7 17.4 0.0 0.054 Antidepressants 32.6 39.1 26.1 0.265 Functionality, FAST, mean (SD) 16.3 (10.8) 13.2 (10.5) 19.4 (10.5) 0.051 Quality of life, VAS, mean (SD) 68.1 (15.1) 71.4 (15.2) 64.7 (14.5) 0.168*People between 35 and 74 years of age in PRISCA (n=19) and control (n=20) groups).
†Only medication with a proportion of days covered (PDC) of at least 0.8 were considered.
BMI indicates body mass index; BP, blood pressure; CVR, cardiovascular risk; DBP, diastolic blood pressure; DM, diabetes mellitus; FAST, functioning assessment short test (functionality); GF, glomerular filtrate; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LAI, long-acting injectable; LDL, low-density lipoprotein; MetS, metabolic syndrome; QRISK3,41 QRISK3 cardiovascular risk algorithm; REGICOR,38 REgistre GIroní del COR Framingham algorithm; SBP, systolic blood pressure; VAS, visual analogy scale (quality of life); SD, standard deviation.All of the subjects included in the PRISCA group (n=22) received information about promoting healthy lifestyles and behaviors. Specific medication for CVRFs (eg, antihypertensives, antidiabetic medications, or statins) was initiated or optimized in 72.7% (n=16) of the subjects, and psychotropic treatment was optimized in 13.6% (n=3) of the patients. Of the 22 subjects included in the PRISCA group, 72.7% (n=16) of the participants completed the motivational intervention, with a mean of 4.7 (0.9) sessions attended during the follow-up period. During the follow-up period, 56.5% of the participants in the control group and 47.8% in the intervention group (P=0.555), had visits with their primary care team, with a mean of 1.17 (1.47) and 0.52 (0.59) visits, respectively (P=0.058). None of the participants suffered any cardiovascular event during the study.
At the 6-month assessment, a statistically significant reduction in Framingham-REGICOR score (−0.96%; 95% CI: −1.60 to −0.32, P=0.011), which was equivalent to a relative risk reduction of 20.9%, was observed in the PRISCA group. Significant reductions in total cholesterol (−30.27 mg/dL; 95% CI: −51.78 to −8.77, P=0.008) and low-density lipoprotein (LDL) cholesterol (−27.14 mg/dL; 95% CI −46.28 to −8.00, P=0.008) were also observed in the PRISCA group (Table 3). In the control group, no statistically significant changes were observed in Framingham-REGICOR scores or cholesterol levels.
TABLE 3 - Outcomes at 6 Months PRISCA group Control group Baseline Change at 6 mo from baseline P Baseline Change at 6 mo from baseline P REGICOR (%)* 4.60 (3.57) −0.96 (−1.60 to −0.32) 0.011 4.46 (2.83) 0.21 (−0.47 to 0.89) 0.706 QRISK3 (%) 8.84 (8.68) −0.58 (−1.41 to 0.25) 0.159 12.90 (8.65) −0.22 (−1.00 to 0.56) 0.569 SBP (mm Hg) 121.41 (14.31) 1.36 (−4.07 to 6.80) 0.607 124.52 (16.36) 1.00 (−3.35 to 5.35) 0.638 DBP (mm Hg) 82.00 (8.80) −0.96 (−4.45 to 2.54) 0.576 81.35 (10.65) 1.44 (−1.47 to 4.34) 0.318 BMI (kg/m2) 29.61 (3.89) −0.08 (−0.79 to 0.62) 0.808 32.02 (5.65) −0.38 (−1.03 to 0.26) 0.233 Waist circumference (cm) 105.81 (9.99) −2.17 (−4.14 to −0.20) 0.033 109.86 (12.24) −0.14 (−1.62 to 1.33) 0.842 Glycemia (mg/dL) 97.81 (15.14) 7.43 (−0.02 to 14.87) 0.050 113.38 (45.00) −3.19 (−23.13 to 16.75) 0.742 HbA1c (%) 5.70 (0.70) −0.05 (−0.32 to 0.22) 0.689 6.19 (2.16) −0.45 (−1.18 to 0.29) 0.222 Total cholesterol (mg/dL) 220.64 (31.24) −30.27 (−51.78 to −8.77) 0.008 221.57 (33.20) 0.83 (−12.33 to 13.98) 0.898 LDL cholesterol (mg/dL) 134.55 (31.73) −27.14 (−46.28 to −8.00) 0.008 140.13 (29.29) −4.74 (−15.47 to 5.99) 0.369 HDL cholesterol (mg/dL) 49.59 (9.34) 2.77 (−0.79 to 6.33) 0.120 51.22 (14.78) 2.83 (−0.24 to 5.89) 0.069 Triglycerides (mg/dL) 182.95 (72.74) −29.55 (−60.87 to 1.78) 0.063 175.96 (127.91) 52.96 (8.88 to 97.03) 0.021 GF (mL/min) 81.86 (12.49) 3.52 (−2.31 to 9.36) 0.222 79.39 (14.75) 4.70 (−0.054 to 9.48) 0.054 FAST (functionality) 13.23 (10.51) −2.05 (−4.31 to 0.21) 0.073 19.03 (10.52) −0.91 (−4.16 to 2.34) 0.567 VAS (quality of life) 71.57 (15.58) 4.14 (−1.68 to 9.96) 0.153 64.69 (14.48) −4.48 (−12.43 to 3.47) 0.255Values are presented as mean and SD. The change is expressed as the difference in means at 6 months from baseline and presented as a 95% CI.
*People between 35 and 75 years of age in the PRISCA (n=19) and CONTROL (n=20) groups.
BMI indicates body mass index; DBP, diastolic blood pressure; FAST, functioning assessment short test (functionality); GF, glomerular filtrate; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; REGICOR,38 REgistre GIroní del COR Framingham algorithm; SBP, systolic blood pressure; VAS, visual analogy scale (quality of life).After 6 months, 54.5% of participants in the PRISCA group showed a reduction in their number of poorly controlled CVRFs from baseline, 36.4% had no change, and 9.1% had an increase in the number of poorly controlled CVRFs. The distribution in the control group was 17.4%, 73.9%, and 8.7%, respectively. Statistically significant differences were observed between the PRISCA and control groups (χ2=7.565, P<0.05) (Fig. 2).
 FIGURE 2:
FIGURE 2: Change in the number of poorly controlled cardiovascular risk factors after the intervention, by groups. The figure represents the change in the number of poorly controlled CVRFs in the PRISCA and control groups, at 6 months compared with baseline. “Better” means a reduction in the number of poorly controlled CVRFs; “equal” means the same number of poorly controlled CVRFs as at baseline; and “worse” means an increase in the number of poorly controlled CVRFs compared with baseline. Statistically significant differences were observed between the PRISCA and control groups (χ2 = 7.565, P < 0.05). CVRFs indicates cardiovascular risk factors; PRISCA, Programa d’optimització del RISc CArdiovascular.
DISCUSSION Overview of Key FindingsTo the best of our knowledge, the PRISCA study described here involved one of the few multimodal interventions conducted in people with schizophrenia in which CVR was used as an outcome. We found that a patient-centered, multifactorial, and multidisciplinary intervention reduced CVR in subjects with schizophrenia after 6 months, with the improvement equivalent to a relative risk reduction of 20.9%. This improvement in CVR was mainly due to the reduction in total and LDL cholesterol levels, achieved through improved dietary habits and the prescription, where appropriate, of statins. This was a significant reduction in LDL cholesterol which, according to the evidence, leads to a reduction in the risk of major cardiovascular events, even in young and low-risk people.43 This result was also relevant given that the participants included in the study had not had any health check-ups by the primary care team in the previous 6 months. This implies a proactive detection of CVRFs in a population that does not usually consult primary care services. Cholesterol reduction secondary to statin use may explain part of the results. However, the study design does not allow us to isolate the contribution of other factors such as diet, physical activity, and optimization of psychotropic drugs. Consequently, it is questionable whether the introduction of a lipid-lowering treatment could have a similar effect on the proposed intervention per se.
Given the lack of consensus on CVR prediction models in schizophrenia, testing of QRISK3 function appeared to be a more realistic option as it incorporated parameters specific to this population group, such as the presence of schizophrenia as a severe mental disorder or the use of second-generation antipsychotics.7,41,44 Using this estimation function, no significant differences were observed at 6 months compared with baseline in either of the study groups. The small sample size and the short follow-up period probably conditioned this result. Some authors suggest conventional estimators, like REGICOR, are not suitable for estimating the true risk in this population,44,45 which could lead to inadequate screening and treatment. Thus, it would be interesting to have a validated, consensual, and systematized estimation function in clinical practice that would facilitate risk stratification, decision-making, and early management21,45 in people with severe mental disorders.
The magnitude of CVR observed in our study using the Framingham-REGICOR function was comparable to that observed in the study of a multifaceted intervention by Daumit et al.30 Those researchers found a reduction of relative risk of 12.7% using the Framingham function after 18 months in people with serious mental illness (59.1% of whom were diagnosed with schizophrenia) using behavioral counseling and coordination with mental health staff to encourage the achievement of health goals. In the PRISCA intervention, having a multidisciplinary group that included both primary care physicians and mental health professionals was probably key in optimizing CVR through screening and management of CVRF in people with schizophrenia. On the other hand, in the PRISCA study, statins were prescribed when a
留言 (0)