
Remember me
The 1-year follow-up has been part of the standard program offered to patients after ACLR at the section for sports traumatology, department of orthopedic surgery at Copenhagen University Hospital Bispebjerg since 2007, and the regional ethical committee stated that ethical permission was not required for this study (ref. nr. F-23055524). The patients gave written consent to have their data registered, and permission to store data for this study was obtained. The study was performed according to the STROBE checklist for cohort studies.
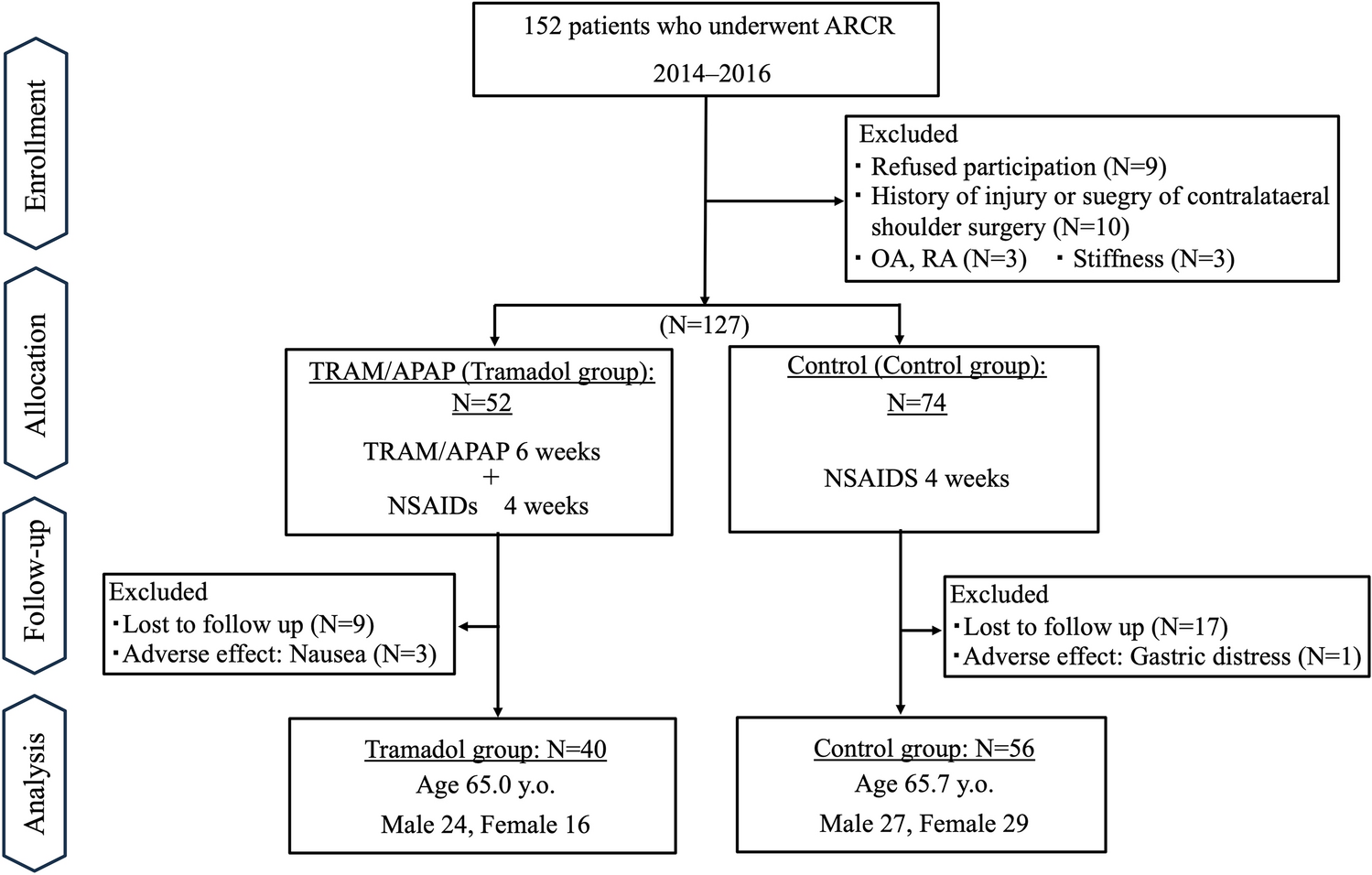
Between January 1, 2019, and December 31, 2021, 190 patients had a primary ACLR (patients with revision ACLR, multiple ligament injuries or pathology of the contralateral knee (including ACLR) were not included). Of these, 151 attended the 1-year follow-up, and they were included in this study (Fig. 1). Meniscal pathology or cartilage defects was not an exclusion criteria. All patients were seen by a physical therapist before discharge after the operation and were given a standard rehabilitation program. Almost all patients attended supervised rehabilitation, either free of charge in a municipal physiotherapy clinic (typically for three months) or with a physical therapist affiliated with a sports club or to a private clinic. Braces were not used, except in cases with meniscal refixation, in which case full weight bearing was allowed but with flexion restricted to 40° for 2 weeks and to 90° for the subsequent 2 weeks.
Fig. 1
The study flowchart summarizing screening, inclusion and exclusion of the patients
Surgical techniquesFor all ACLRs, the drill tunnels were positioned at the anatomical insertion sites of ACL. Drilling of the femoral tunnel was through the anteromedial portal, inside-out, and of the tibial portal outside-in. Standard grafts were doubled hamstring tendons, and they were fixed by EndoButton (Smith & Nephew) on the femur and by Intrafix with a sheath (DePuy) on tibia. Patellar tendon grafts and quadriceps tendon grafts were fixed with Peek screws (Arthrex), and iliotibal tract grafts were fixed with TightRope (Arthrex) at tibia and a peek screw on femur. The grafts that had been used are listed in Table 1. Meniscal lesions were either resected or repaired using FastFix (Smith & Nephew) (Table 2). In this cohort two patients had cartilage defects (one patient with a defect in the medial femoral cartilage and one in the lateral femoral cartilage), and both were left untouched.
Table 1 Grafts used for reconstruction of the anterior cruciate ligament in the 151 patients included in the studyTable 2 Details of meniscal injuries and their treatment in 151 patients who had a reconstruction of the anterior cruciate ligamentClinical evaluationInformation was prospectively registered: Preoperative data on gender, age, results of manual Lachman, drawer- and pivot shift tests, instrumented stability by Rolimeter in 30° of knee flexion, and results of the dial test and MCL/LCL stability tests—all stability tests were performed in both knees. There was peroperative information on concomitant injuries and their treatment. The 1-year follow-up was performed by a physical therapist (one of three) with special experience in knee ligament injury and functional testing. Lachman-, drawer- and pivot shift tests and instrumented stability measurements were performed.
Laxity was measured in mm by the Rolimeter as described by Ganko [9] with the knee in 30° flexion and the patient in the supine position. With the patient fully relaxed, the tibia was pulled anteriorly as far as possible with maximal power. The measurement was performed three times, and the last result was registered. Lachman stability was tested as described in [31], anterior and posterior drawer as in [25], pivot shift as in [8], side-stability as in [24] and dial test as in [24].
Patient-reported outcome measures (PROMs)At 1-year follow-up, patients completed four patient-reported outcome measures (PROMs): the Lysholm score, the Subjective IKDC score, the Knee Numeric-Entity Evaluation Score (KNEES-ACL) and the Knee injury and Osteoarthritis Outcome Score (KOOS). Activity was assessed by the Tegner Score. Anchor questions were answered: satisfaction with the ACLR, indicated on a 3-point scale (very satisfied, satisfied, not satisfied), and whether the patient would prefer the same treatment if the postoperative result had been known preoperatively (on a 3-point scale: yes, perhaps, no).
The IKDC questionnaire was published in 2001 [16] and it was intended for patients with a variety of knee conditions. It was developed by experts without the involvement of patients, and therefore it has no proven content validity [12, 13]. KOOS was published in 1998 [29] and it was intended for patients with knee injury and osteoarthritis. It is an aggregation of The Western Ontario and McMaster Universities’ Arthritis Index (WOMAC) [3], consisting of 3 domains with 33 items, plus two domains with 9 items developed through interviews with patients with ACL injury or meniscal conditions. WOMAC was developed for patients with end-stage osteoarthritis of the hip or knee and with the involvement of such patients. KOOS has no proven content validity for patients with ACL injury [12, 13]. Also, it has a low degree of construct validity (measurement properties) for patients with ACL injury when evaluated with item response theory models [4, 13, 19]. The Lysholm score was published in 1982 and updated in 1985, and it intended to evaluate knee ligament surgery [30]. It was developed without patient involvement and has no proven content validity [13]. KNEES-ACL was published in 2013 and intended for patients with ACL injury [5]. It was developed by involvement of patients with ACL injury and has good content validity [12, 13]. Construct validity evaluated with item response theory models is good [13].
Functional performance testsAll tests were conducted 1 year after the operation by a group of trained physiotherapists who had not been involved in the patients’ surgery. The test battery included single leg hop test (SH), triple hop test (TH), 6-m timed hop test (6 m-timed) and cross-over hop test (COH), as described by Noyes et al. [26]. The intra- and inter-rater reliability of these tests is moderate to excellent [18]. The test procedures are described in detail by Warming et al. [32].
After 5 min of warming up, typically on an exercise bike, followed by 2 min of stretching, the patients made three practice trials prior to each test with adequate rest periods between trials to minimize the effects of fatigue. The practice trials allowed the patients to familiarize themselves with the tests and minimized the learning effects. The best trial score of three jumps was utilized for data analysis, indicating the patient’s maximal performance. All tests had to be performed without losing balance and with a secure landing.
During the single-leg hop the patients stood on one limb, hopped as far forward as possible, and landed on the same limb. The distance was recorded with a tape measure, fixed to the floor. As the subject landed, an investigator recorded the distance from the starting position to the heel strike. Each limb was tested three times. To calculate the limb symmetry index, the best result for the involved limb was divided by the best result for the non-involved limb, and the result was multiplied by 100. A similar procedure was conducted with the triple hop test (to jump as far as possible on a single leg three consecutive times), and the longest distance for each leg was used to calculate limb symmetry.
The single-leg timed hop test was performed over a distance of 6 m with the patients jumping as fast as possible on a single leg. The patients were encouraged to use large, forceful one-legged hopping motions to propel their body forward. The best time of three attempts was chosen for each limb and used for limb symmetry calculation.
The single-leg cross-over triple hop for distance test was performed on a test ground with a 15-cm broad, 6 m long marking strip on the floor. Each patient hopped three consecutive times on one foot, crossing the marking strip during each hop. Each subject was encouraged to jump as far forward as possible during each hop. The total hop distance was measured for each of the three trials, and the best result was used for the calculation of limb symmetry.
After the calculation of the limb symmetry indexes for each of the four hop tests, a composite symmetry index was calculated for the individual patients as the mean of the four indexes.
Statistical analysisA comparison was evaluated through Pearson correlations and a 95% confidence interval (CI) computed based on Fisher’s z-transformation. The KOOS and KNEES-ACL domain scores were calculated as raw scores. The strength of the correlations was interpreted as: 0.00–0.30 negligible, 0.30–0.50 low, 0.50–0.70 moderate, 0.70–0.90 high and 0.90–1.00 very high. With α = 0.05, β = 0.20 and the lowest correlation we regarded as relevant being 0.25 (high in the negligible category and meaning that 6.25% of the changes in one outcome can explain changes in the other outcome) we needed 123 patients in the study [15].
Calculations were performed in SAS.
To evaluate whether the presence of meniscal injury affected the correlations, the two groups [no meniscal pathology (n = 77) and meniscal pathology (n = 74)] were also analysed separately.
Comments (0)