
Remember me

We conducted a proof-of concept, prospective, randomized, double-blind, placebo-controlled, multicenter, dose-ranging study of 2 doses of suramin (10 mg/kg and 20 mg/kg) versus placebo in 52 boys with ASD, ages 4–17 years. The primary objectives of the study were the safety, tolerability, and efficacy of suramin in children with autism. Investigators confirmed the diagnosis and that each subject had at least moderate ASD symptoms, based on the ADOS-2 comparison score.
The Aberrant Behavior Checklist (ABC) is an informant rating scale that is widely used in pharmacological research; it has well-established reliability, validity, and drug sensitivity [26,27,28]. Its five subscales are 1 (irritability, agitation, crying); 2 (lethargy/social withdrawal), 3 (stereotypic behavior), 4 (hyperactivity/noncompliance); and 5 (inappropriate speech). Prospectively, we designated improvements in the sum of ABC subscales 2, 3, and 5, the ABC-Core, as our primary endpoint. The ABC-Core has not previously been used as a singular outcome variable, although the three separate subscales have been used extensively in drug research. Subscales 1 and 4 were not included in ABC-Core as these subscales did not assess core ASD symptoms, but they were analyzed separately.
Secondary endpoints included ABC-Total Score (including all 5 subscales), Clinical Global Impression of Improvement (CGI-I) adapted for autism, Autism Treatment Evaluation Checklist (ATEC), and Expressive One Word Picture Vocabulary Test (EOWPVT). All primary and secondary endpoints were prespecified in the statistical analysis plan. A post hoc analysis was conducted with the ABC-Core evaluating the impact of age and severity of illness at baseline on efficacy outcomes.
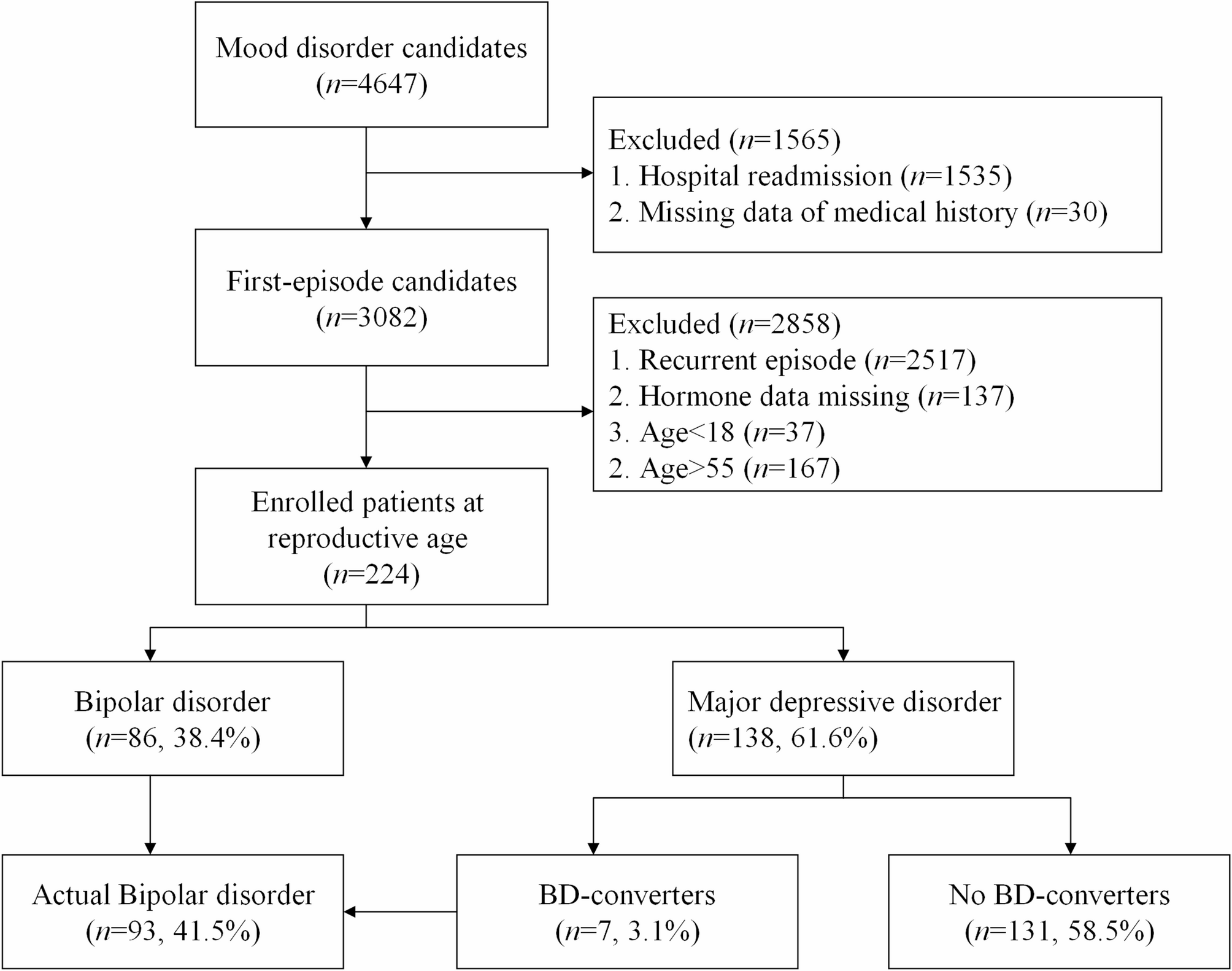
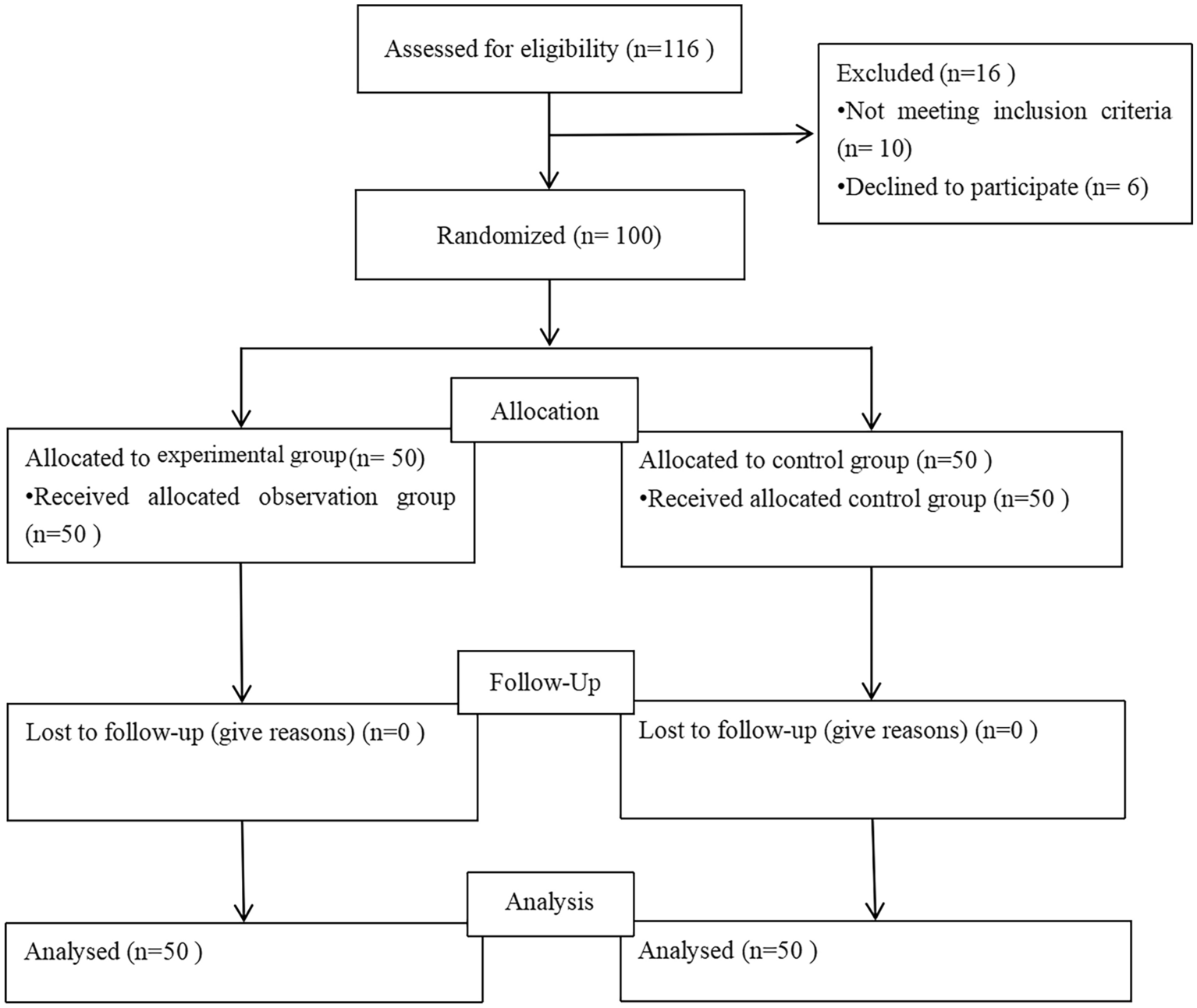
There were 3 intravenous infusion treatment groups: suramin 20 mg/kg, suramin 10 mg/kg, and placebo. Treatment was administered at baseline, week 4, and week 8. The higher dose was chosen based on the previous Naviaux et al., 2017 study. This study used a single dose of 20 mg/kg, which was well tolerated, and some efficacy benefits were observed in 5 participants with ASD. A lower dose of 10 mg/kg was also chosen to determine if a lower dose would show similar efficacy and potentially better safety and tolerability. Total duration of the study was 14 weeks. The details of the patient flow and study design are shown in Figs. 1 and 2, respectively. The study was conducted at 6 sites in South Africa, where suramin is a registered medicine and was approved by the South African Health Products Regulatory Authority and the National Health Research Ethics Council on February 19, 2019 (Application 3DOH-27–0419-6116). The ClinicalTrials.Gov ID is NCT06058962. Each of these sites were outpatient treatment centers and subjects were recruited through local advertising. Each family member or caregiver was given a small stipend to cover out of pocket expenses (e.g., transportation, meals) for each study visit. The amount of these stipends was reviewed and approved by local ethics committees. The study was conducted according to the ethical principles of the Declaration of Helsinki, International Conference on Harmonization guidelines for Good Clinical Practices (GCP).
Fig. 1 Fig. 2
Fig. 2
Inclusion criteria included males aged 4 to 17 years with a diagnosis of ASD by Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V), ADOS-2 comparison scores in the moderate and high level as evaluated on the ADOS-2, and stable treatment intervention for ≥ 2 months. Participants agreed to remain on a stable treatment intervention throughout the study and participants on methylphenidate and risperidone or similar medication agreed to maintain a stable dose during the study.
Exclusion criteria included psychiatric hospitalization within the previous 2 months, an acute medical problem, Rett syndrome, microcephaly, tuberous sclerosis, neurofibromatosis, epilepsy or children with known syndromic forms of ASD caused by DNA mutation or chromosomal copy number variation. Other exclusion criteria included any clinically significant liver, kidney, or adrenal disease, serious acute condition, plans to start a new drug, diet, or behavioral intervention during the study, weight under the 5th percentile for age, plasma creatinine above normal for age and weight according to the laboratory reference ranges, liver enzyme alanine aminotransferase (ALT) or aspartate aminotransferase (AST) ≥ 1.5-fold above the upper limit of normal, and known intolerance to suramin or other antipurinergic drugs.
The study was conducted between May 2019 and December 2020. There was a pause of approximately 6 months during the COVID-19 pandemic as clinics closed and families were unwilling to come in for clinical visits. This resulted in five participants dropping out of the study (Fig. 1). The sample size was increased to 52 (48 originally planned) to replace these early withdrawal participants.
Statistical analysisStatistical analysis was governed by a Statistical Analysis Plan (SAP), which was amended on 26 January 2020 to accommodate delays in study visits due to COVID-19. The Intention-to-Treat (ITT) population, which was the primary efficacy analysis population, consisted of all randomized participants. The sample size of 52 randomized 1:1:1 was chosen to yield 80% power to detect a difference of 2 units between treatment arms with a significance level of 0.05. This calculation was based on a between-participant standard deviation based on the ABC – Total Score of about 2.3 in suramin and 4.3 in placebo as reported by Naviaux et al., 2017 [25].
After signing the informed consent and assent forms, the participants were allocated a 3-digit participant number that was used to identify them throughout the study. In each center, participant numbers were assigned in sequential order. The site requested the central randomizer to randomize the participant. Each participant was assigned to one of the three double-blind treatment groups for the duration of the study. The randomization was also stratified according to Age, ADOS-2 and Non-verbal Intelligence Quotient (NVIQ) as assessed by the Leiter International Performance Scale, 3rd Edition (Leiter-3). Participants were randomized to one of three double-blind treatment groups, i.e., Arm A (10 mg/kg suramin) or Arm B (20 mg/kg suramin) or Arm C (placebo) in a targeted 1:1:1 ratio, as per the randomization schedule and stratification plan. The stratification plan was to match patients by age (< 7 vs ≥ 7), ADOS-2 comparison scores (≤ 8.5 vs > 8.5) and NVIQ (≤ 80 vs > 80).
For efficacy modeling, the SAP approach for missing data would focus on the ABC-Core and CGI outcomes for participants missing Week 14 data resulting from withdrawal, drop-out, loss-to-follow-up, or missed visits. Because of COVID quarantine, the planned approach for the ABC-Core was to apply a wide window to the last two visits, and to use a single imputation. The CGI-I was recorded at each timepoint relative to the previous one; the sum of all timepoints represents the week 7 change from baseline. The approach for CGI-I missing data was to use all available timepoint data, which is akin to a last-observation-carried-forward (LOCF) approach and assumes no additional changes after the last timepoint for non-completers. An analysis of variance (ANOVA) used changes at Week 14 compared to baseline for ABC-Core and Week 14 scaled scores (as described above) for CGI-I as responses, with categorical treatment group and baseline age, ADOS-2, and non-verbal IQ (NVIQ) (all continuous) as covariates. P-values for ABC-Core and CGI analyses used Dunnett’s method for multiple comparisons. As this study was aimed at selecting viable outcomes for future studies, there were no other adjustments for multiple outcomes.
Pharmacokinetic analysisPharmacokinetic samples were obtained at seven time points: Baseline (before and 1 h after infusion), day 28 (before and 1 h after infusion), day 56 (before and 1 h after infusion), and at the end of the study (day 98). PK plasma samples with lithium heparinate as anticoagulant were collected and stored at ~ − 20 °C and analyzed after the study by Farmovs Integrated Research Solutions in Bloemfontein, South Africa. Extraction from the biological matrix was performed with a protein precipitation technique, liquid chromatography with tandem mass spectrometry detection (LC–MS/MS) Sciex API4000. The software used Watson LIMS™ software version 7.4.2 and Analyst® software version 1.6.2.
Comments (0)