
記住我

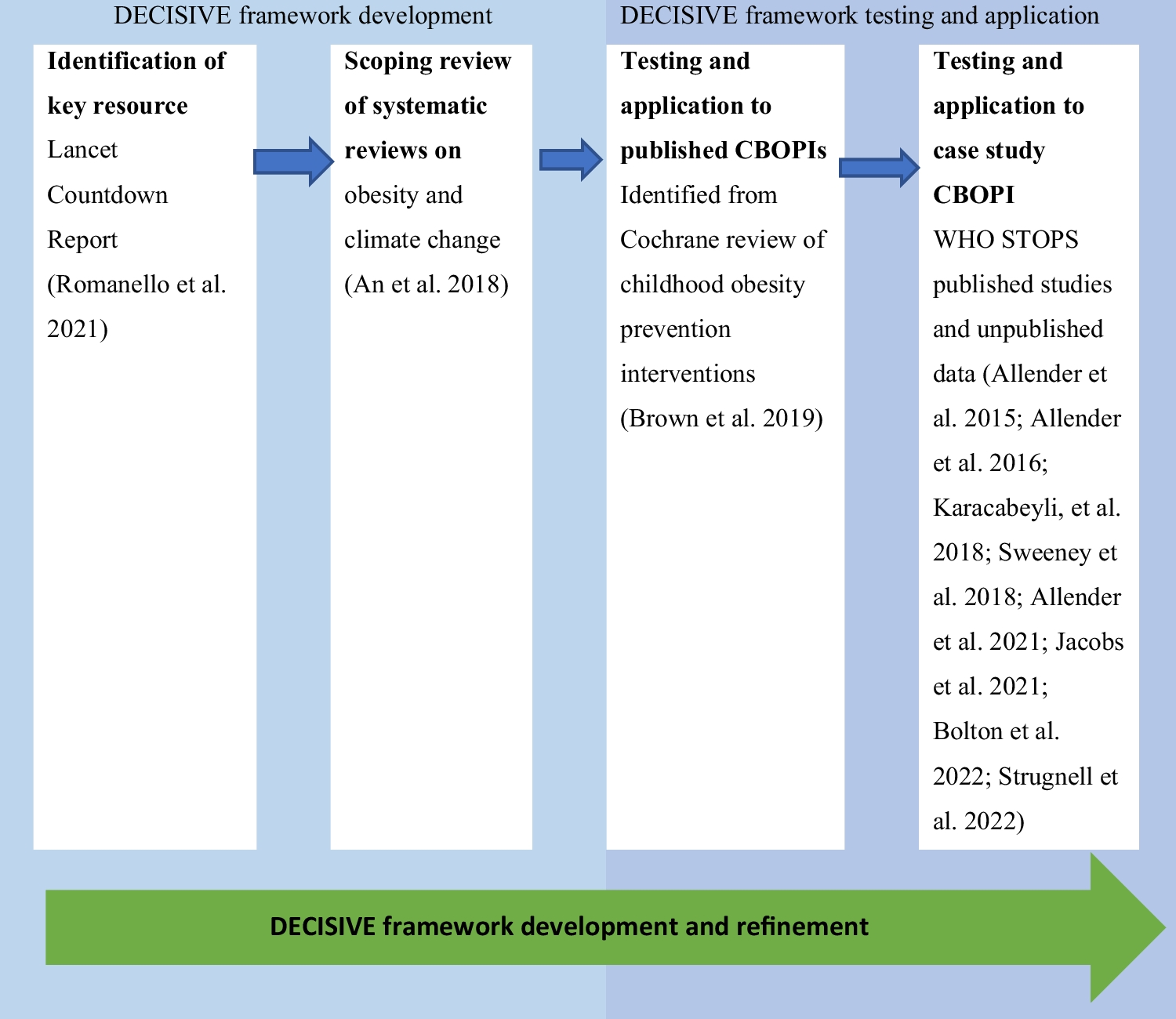
This pilot study is conceived as a prospective interventional experimental study, the main purpose of which is supportive care. A total of 20 participants with PD were randomly assigned to the intervention (vCare group) or control group. A total of 10 patients were assigned to the intervention group and performed telerehabilitation with vCare system during a 4-month period. In addition, 10 patients were assigned to the control group with the same demographic characteristics who received the standard care at the clinic (Fig. 1). Participants were recruited through the Department of Neurology at Cruces University Hospital (Barakaldo, Spain). The study protocol was approved by the Basque Research Ethics Committee (CEIm-E, code: PS2021041). All participants gave written informed consent prior to their participation in the study, in accordance with the tenets of the Declaration of Helsinki.
Fig. 1
Study design for PD vCare group
Patients with PD fulfilled Parkinson’s UK Brain Bank criteria for the diagnosis of PD (Hughes et al. 1992). Other inclusion criteria: (1) Age > 60 years; (2) Patients with scores higher than 60% on the daily life activities scale of Schwab and England; (3) Presence of motor fluctuations perceived by the patient; (4) Hoehn and Yahr stage between 1 and 3; (5) Willingness to interact with technological devices; (6) Internet connection at home; (7) TV screen with HDMI port at home. The exclusion criteria were as follows (1) Patients diagnosed with atypical Parkinsonism, dementia, or other chronic diseases such as heart failure, severe lung, or liver problems; (2) bedridden patients; (3) Patients with severe psychiatric problems such as hallucinations or major depression; (4) Patients with poor adherence prior to pharmacological or rehabilitative treatment; (5) Unable to understand and comply with protocol and/or give informed consent.
Clinical and usability evaluationThe clinical evaluation protocol consisted of measuring: (1) QoL through the Euro Quality of Life 5 Levels (EQ5D-5L: mobility, self-care, daily activities, pain/discomfort, anxiety/depression, and perceived health) (Ramos-Goñi et al. 2018); (2) Cognitive general status with the Montreal Cognitive Assessment (MoCA) (Nasreddine et al. 2005); (3) Motor symptoms with the Unified Parkinson’s Disease Rating Scale (UPDRS) part I, II, III, and IV (Fahn et al. 1987); (4) Functional disability associated with PD and the progression of the disease with the Modified Hoehn and Yahr scale (H&Y) (Hoehn and Yahr 1976); (5) Capabilities for performing activities of daily living with the Schwab and England Activities of Daily Living (ADL) (Gillingham and Donaldson 1967).
The usability and satisfaction evaluations were only performed for the vCare group: (1) System usability scale (SUS) (Brooke 1986); (2) User Experience Questionnaire (UEQ) (Rauschenberger et al. 2013) evaluates 6 domains that include attractiveness, perspicuity, efficiency, dependability, stimulation, and novelty of the vCare system. The range of the scales is between -3 (“horribly bad”) and *3 (“extremely good”). Values between -0,8 and 0.8 represent a neutral opinion of the vCare system; values >0,8 represents a positive evaluation; while <-0,8 means a negative evaluation of the vCare system.
ProcedureThe vCare project consisted of 5 phases: 1. Definition of architecture/interface and technical preparation phase. The first stage was to define the architecture and interface of the system; 2. Preliminary phase. This phase consisted of modeling narratives using knowledge representation methods, such as pathways, profiles (diseases, users, coach, treatment, activity, performance, and environment), and ontologies depending on the disability/ impairment to be recovered. The activity was performed according to a process-driven approach, addressing different care pathways and related supporting services; 3. Tech Labs phase. This phase consisted of performing the test setup including test preconditions, test conducted execution, test validation dimensions, impressions of medical partners during and after the tests, and finally a comprehensive test summary. In addition to the functional requirements validated by the test cases, the non-functional requirements were also addressed; 4. Living Labs phase. The Living Lab Phase included PD patients recruited at Biocruces Bizkaia Health Research Institute/Cruces University Hospital (ethical committee approval Code: PS2020039) and had the aim to assess the vCare system usability of the devices and the satisfaction level of the 20 PD patients involved in the present study for a two-week period in a ‘controlled environment’. This controlled environment was an apartment intended exclusively for the living lab, which was provided with all the necessary equipment to perform the vCare telerehabilitation and monitoring system, where patients behaved like at their own homes (Seregni et al. 2021); 5. Pilot phase. Finally, the pilot test was conducted at the patients homes for 4 months. Patients were assigned to the intervention or control group by randomization (not masked) in 5 blocks of 4 subjects for each block. Figure 2 shows the flow diagram. All patients performed a clinical evaluation (pre- and post-intervention), and the clinicians designed the personalized telerehabilitation program for each patient included in the PD vCare group. However, the control group for this study did not perform traditional rehabilitation, just the clinical health standard at the clinic.
Fig. 2
Flowchart of group enrolment
RehabilitationDefinition of the rehabilitation treatmentThe vCare telerehabilitation followed a routine of clinical condition monitoring, risk prevention, and motor and cognitive rehabilitation synchronized by an intelligent system with an avatar, which scheduled the rehabilitation based on the plan established by the clinicians responsible for the patient. The interaction between the patient and the avatar was done through a television and a tablet installed in the patient's home. The vCare system's intelligent algorithms adapted the rehabilitation routine set by the responsible clinicians to the patient's situation and continuously reported on the patient's clinical condition and response to rehabilitation.
Before defining the home telerehabilitation pathway provided through the vCare solution (Gand et al. 2021; Gißke et al. 2022) (for the vCare group), clinicians gathered the user’s personal data into the Professional Portal (KIOLA), and the client ID, the correspondent user, and password associated with the Gmail account was created for each user. These credentials were required to associate each user in the Keycloak and in the Knowledge representation framework (KRF) server. Finally, the clinical team defined the motor and cognitive status of the patient, by entering the most relevant clinical information collected during the pre-intervention evaluation.
The cognitive and motor telerehabilitation activities consisted on the serious games suite REHABILITY package (www.rehability.me) and included: (1) Attention; (2) Executive Functions; (3) Attention+ Executive Functions; (4) Mobility; (5) Strengthening; (6) Coordination; (7) Dexterity; (8) Speed; (9) Motor Control; (10) Postural Control; (11) Balance; (12) Endurance; (13) Rhythm. The clinical team the motor and cognitive telerehabilitation treatment to be performed at home.
The telerehabilitation for PD patients performed by the vCare system followed the same structure as the traditional rehabilitation at the clinic. The PD vCare group performed the motor and cognitive rehabilitation sessions 4 times a week (2 days for motor sessions and 2 days for cognitive sessions). The games selected, the time per game and the difficulty for each game were different and personalized for each patient. The motor session was performed through a TV connected with a 3-dimensional (3D) camera and with a mini-PC unit while the cognitive session was done with a tablet; both platforms were connected to the internet, to vCare dedicated cloud servers, and the vCare app (the avatar) installed in the tablet. Each session lasted approximately 30 minutes, 20 minutes at the minimum and 45 minutes at the maximum. Traditional rehabilitation is guided by a clinician (physiotherapist and neuropsychologist) while in the vCare system, the virtual coach guided the patient once the clinician has designed in the platform the rehabilitation plan for each patient.
Before performing the rehabilitation, the patient had to open the vCare app to interact with the virtual coach. Before the telerehabilitation session, patients were evaluated by the vCare avatar with a fatigue questionnaire (Herlofson and Larsen 2002), and depending on the score, a specific telerehabilitation session was personally designed for each patient. For example, if the patient did not present fatigue, the patient was invited by the virtual coach to participate in the scheduled sessions via notifications on the tablet, and during the session, it provided the user with postural feedback in real-time to correct any posture compensation. However, if the patient presented with a fatigue score, depending on the degree of fatigue, the vCare avatar coach suggested resting and/or a shorter telerehabilitation session.
The motor serious games proposed by Virtual Coaching were task-oriented, through gestures performed while sitting or standing, to stimulate the body districts and (neuro) motor functions in agreement with the motor deficit shown by the patient during clinical evaluation. The cognitive serious games included the following cognitive domains: selective, divided, and sustained attention, visual-spatial planning, abstraction, categorization, working memory and calculation. In addition to the home-based motor activities and home-based cognitive games, each PD patient vCare system was assigned electronic learning (E-learning), coaching for an active lifestyle, and falls prevention programs. Subjects had available a library of educational and informative multimedia content about rehabilitation, including the management of home risks, information about the disease, the motor and non-motor symptoms, and information related to different treatments for PD. This material was used within the vCare app installed on the tablet supplied to all patients.
PD vCare group monitoringThe monitoring task was performed through different sensors: movement and presence sensors from MYSPHERA (www.mysphera.com), the smart band (Beurer AS97 or XIAOMI band) recorded the daily number of steps and the heart rate, and the STAT-ON device (PD Holter, www.statonholter.com) recorded the PD motor symptoms such as freezing of gait, number of steps, movement, bradykinesia, time in OFF and ON state, and dyskinesias. The movement and presence sensors and the smart band were installed at the patient’s home for the whole telerehabilitation period. However, at the house of the patients PD01 and PD02, there seemed to be a technological issue with the connection of the devices and just the sensor of the bedroom was recording the information and only for 2 months. The STAT-ON device was used during the first and last week of the Pilot study (7 days each week). In addition, the clinical staff facilitated the patients with a telephone number to contact if needed. Almost every week, contact was maintained with the vCare PD patients to verify that everything was working correctly and/or if there were any technical issues to solve them.
Cost-utility analysisData related to QoL were collected from the EQ5D-5L before and after the intervention in both groups. Regarding the utilities, values from 0 to 1 have been obtained for the health states provided by the patients through the EQ-5D-5L quality of life survey, following the methodology published by Ramos-Goñi et al. (2018). The patient pathway for traditional rehabilitation and the one that would be followed with vCare were reviewed and validated (Ramos-Goñi et al. 2018). With this information, the use and consumption of resources for both types of rehabilitation were quantified. Information on the unit cost of each of these resources was extracted from the Ezkerraldea-Enkarterri-Cruces Integrated Healthcare Organization (EEC IHO) Cost per Patient Information System (Osakidetza). The costs per patient of both rehabilitation (regular rehabilitation at the clinic versus vCare telerehabilitation) were calculated using the following resources from the hospital information system: face-to-face neurological, neuropsychological, and motor consultation (first and successive), telephone consultation (first and successive), motor and cognitive rehabilitation, neuropsychological evaluation; and from the vCare system costs: avatar voice, Rehability (i-maginary), vCare maintenance, devices, design of motor and cognitive sessions, installation and uninstallation of devices. Both types of rehabilitation include three consultations at the beginning and at the end of the process, which lasts 4 months. Motor and cognitive rehabilitation (both, telerehabilitation or standard care) were performed 4 times a week for 12 weeks. Both rehabilitations included a face-to-face clinical, neurological, neuropsychological, and motor pre-post evaluation (Time 0 and Time 1). During the traditional rehabilitation time, no face-to-face consultation is needed while during the vCare telerehabilitation, a telephone follow-up consultation is performed 2 times a month.
The cost of subsequent consultations is half the cost of the first consultation, according to corporate criteria. The cost of telephone consultations is 0.4 of the cost of a face-to-face consultation, according to corporate criteria. The cost of motor rehabilitation corresponds to neurological rehabilitation sessions of the EEC IHO Rehabilitation Service. The cost of cognitive rehabilitation corresponds to the cost of a neuropsychological consultation.
Statistical analysisDemographic and clinical data of PD patients (vCare and control group) were collected and recorded on an Excel sheet by the clinical team. Statistical analyses were carried out using IBM SPSS Statistics for Windows, version 20.0 (IBM-SPSS, Armonk, New York). The Kolmogorov-Smirnov test was performed to determine whether the study variables followed a normal distribution. Descriptive analyses were performed for the mean and standard deviation of each variable at time 0 (baseline, pre-intervention) and time 1 (post-intervention). Repeated measures ANOVA was performed to test “groupxtime” interaction between PD vCare group and the control group at post-treatment compared to pre-treatment. Moreover, the Wilcoxon test for intergroup differences was performed. Regarding the data extracted from the STAT-ON device, a t-test for paired samples was used since the STAT-ON recorded a large number of measurements for each patient and compared the differences between the pre-and post-intervention of these groups of measurements. The data extracted by the vCare app was facilitated by the technical team in charge of that task [Forschungszentrum Informatik (FZI), Austrian Institute of Technology (AIT), and IMAGINARY SRL (IMA)]. In addition, correlations between MoCA, UPDRS, EuroQol-5D, data extracted from the STAT-ON device, and data extracted by the vCare app were analysed with Spearman's bivariate correlation coefficient. Statistical significance was set at p<0.05 (two-tailed). The outcome measures were analysed according to the objectives established for the PD pilot.
Regarding the monitorization of motor symptoms through the STAT-ON Holter, each parameter of interest was compared using the mean measurement per day against two groups, pre-versus post-measurements. Each parameter was calculated using 3 strategies: (i) against all days, (ii) against the 3 worst days (the three days with the most hours in OFF), and (iii) against the 3 best days (the three days with the most hours in ON). Supplementary material (Table 1) presents the mean difference (pre minus post) and the p-value of the pre vs. post sets using the t-test. The measure per day is obtained by averaging the measure over the corresponding day. In the case of Hours OFF, OFF+INT, ON, ON+INT, dyskinesia (Dysk) and Gray] the measure per day is the percentage of monitored time in which the patient has been diagnosed with that state. Freezing of gait (FoG) episodes are counted by aggregating them by day. Finally, the thresholds (Upper: Threshold_HI and Lower: Threshold_LO) are common for all monitoring and therefore the table presents only the difference (pre minus post) between the thresholds of the two monitoring.
Lastly, the cost-utility was performed with the Monitoring and Assessment Framework for the European Innovation Partnership on Active and Healthy Ageing (MAFEIP) tool following the European recommendations, including the costs of both rehabilitations and the effectiveness measured in quality-adjusted life years (QALY), given a threshold of €20,000 per QALY (Vallejo-Torres et al., 2018).
留言 (0)