
記住我
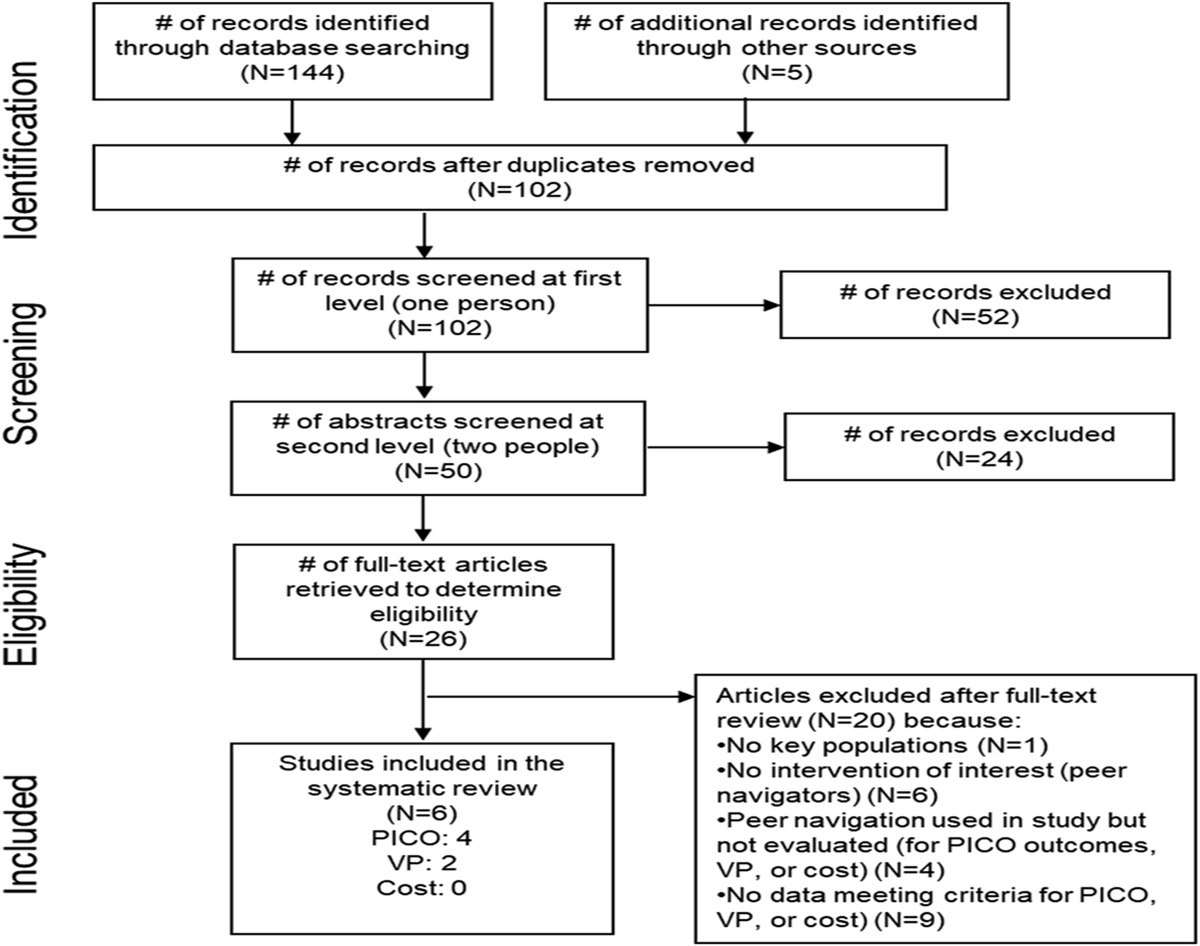

Differentiated service delivery (DSD) is an evidence-based strategy that adapts HIV services to better meet the needs and preferences of people living with HIV.1,2 Endorsed by the World Health Organization in 2016, DSD simplifies and streamlines HIV services for patients who are “clinically stable” (eg, retained in care and virally suppressed), enabling intensified service delivery to patients at risk of adverse outcomes, such as disengagement from care and HIV viremia. Various individual-based and group-based DSD models have been implemented for general and key populations in sub-Saharan Africa.3,4 However, DSD models for pregnant and postpartum women living with HIV (PPWH) are lacking, and there are limited data to guide the adaptation of DSD to this population's unique care needs and the context in which HIV services are integrated within maternal and child health clinics.5–7
A discrete choice experiment (DCE) is a market research method that has recently been used to measure patients' preferences for HIV services.8 This approach is premised on the notion that HIV service delivery should accommodate the preferences of its end users to optimize the patient-centeredness, acceptability, and uptake of services.9 Previous DCEs have found that patients prefer less compared with more frequent clinic visits, facility-based services compared with community-based services, and lower compared with higher costs for services.10–12 Patients' preferences for these attributes also outweigh their preferences for other service features, such as waiting times or travel distances. However, studies to date have focused on nonpregnant persons; it is unclear whether their findings extend to PPWH. Prevention of mother-to-child transmission of HIV (PMTCT) is a primary concern for this population, so it is conceivable that less intensive health services may not be preferred.13 Previous DCEs have also focused on individuals living with HIV who are clinically stable without sampling individuals considered “at risk.” The latter group may have distinct preferences that should be accounted for in any HIV service model.
Given the accelerated implementation of DSD during the COVID-19 pandemic and the growing recognition of the need for patient-centered HIV services, understanding women's preferences for DSD during pregnancy and the postpartum period is important.14 In Kenya, women are routinely given monthly clinic appointments during pregnancy and breastfeeding, which typically continues through 12–24 months postpartum. Although well-intended to enhance clinical support, these frequent clinic visits burden patients, and there is little evidence that they offer added benefit for those maintaining viral suppression through sustained adherence to antiretroviral treatment (ART). With the superior effectiveness of dolutegravir-containing ART and emerging data demonstrating minimal vertical transmission among pregnant and breastfeeding women who are virally suppressed, DSD could play a pivotal role in easing access to services for PPWH while preserving good clinical outcomes.13,15,16 Understanding women's preferences for DSD can also help define the future role of long-acting ART for this population. The objective of this study was to determine the preferences of PPWH for HIV services in Kenya to guide the adaptation of DSD to this population.
METHODS SettingKenya has one of the largest HIV burdens in the world with an HIV prevalence of 6.6% among women aged 15–49 years.17 In the current standard-of-care model for PMTCT services in Kenya (henceforth abbreviated “standard care”), HIV services are fully integrated within antenatal clinics (ANC) and postnatal clinics rather than delivered in HIV clinics. In integrated ANC clinics, standard care for pregnant women living with HIV consists of monthly appointments that involve separate encounters with a midlevel clinician (ie, clinical officer) and mentor mother (ie, peer counselor) at each appointment. Postpartum women and their infants continue similarly structured monthly appointments through at least 12 months postdelivery. This is typically followed by appointment spacing every 2–3 months through 18–24 months postdelivery and cessation of breastfeeding, when the child's final HIV test is performed. Routine visit frequency for pregnant women without HIV was based on the WHO-focused antenatal care model, which recommended at least 4 visits at 8–12, 24–26, 32, and 36–38 weeks of pregnancy.18 As such, the monthly ANC visit schedule for women living with HIV (WHIV) superseded the 4-visit focused antenatal care model for women without HIV. Routine infant immunizations were recommended at 6, 10, and 14 weeks and at 6, 9, and 18 months. At the time of this study, Kenyan HIV treatment guidelines recommended dolutegravir-based first-line ART for adults aged 15 years or older.19 Viral load testing was recommended every 6 months for women who were pregnant or breastfeeding.
Sampling FramePPWH were eligible to participate in this study if they were aged 15 years or older, able to understand English or Kiswahili, pregnant or ≤24 months postpartum, and enrolled in the PMTCT care at one of the following facilities affiliated with the Academic Model Providing Access to Healthcare: Moi Teaching and Referral Hospital, Busia County Referral Hospital, Kitale County Referral Hospital, Uasin Gishu County Hospital, and Huruma Sub-County Hospital. These hospitals serve urban and periurban populations in different ethnic and geographic settings and are representative of Ministry of Health facilities in the country. Each facility services 30–70 pregnant women with HIV per month.
PPWH were consecutively sampled from each facility, stratified by pregnancy status and retention status (retained vs. gap in care) to obtain a generalizable sample of the PMTCT population (see Table 1 for sampling strategy and map of study facilities, Supplementary Digital Content, https://links.lww.com/QAI/C119). Women were defined by the study as having a gap in care if they did not return to the facility for >30 days after their last missed scheduled visit and were not documented as deceased or transferred out. Women retained in care were approached by a research assistant after their routine clinic appointment. Women with a gap in care were identified by medical record reviews and recruited by phone or in person through community tracing in collaboration with the facility outreach team. The target sample size at each facility was set proportional to each facility's monthly PMTCT patient volume. For this study, we aimed to recruit 250 women based on Johnson and Orme's sample size equation.20 This sample size is within the range of other published DCEs according to our scoping review.8
Attribute SelectionWe selected attributes for the DCE based on the literature,5,6,8,21,22 our previous qualitative work among PPWH,13 and additional qualitative interviews with 12 PMTCT providers (manuscript under review). Based on these data, we determined that a facility-based, individual DSD model would be more preferred by patients and feasible to deliver than a group and/or community-based model. A community-based, group model for postpartum women has been implemented in South Africa.23 However, we previously investigated women's preferences for such a model and found that in our setting, women prefer facility-based services, which is partly driven by a perceived risk of HIV disclosure and stigma in the community.13 A facility-based DSD model would also require minimal changes to the program infrastructure.
Thus, we selected the following attributes and levels relevant to facility-based, individual DSD: visit frequency during pregnancy (every month vs. every 2 months); visit frequency during the first 12 months postpartum (every month vs. only during infant immunization visits, defined above); meeting with a mentor mother (at each clinic visit vs. not at each visit but as needed based on the woman's preference or as determined by the care team); meeting with a clinician (same levels as for the mentor mother attribute); and basic consultation cost (0, 50, or 100 Kenya Shillings [KSh]). The less frequent visits also represent multimonth prescribing of ART for the mother and antiretroviral prophylaxis for the infant, while the “as-needed” meetings with a mentor mother and clinician represent “fast-tracked” appointments which are common components of facility-based DSD. Consultation cost is variable across public facilities in western Kenya and dependent on a patient's insurance coverage, but it is generally in the range of 0–100 KSh. Concepts for the illustrations of each attribute level were initially developed through discussion with the Kenyan investigators on our study team (Fig. 1). Concepts were then submitted to a professional illustrator contracted through FIVERR (www.fiverr.com). The illustrator developed colored prototypes which were further refined through iterative review by the study team and 2 mentor mothers at Moi Teaching and Referral Hospital who were knowledgeable about the target population. This helped ensuring that the illustrations appropriately conveyed the meaning of the attribute levels for participants with varying literacies.
 FIGURE 1.:
FIGURE 1.: Attributes and levels for the DCE.
Experimental DesignWe used Sawtooth software (Provo, UT) to develop a D-efficient, randomized design that adhered to orthogonality and level balance after best practices (see Table 2, Supplemental Digital Content, https://links.lww.com/QAI/C119).24 Each respondent received a unique set of 12 choice tasks containing 2 choice sets per task in which each choice represented a different hypothetical PMTCT clinic with each of the 5 attributes. For each choice task, respondents were asked to choose which clinic they would most prefer. No fixed tasks or opt-outs were presented based on the rationale that PMTCT services are recommend for all PPWH and their infants. The DCE was piloted among 15 PPWH. During this process, we found that some PPWH struggled to understand the tasks and became fatigued toward the end of the questionnaire. Therefore, a modest degree of balanced level overlap was incorporated into the DCE questionnaire to improve the respondent efficiency and account for the noncompensatory decision behavior, while minimizing the impact on statistical efficiency. The correlation between attributes was low (2-log likelihood P-value ≥0.10 for all potential two-way interaction effects).
Data Collection and ManagementA trained research assistant administered a structured demographic and clinical questionnaire and DCE in person with each participant. Responses were recorded on a tablet using the REDCap mobile application. The DCE was also administered on a tablet using the web-based Sawtooth program. Both the questionnaire and DCE were translated into English and Kiswahili and administered in either language according to participant preferences. The research assistant oriented each participant to the DCE questionnaire using a structured introduction and by carefully verifying participants fully understood the choice tasks and meanings of the attributes and levels. This included descriptions of the standard care visit structure and frequency and infant immunization schedule. The same research assistant administered the DCE to all participants.
Patient-level independent variables collected at study enrollment included age, facility, educational attainment (ie, highest level of completed education), employment, monthly family income, travel time to the facility, queuing time during a routine appointment, pregnancy status, retention status, and timing of HIV diagnosis (ie, newly diagnosed with HIV at enrollment in ANC vs. known positive). HIV-related variables were also extracted from the Academic Model Providing Access to Healthcare electronic medical record for each participant and included years on ART, antiretroviral base at study enrollment, and HIV viral load (most recent within 1 year before study enrollment).
Statistical AnalysisWe summarized the characteristics of participants overall and by retention status using the χ2 test and the Fisher exact test to compare categorical variables and the two-tailed sample t test and the Wilcoxon rank-sum test to compare continuous variables. Viral suppression was defined as <200 copies/mL according to the Kenya treatment guidelines.18 We used a multinomial logit model to determine the strength of women's preferences for each attribute level by estimating utilities for all main effects (β-coefficients), which reflect the relative impact of each attribute level on clinic choice compared with a reference level, measured independently of the other attributes. Positive values for β represent a positive preference for the attribute level, with higher values representing stronger preferences and negative values representing negative preferences. We calculated the importance score for each attribute across individuals by converting the utility estimate ranges for each attribute into a proportion that sums to 100%. The magnitude of each score represents how impactful the attribute was on participant choice.
Using a market simulator (share of preference) model in Sawtooth, we used the individual-level utility estimates to identify the clinic model (ie, choice set) that yielded the maximum utility to participants compared with standard care (defined above), with the cost set to 0 KSh for both models. We used generalized linear regression with a log link function and a binomial distribution (ie, log-binomial regression) to estimate unadjusted and adjusted risk ratios for associations between covariates selected a priori, with an outcome defined as >50% preference for the maximum utility model compared with standard care. The primary exposure was the retention status. Additional covariates included age, education, employment, family income, parity, timing of HIV diagnosis, retention status, travel time, queuing time at the facility, and facility, which was included in the models as a factor variable. Because >20% of participants were missing a recent viral load, we included the viral suppression status (ie, suppressed vs. not suppressed) in the models as secondary analyses that excluded those with missing viral loads. We checked for multicollinearity among the independent variables using the variance inflation factor, finding values ≤1.6 for all variables indicating a low degree of collinearity. To explore preference heterogeneity, we calculated importance scores for each attribute by stratifying participants according to the previously described demographic characteristics. Analyses were performed using Sawtooth software and Stata version 14 (College Station, TX).
Ethics ApprovalsThe study was approved by the Moi University/Moi Teaching and Referral Hospital Institutional Research and Ethics Committee in Kenya and the Indiana University Institutional Review Board in the United States. A research permit was also granted by the National Commission for Science, Technology, and Innovation (NACOSTI) in Kenya. All participants provided written informed consent, and the data were coded for analysis using a study identification number assigned to each participant so that the data could not be linked to the participant except by using a linkage log.
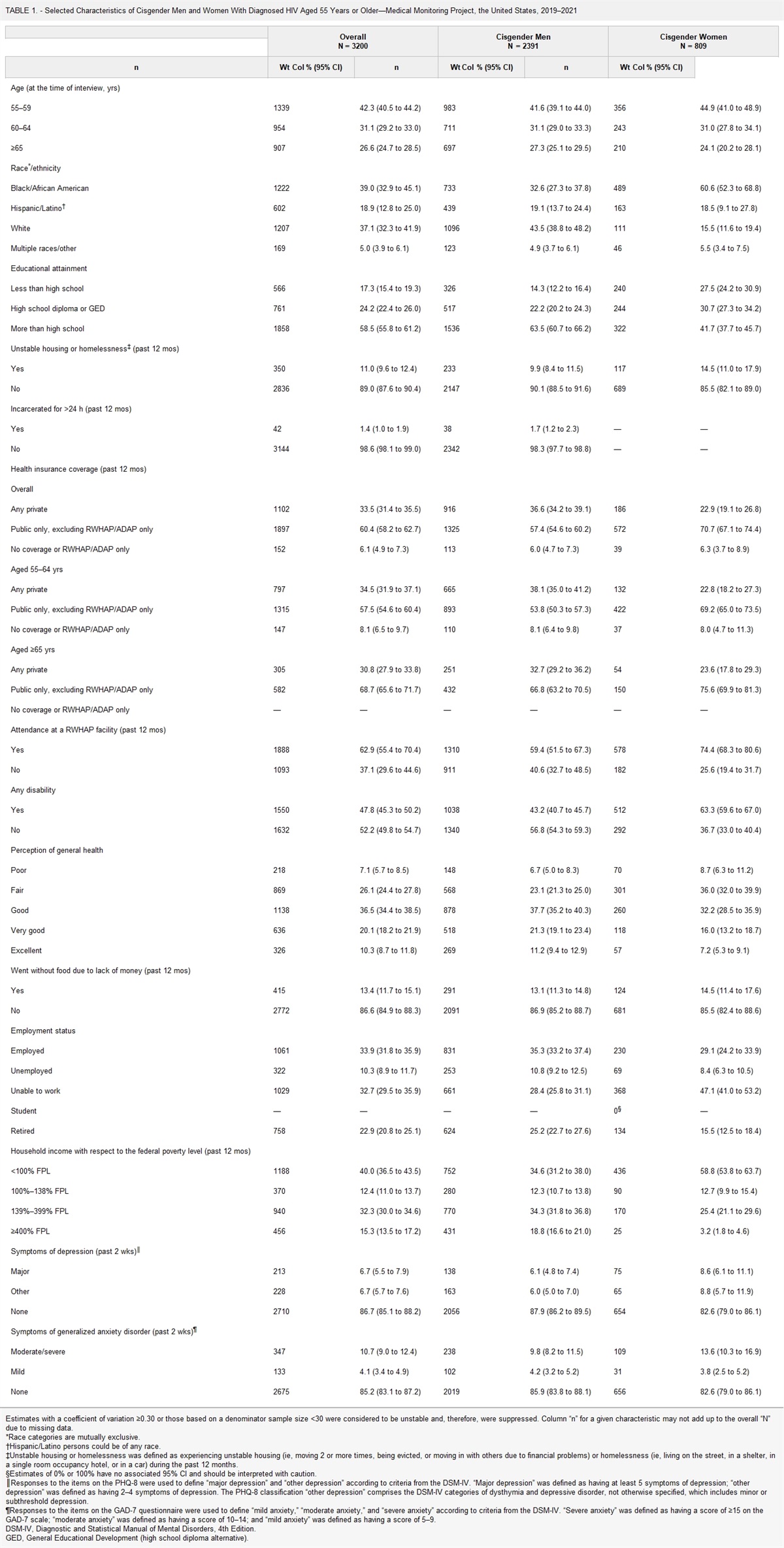
RESULTS Characteristics of ParticipantsA total of 250 PPWH enrolled in the study from April to December 2022 (Table 1). One patient completed the demographic questionnaire but not the DCE citing insufficient time to continue participating. The median (interquartile range [IQR]) age at enrollment in the study was 31 (26–36) years, 29% had not completed primary school, 47% were unemployed, and 43% reported a family income ≤10,000 KSh/month. Overall, 104 (42%) women were pregnant with a median (IQR) gestational age of 28 (22–35) weeks, and 146 (58%) were postpartum at a median of 11 (6–17) months postpartum. A third of women overall were newly diagnosed with HIV at enrollment in PMTCT services. Among women diagnosed with HIV before enrollment in PMTCT services (ie, known positive), their median time on ART was 6.4 (3.2–9.9) years. Most (92%) of the women were taking the dolutegravir-containing ART. A viral load was available for 195 of the 230 women who had been on ART for at least 3 months at study enrollment, 180 (92%) of whom were virally suppressed.
TABLE 1. - Characteristics of Participants Characteristic Total (N = 250) n (%) Age, median years (IQR) 31 (26–36) Facility Moi Teaching and Referral Hospital 70 (28) Busia County Referral Hospital 60 (24) Kitale County Referral Hospital 45 (18) Uasin Gishu County Hospital 45 (18) Huruma Sub-County Hospital 30 (12) Educational attainment None 72 (29) Primary 83 (33) Secondary 46 (18) Tertiary or higher 49 (20) Unemployed 117 (47) Family income (Ksh/month) <1000 13 (5) 1001–10,000 94 (38) >10,000 143 (57) Travel time to facility, median minutes (IQR) 40 (30–60) Queuing time* ≤60 min 153 (62) >60 min 95 (38) Pregnant 104 (42) Parity >1 68 (27) Retention status Retained 200 (80) Gap in care 50 (20) Timing of HIV diagnosis New positive 78 (31) Known positive 172 (69) Years on ART, median (IQR)† 6.4 (3.2–9.9) Antiretroviral base Dolutegravir 229 (92) Atazanavir or lopinavir 18 (7) Efavirenz or nevirapine 3 (1) Viral load <200 copies/mL‡ 172 (88)*n = 248.
†Among 172 women diagnosed with HIV before enrollment in PMTCT services.
‡Among 195 women with an available viral load.
As per the protocol sampling frame, 200 women were retained in care and 50 had a gap in care. Among the latter group, the median number of days to study enrollment after the first missed scheduled visit was 66 (IQR 43–130) days, with a range of 30–343 days. A few women (6%) reported transferring in from another facility to the study facility during pregnancy or postpartum follow-up, and none of the women with a gap in care reported being in care at another facility. A significantly higher proportion of women with a gap in care were postpartum at enrollment in the study versus pregnant (90% vs. 10%, P < 0.01, see Table 3, Supplemental Digital Content, https://links.lww.com/QAI/C119).
PreferencesWomen had the strongest preferences for pregnancy visits every 2 months (β = 0.15), postpartum visits only during infant immunization visits (β = 0.36), and 0 KSh consultation cost (β = 0.39) (Fig. 2). Women also had weaker positive preferences for seeing a mentor mother and clinician at each visit (β = 0.05 and 0.08, respectively). The strongest negative preference was for 100 KSh cost (β= −0.41).
 FIGURE 2.:
FIGURE 2.: Results of multinomial logit regression models for preferences.
Compared with standard care, the clinic model that yielded the maximum utility to participants consisted of pregnancy visits every 2 months, postpartum visits only with infant immunization visits, and mentor mother and clinician meetings at each encounter. Most participants (75%, 95% CI: 71–88) were predicted to prefer this model over the current standard care (25%, 95% CI: 21–29).
In the unadjusted model, preference for the maximum utility model over standard care was associated with enrollment at Huruma Sub-County Hospital (risk ratio [RR] 0.64, 95% CI: 0.44–0.93) and Kitale County Referral Hospital (RR 1.25, 95% CI: 1.08–1.40) (see Table 4, Supplemental Digital Content, https://links.lww.com/QAI/C119). These estimates were similar to those in the covariate-adjusted model. In the secondary analyses, preference for the maximum utility model over standard care was significantly associated with viral suppression in the unadjusted (RR 2.81, 95% CI: 1.12–7.01) but not adjusted model (RR 1.22, 95% CI: 0.92–1.65).
Importance scores were generally similar among participants when stratified by age, employment status, timing of HIV diagnosis, queuing time, and facility (Fig. 3; see Table 5 for importance score percentages and Table 6 for raw utilities for each attribute level by participant characteristic, Supplemental Digital Content, https://links.lww.com/QAI/C119). There was a trend toward lower relative importance of consultation cost and proportionally higher relative importance of visit frequency among women with increasing family income and educational attainment and among women retained in care versus those with a gap in care.
 FIGURE 3.:
FIGURE 3.: Preference shares among participants overall and by participant characteristics.
DISCUSSIONThe central finding of our study is that the large majority of PPWH in our study in western Kenya, regardless of their sociodemographic characteristics, would prefer a service model that includes less frequent clinic appointments compared with the monthly appointment frequency in the current standard of care. This finding strongly supports the rationale for adapting a DSD model to this population within clinics, offering integrated HIV and maternal–child health services. Such a model would be more responsive to women's preferences for services during pregnancy and the postpartum period and thus, more patient-centered. This model could reduce long queuing times and enable delivery of more intensive services to patients at risk of adverse outcomes. In addition, aligning postpartum visits with the infant immunization schedule could streamline services for mother–child dyads while still accounting for routine weight-based infant antiretroviral dose adjustments, infant HIV testing, and maternal viral load testing. The finding that most women prefer ANC visits every 2 months rather than monthly should be evaluated in the context of program policies and resources because it would not be rational to reduce the visit frequency for pregnant WHIV to less than what is recommended for women irrespective of HIV status. This could mean aligning the visit schedule for stable pregnant WHIV with that of women without HIV, such as the 4-visit schedule. Extended ART refills could also allow for less frequent HIV-focused visits while maintaining routine ANC contact. Future research is needed to assess the implementation outcomes and effectiveness of a facility-based DSD model for PMTCT, including the model's cost-effectiveness and acceptability to providers and male partners of PPWH.
The potential association between viral suppression and preference for the DSD model is also notable but requires cautious interpretation because 22% of participants were missing a viral load. It is conceivable that women who were virally suppressed had greater agency and self-empowerment to manage their HIV infection and ART and thus preferred less frequent appointments. Conversely, women who were not virally suppressed possibly preferred more frequent appointments to help them overcome barriers to care and achieve viral suppression. Understanding the impact of viral suppression on patient preferences for services may have important implications on the delivery of patient-centered care and requires further study.
As anticipated, having no consultation cost was also important to women in this resource-constrained setting, particularly among those with lower levels of education and income. Women also preferred seeing a mentor mother and clinician at each visit rather than as needed, but their preferences for these attributes were weak relative to their preferences regarding visit frequency and cost. Given this, a facility-based DSD model could potentially reduce patient contact with a clinician or mentor mother, for example, through fast-track encounters, while remaining largely acceptable to PPWH. This approach would require further evaluation because studies have demonstrated improved retention and viral suppression among PPWH accessing mentor mother services.25,26 Establishing a therapeutic relationship with patients is a core aspect of clinicians' and mentor mothers' ability to counsel and intervene, which could be diminished if insufficient time is allocated for patient–provider interactions. More research is needed to understand what PPWH value in their encounters with mentor mothers and clinicians to enhance, and not diminish, the utility of these services for this population.
We did not identify diverging preferences between PPWH retained in care compared with those with a gap in care or among PPWH stratified by several other sociodemographic characteristics. This is likely related to the study population's similar preferences for less frequent visits and no consultation cost, as well as the study's modest sample size. However, we did find that attending Kitale County Referral Hospital was associated with higher risk and attending Huruma Sub-County Hospital was associated with lower risk, of preferring the maximum utility model over standard care. To date, the DSD literature has predominantly focused on determining characteristics of patients that differentiate them as “stable” or “unstable” in relation to a clinical outcome or which predict their preferences for services. Comparatively less attention has focused on the characteristic of the facilities themselves or the patient–provider interactions they host and how these elements shape women's experiences and preferences for care. For example, previous DCEs have consistently found that, when given the choice, patients strongly prefer nice and respectful providers over rude providers, and their preference for this attribute outweighs their preferences for other attributes of service delivery.11,27 Previous studies have also found associations between retention in PMTCT services and nurse-to-patient ratio, facility size, and rural versus urban location.28–30
Although we did not explore these factors in depth, it is notable that Kitale County Referral Hospital is a large-volume, urban district facility compared with the smaller-volume, periurban facility at Huruma. It is possible that the facility associations with a preference for DSD in our study are markers of unmeasured structural or operational characteristics of these facilities, such as additional facility fees, provider behaviors, drug/supply stockouts, or integration with the community. More research is needed to understand the facility characteristics that determine the fit and appropriateness of facility-based DSD in integrated HIV and maternal–child health settings.
A strength of our study is its focus on PPWH, who are underrepresented in the DSD and DCE literature. Including patients with a gap in care is also a strength because many studies only sample individuals attending clinics routinely, potentially biasing findings in favor of those retained in care. The DCE was further strengthened by in-person administration by the same research assistant for all participants, which helped ensure understanding of the attribute levels and choice tasks and reduce the potential for response and nonresponse biases compared with other DCE fielding strategies. The directionality of preferences for consultation cost (ie, a strong positive preference for 0 KSh and strong negative preference for 100 KSh) also indicates rational decision-making among respondents, supporting the validity of the data. A limitation of our study, which is common to DCEs, is that it is not possible to include all possible attributes influencing individuals' preferences for services. The DCE also did not include an opt-out, which can result in overestimation of demand. Because HIV services are recommended for all PPWH, we considered exclusion of an opt-out acceptable. Notwithstanding these limitations, our findings are consistent with previous studies assessing preferences for DSD among people living with HIV.10–12
CONCLUSIONPPWH strongly prefer less frequent clinic visits compared with the current standard-of-care PMTCT model in Kenya. This finding supports the adaptation of facility-based DSD for this population. More research is needed to understand the factors influencing women's preferences for services, including the variability in facility-level and provider-level characteristics and their influences on choice heterogeneity. Research is also needed to assess the implementation outcomes and effectiveness of a facility-based DSD model within integrated HIV and maternal–child health settings, including the model's cost-effectiveness and acceptability to its end users and policymakers.
ACKNOWLEDGMENTSThe authors thank the clinical staff at the study facilities for helping to make this study possible.
REFERENCES 1. World Health Organization. Key Considerations for Differentiated Antiretroviral Therapy Delivery for Specific Populations: Children, Adolescents, Pregnant and Breastfeeding Women and Key Populations. Geneva: World Health Organization; 2017. Available at: https://apps.who.int/iris/handle/10665/258506. Accessed August 15, 2023. 2. International AIDS Society. Differentiated Care for HIV: A Decision Framework for Antiretroviral Therapy Delivery. Geneva: IAS; 2017. Available at: https://differentiatedservicedelivery.org/wp-content/uploads/decision-framework-version-2-2017.pdf. Accessed August 31, 2023. 3. Hagey JM, Li X, Barr-Walker J, et al. Differentiated HIV care in sub-Saharan Africa: a scoping review to inform antiretroviral therapy provision for stable HIV-infected individuals in Kenya. AIDS Care. 2018;30:1477–1487. 4. International AIDS Society. Differentiated Service Delivery. 2023. Available at: http://www.differentiatedservicedelivery.org. Accessed June 3, 2023. 5. Chimukuche RS, Wringe A, Songo J, et al. Investigating the implementation of differentiated HIV services and implications for pregnant and postpartum women: a mixed methods multi-country study. Glob Public Health. 2021;16:274–287. 6. Roy M, Bolton Moore C, Sikazwe I, et al. A review of differentiated service delivery for HIV treatment: effectiveness, mechanisms, targeting, and scale. Curr HIV/AIDS Rep. 2019;16:324–334. 7. Long L, Kuchukhidze S, Pascoe S, et al. Retention in care and viral suppression in differentiated service delivery models for HIV treatment delivery in sub-Saharan Africa: a rapid systematic review. J Int AIDS Soc. 2020;23:e25640. 8. Humphrey JM, Naanyu V, MacDonald KR, et al. Stated-preference research in HIV: a scoping review. PLoS One. 2019;14:e0224566. 9. Ostermann J, Brown DS, de Bekker-Grob EW, et al. Preferences for health interventions: improving uptake, adherence, and efficiency. Patient. 2017;10:511–514. 10. Dommaraju S, Hagey J, Odeny TA, et al. Preferences of people living with HIV for differentiated care models in Kenya: a discrete choice experiment. PLoS One. 2021;16:e0255650. 11. Eshun-Wilson I, Kim HY, Schwartz S, et al. Exploring relative preferences for HIV service features using discrete choice experiments: a synthetic review. Curr HIV/AIDS Rep. 2020;17:467–477. 12. Eshun-Wilson I, Mukumbwa-Mwenechanya M, Kim HY, et al. Differentiated care preferences of stable patients on antiretroviral therapy in Zambia: a discrete choice experiment. J Acquir Immune Defic Syndr. 2019;81:540–546. 13. Humphrey J, Alera M, Kipchumba B, et al. A qualitative study of the barriers and enhancers to retention in care for pregnant and postpartum women living with HIV. PLOS Glob Public Health. 2021;1:e0000004. 14. Grimsrud A, Ehrenkranz P, Sikazwe I. Silver linings: how COVID-19 expedited differentiated service delivery for HIV. J Int AIDS Soc. 2021;24(suppl 6):e25807. 15. Mandelbrot L, Tubiana R, Le Chenadec J, et al. No perinatal HIV-1 transmission from women with effective antiretroviral therapy starting before conception. Clin Infect Dis. 2015;61:1715–1725. 16. Luoga E, Vanobberghen F, Bircher R, et al. Brief report: No HIV transmission from virally suppressed mothers during breastfeeding in rural Tanzania. J Acquir Immune Defic Syndr. 2018;79:e17–e20. 17. National AIDS and STI Control Programme. Preliminary KENPHIA 2018 Report. Nairobi: NASCOP; 2020. Available at: https://dc.sourceafrica.net/documents/119832-KENPHIA-Preliminary-Report-Final-Web.html. Accessed June 5, 2022. 18. Kenya Ministry of Health. National Guidelines for Quality Obstetrics and Perinatal Care. Nairobi: Kenya MOH; 2010. Available at: http://guidelines.health.go.ke:8000/media/National_Guidelines_for_Quality_Obstetrics_and_Perinatal_Care.pdf. Accessed June 5, 2022. 19. Kenya Ministry of Health. Kenya HIV Prevention and Treatment Guidelines, 2022. Nairobi: Kenya MOH; 2022. Available at: https://nphl.go.ke/wp-content/uploads/2022/11/Kenya-ARV-Guidelines-2022-2.pdf. Accessed August 31, 2023. 20. de Bekker-Grob EW, Donkers B, Jonker MF, et al. Sample size requirements for discrete-choice experiments in Healthcare: a practical guide. Patient. 2015;8:373–384. 21. International AIDS Society. Differentiated Service Delivery for Families - Children, Adolescents, and Pregnant and Breastfeeding Women: A Background Review. Geneva: IAS; 2016. Available at: https://www.differentiatedservicedelivery.org/wp-content/uploads/DSD-Families-review_28Nov-1.pdf. 22. Abuogi LL, Humphrey JM, Mpody C, et al. Achieving UNAIDS 90-90-90 targets for pregnant and postpartum women in sub-Saharan Africa: progress, gaps and research needs. J Virus Eradication. 2018;4(suppl 2):33–39. 23. Myer L, Odayar J, Malaba TR, et al. Improved virologic outcomes in postpartum women living with HIV referred to differentiated models of care. AIDS. 2022;36:2203–2211. 24. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16:3–13. 25. Carlucci JG, Yu Z, Gonzalez P, et al. The effect of a Mentor Mothers program on prevention of vertical transmission of HIV outcomes in Zambezia Province, Mozambique: a retrospective interrupted time series analysis. J Int AIDS Soc. 2022;25:e25952. 26. Sam-Agudu NA, Ramadhani HO, Isah C, et al. The impact of structured mentor mother programs on 6-month postpartum retention and viral suppression among HIV-positive women in rural Nigeria: a prospective paired cohort study. J Acquir Immune Defic Syndr. 2017;75:S173–S181. 27. Kruk ME, Riley PL, Palma AM, et al. How can the health system retain women in HIV treatment for a lifetime? A discrete choice experiment in Ethiopia and Mozambique. PLoS One. 2016;11:e0160764. 28. Lerebo W, Callens S, Jackson D, et al. Identifying factors associated with the uptake of prevention of mother to child HIV transmission programme in Tigray region, Ethiopia: a multilevel modeling approach. BMC Health Serv Res. 2014;14:181. 29. Bedelu M, Ford N, Hilderbrand K, et al. Implementing antiretroviral therapy in rural communities: the Lusikisiki model of decentralized HIV/AIDS care. J Infect Dis. 2007;196:S464–S468. 30. Tenthani L, Haas AD, Tweya H, et al. Retention in care under universal antiretroviral therapy for HIV-infected pregnant and breastfeeding women ('Option B+') in Malawi. AIDS. 2014;28:589–598.
留言 (0)