
Remember me







The study was approved by the local regional ethical committee (ECS 1191/2021).
PatientsConsecutive patients with an isolated pertrochanteric fracture treated with a proximal femoral nailing surgery in our level-1 trauma center between 1 January 2016 and 30 April 2021 were included. We excluded patients without at least a 3-month postoperative radiograph and patients with concomitant fractures that required further surgeries.
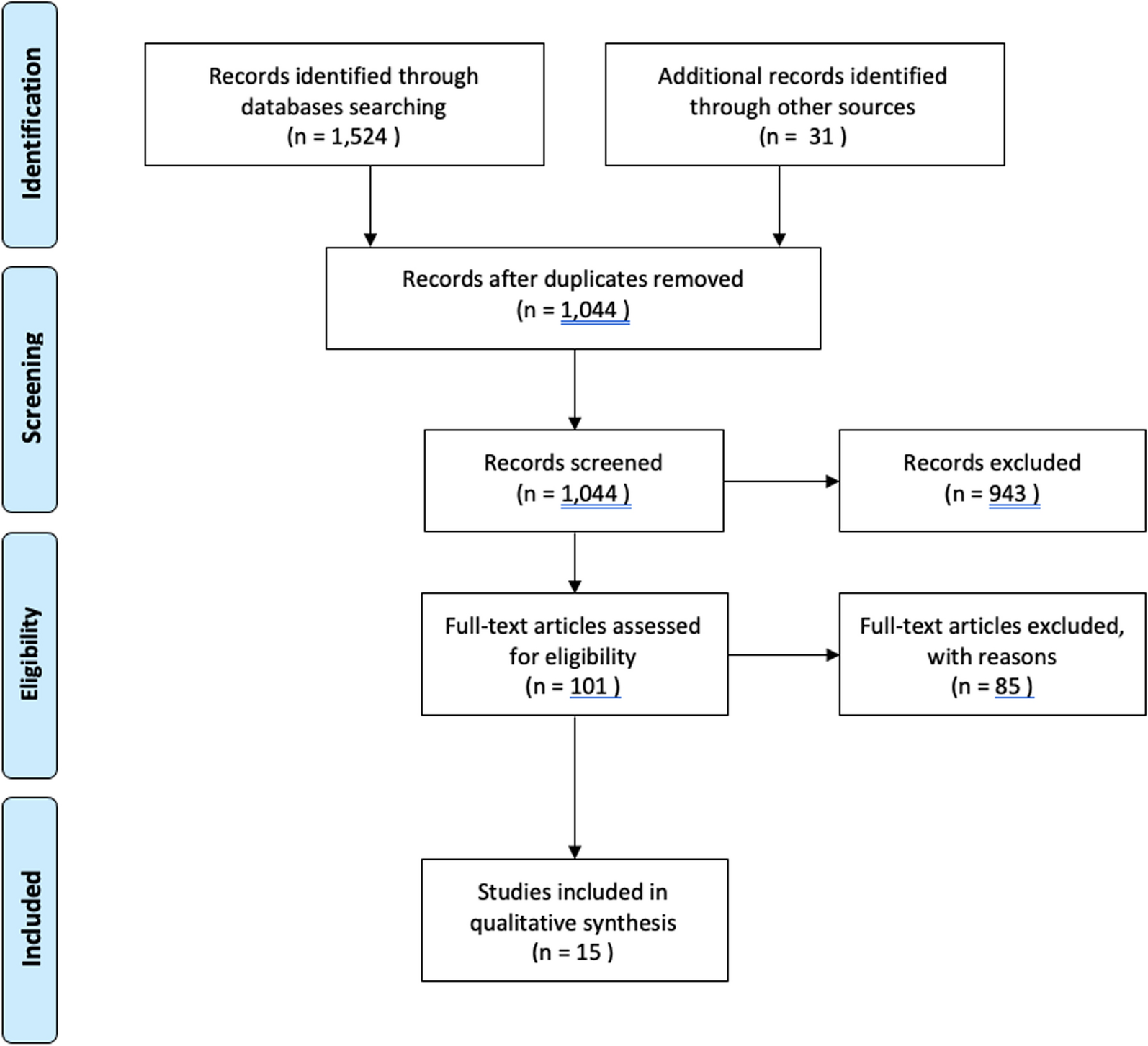
The data for 955 consecutive patients were extracted from this period (Fig. 1).
Fig. 1
We collected age, gender, side of injury, body mass index (BMI), and fracture classification according to the AO classification (31-A1 to 31-A3) [14]. We further collected intraoperative data—surgery date, surgeon, surgery duration, surgery start time, nail type and nail diameter, femoral neck implant, femoral neck implant length, and intraoperative radiological position of the femoral neck implant.
Postoperative complications were defined as infection (positive postoperative wound swab) or cut-out and revision surgery for any reason.
Radiographic evaluation was performed based on preoperative X-ray images. Furthermore, the position of the neck screw as well as signs of a cut-out were examined in the most recent images for each patient.
MethodsTo investigate the effects of level of training, the surgeons were assigned to four groups. Depending on the year of training of the residents at the time of surgery, they were assigned to groups 1–3 (group 1—training year 1 + 2, group 2—training year 3 + 4, group 3—training year 5 + 6). Senior surgeons were assigned to group 4.
Residency typically lasts 6 years. Before entering the training period, 9 months of basic training must be completed, at least 3 months of which must be in a surgical specialty. During this phase, however, the trainee is not yet involved in active surgical activities. For surgeons with prior surgical experience, the level of training is adjusted accordingly.
Surgery was performed with the patient in the supine position on an extension table. Preoperative single-shot antibiotics with 1.5 g cephazolin were standardized. After a reduction under fluoroscopy on both projections, the surgical area was prepped and sterilely draped. The surgical procedure corresponded to the procedures specified for the particular type of nail used. Open reduction was only performed when an anatomical reduction via closed reduction could not be achieved. Cerclage cables were used when the type of fracture needed extra stabilization. Postoperatively, thromboembolic prophylaxis with a low molecular weight heparin was administered for at least 10 days. Postoperative antibiotics were not used as standard. Full weight-bearing was possible immediately if the surgical treatment allowed it.
A senior surgeon was always present in the operating room during the first operations performed by residents. The transition, where the residents finally perform the operation without direct supervision, is completed before the end of the second-year training. After this transition, the senior surgeon is on standby, only getting involved if the trainee calls for the surgeon. This has the significant teaching benefit of increasing the responsibility held by the trainee. Fluoroscopic images showing the k-wire positioned inside the femoral neck were always supervised by senior surgeons during this transition time. Residents in advanced training years discussed the postoperative X-rays with a senior.
The assessment of the position of the femoral neck screw in the intraoperative fluoroscopic images was performed in anterior–posterior view as well as in axial view. For this purpose, the femoral neck was divided into thirds in each view, and thus the exact position was determined. Consequently, there were nine possible positions of the femoral neck screw (Fig. 2). Calculation of the tip apex distance (TAD) was also performed using intraoperative fluoroscopic images.
Fig. 2
Screw positioning within the femoral neck. The first number describes the cut-out cases, and the second number describes the total amount of screws in the particular area. The first percentage is the cut-out rate in each area, and the second percentage is the overall position rate
Classification of the fracture type was performed by four of the authors, two seniors, and two residents using the AO classification (31-A1 to 31-A3). Both inter- and intraobserver ICCs were high, 0.92 and 0.96.
The following incidents were included as complications: infections, defined as at least one documented positive wound swab; cut-out, identified in correlating fluorographs or computer tomography scans; and revision surgery, defined as documented unplanned surgery subsequent to the initial surgery provided [15].
StatisticsStatistical analysis was performed using IBM SPSS Statistics 28 (Chicago, IL, USA). Data are reported as mean (± SD) for normally distributed data and median [IQR] for non-normally distributed data. To test our hypothesis, we used the Pearson’s chi-square test. Significance was set at p < 0.05.
Comments (0)