
Remember me







In this retrospective follow-up study, patients at a level I trauma center (University Hospital) who underwent THA for treatment of traumatic femoral neck fractures between January 2019 and January 2021 were evaluated. All patients were surgically treated using a transgluteal Bauer approach in lateral position. Only cases with surgery performed by senior and chief physicians were included in the study. In these cases, residents were only involved in assisting positions.
The data was retrospectively collected using records of the patients and by using telephone follow-up interviews to evaluate the outcome and quality of the surgical treatment. The data was irreversibly anonymized. No experiments on patients were carried out. The physical integrity and the treatment of the patients were not affected by the data collection.
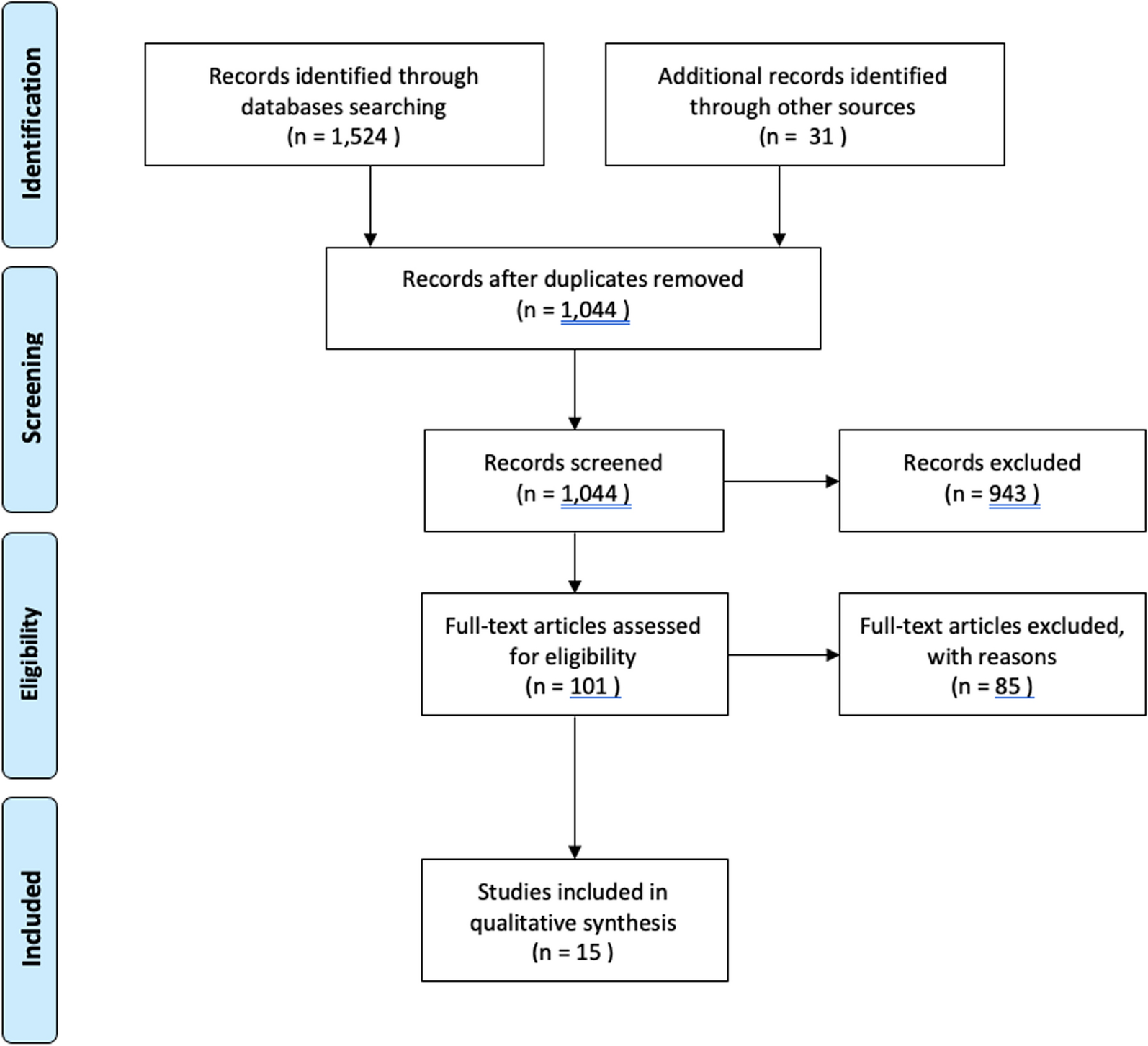
All applicable cases were screened for inclusion and exclusion criteria before study enrollment. In the recruitment procedure, pathological fractures and history of surgical procedures of both hips, including conversion osteotomies of the pelvis, femur, and knee were excluded. Patients with conditions that made proximal femoral replacements necessary were excluded, since high complication rates were reported in past studies [17]. In addition, a suitable postoperative radiograph meeting the quality requirements had to be available. The radiograph was checked for projection and rotation errors in the two-dimensional (2D) image. Figure 1 shows that the two deepest points of the ischiadic tuberosity were connected by a straight line (line 1), which is exactly perpendicular to the midline mark of the symphysis (line 2). At the same time, the symphysis marking had to intersect a drawn line from both outer edges of the ischial ramus, which passes over the deepest point of the obturator foramen (line 3) at its midpoint. Finally, both foramina were checked for size equality by diameter (line 4), and the distances from the projected linea iliopectinea and linea ilioischiadica (line 5) were measured. Deviations of the mentioned quality criteria > 1 mm also led to complete case exclusion, so that a study population of 110 patients was examined. A discrepancy to the opposite side > 0.1 mm ensured deliberate exclusion of the horizontal center-of-rotation position (RC-ML) (see below and Fig. 1) from further data analysis. This was done to mitigate the risk of inaccurate results. Due to the retrospective follow-up design of the study, the data set could not be collected completely for each patient, so the number varied (Table 1).
Fig. 1
Sketch of a pelvic overview. 1–5: Marks of quality requirements, 6: parallel to 1, 7: RC-SI, 8: THA and healthy horizontal distances, RC-ML = 8THA—8healthy, 9: anatomical leg length difference
Table 1 Overview of all variables collected including case numbers of the different endpoints and standard deviations and of all total endoprostheses used in the patient collective (Zimmer Biomet)Radiological measurementThe evaluated radiographs consisted of anterior–posterior pelvic overviews appropriate for the indication with generous exposure of the femur. The first postoperative radiographs were used to collect all variables. The following measurements are illustrated in Fig. 1. To determine the horizontal (RC-ML) and vertical (RC-SI) center-of-rotation position, the previously placed markers could be adopted to maintain quality requirements. In addition, a parallel line (line 6) was drawn to the straight line of both ischiadic tubera (line 1) starting from the healthy center of rotation, so that the RC-SI (line 7) could be determined from the center of rotation of the total endoprosthesis. Comparison of the horizontal distances of both sides was made by determining both distances (8THA and 8healthy) between the center of rotation and the marker running centrally through the symphysis (line 2). By subtracting 8THA—8healthy, the RC-ML could be formed. As described by Durand-Hill et al., the opposite side can be used in a reliable way for the planning THA [18]. Therefore, in our study, changes in COR are determined using the healthy side to evaluate the original COR position. Lastly, anatomic leg length (ALL) was determined by trochanteric lesser trochanter height differences (line 9).
Clinical data collectionTo ensure that possible unknown influencing factors are not missed, additional variables were collected on the basis of surgical protocols, patient history, and the internal digital data processing program ORBIS® (Agfa Health Care). These sources provided information about the inpatient course, the short-term recovery after surgery, and the need for care after discharge. Thus, the Barthel Index and the type of prosthesis used (Table 1) were considered in the statistical analysis. In our clinical routine, the nursing staff is in charge of determining the Barthel Index at admission and discharge. To achieve a long-term quality assessment mobility, independence and pain were evaluated using the Parker mobility score (PMS), the Barthel Index, and the pain level (NRS) at 6 and 12 months after surgery. This data were acquired using respective follow-up interviews. The follow-up interview was respectively conducted by telephone. Previous studies showed that prefracture mobility is an independent outcome predictor [19]. To analyze the isolated influence of rotation center reconstruction as precise as possible, only patients with full PMS (9/9) and full Barthel Index (100/100) before the fracture event were included in further analysis. This way, an interfering effect can be minimized.
Statistical analysisStatistical analysis was performed using SPSS® version 28.0 (IBM, SPSS Inc. Armonk, NY). Due to the ordinal scaled dependent variables, a nonparametric test had to be used. Possible outcome-relevant parameters were identified in a first correlation analysis according to Spearman, in which all variables were entered. For this purpose, RC-ML was additionally indexed to account for individual body relations, which were calculated as follows: RC-MLI = RC-ML/distance line 8healthy.
In our department we seem to have a tendency for superomedial cup positions (Table 1). This discovery of the frequently interrelated reconstruction positioning provided for the development of the CPS score. The formation by adding RC-ML and RC-SI is extremely useful especially for analyzing the milling direction and the effect of this superomedial versus inferolateral cup positions. The score takes on positive values for superior and medial cup positions and negative values for inferior and lateral cup positions. With a shallow and flat milling technique an inferolateral COR reconstruction is almost predetermined, especially with increasing cup size. A deep and steeper milling technique in combination with a small cup predisposes to a superomedial COR position. Patients with an RC-SI greater than 10 mm and RC-ML greater than 6.5 mm were excluded. Deviations of the center of rotation of this magnitude were considered to be clinically extreme displacements and should not artificially attenuate or even enhance a possible correlation.
In addition, three groups for center-of-rotation reconstruction were formed: medial (A), lateral (B), exact (C), and superior (A), inferior (B), exact (C). For consistent comparability, group C included all patients with a reconstruction accuracy of < 2 mm. Mann–Whitney U tests for further statistical analysis was performed. The nonparametric test (applicable for ordinally scaled dependent variable) makes putative outliers statistically evaluable. This had the advantage of not having to unnecessarily reduce the number of cases. The strict quality criteria of the chosen radiographs should make gross measurement errors unlikely. Overall nonparametric tests do not rely on the removal of outlier, so that no further reduction of cases was necessary. Furthermore, the recruitment of a sufficient number of cases was highly challenging due to the narrow inclusion corridor and many elder patients were not available for a follow-up survey. Despite these obstacles, the basic scientific idea of reproducibly accurate data collection was to be maintained. For this very reason, strict inclusion criteria were essential, especially with regard to the quality of the radiographs. Afterwards, a suitable case number was achieved to present significant results.
LanguageFluent English-speaking authors, some of whom are native speakers, wrote this text. This process was also supported by DeepL Translator [www.DeepL.com/Translator (free version)].
Comments (0)