
記住我

A 56-year-old woman experienced mild fever and fatigue (day 0), prompting her to seek medical attention at various medical facilities. Her nasopharyngeal swab polymerase chain reaction (PCR) for COVID-19 was positive. Fever and fatigue disappeared a few days after onset. About 2 weeks after these symptoms improved, she experienced difficulty with arm and hand mobility, speech articulation, and maintaining balance while standing. She consulted our department three days after the onset of these neurological symptoms (on day 22). On admission, her body temperature was 36.5 °C; other vital signs were normal. Despite an otherwise normal general exam, manifestations suggestive of cerebellar impairment were present. These signs included oculomotor overshoot, gaze-evoked nystagmus, and dysarthria with scanning speech. Further evaluation revealed pronounced ataxia involving both limbs and trunk, as well as intention tremor. The finger-to-nose and heel-to-knee tests revealed impaired coordination of limb movements. Muscle tone was hypotonic. Cranial nerve examination revealed no abnormalities. Muscle strength was normal and deep tendon reflexes were within normal limits. There were no sensory disturbances and no meningeal signs.
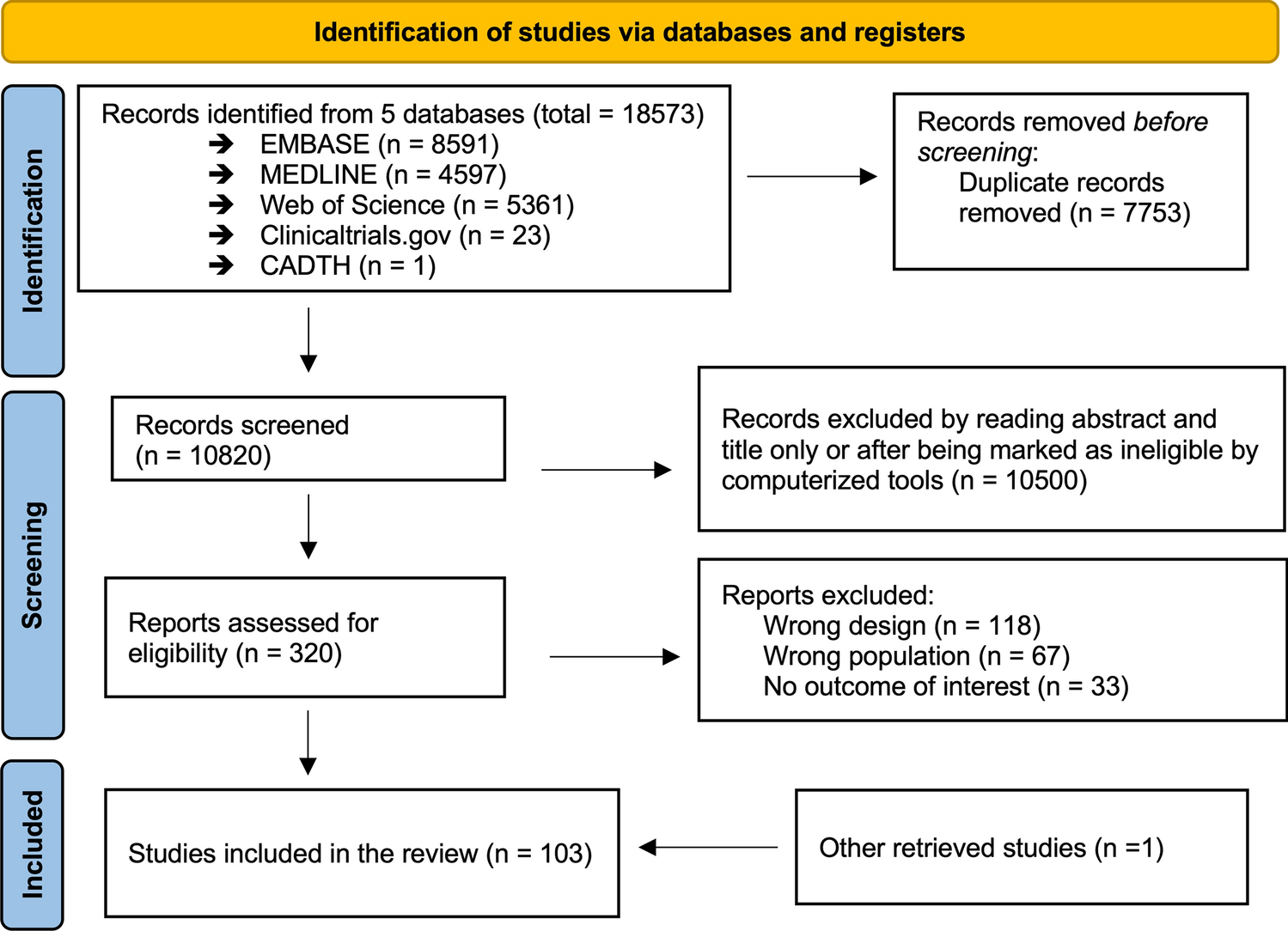
Nasopharyngeal swab PCR for COVID-19 on admission was negative. Blood tests revealed a slightly elevated erythrocyte sedimentation rate (40 mm/h), while the white blood cell count remained within the normal range (6220 /μL with 69.5% neutrophils). Cerebrospinal fluid (CSF) analysis showed a normal cell count (2/μL), along with typical levels of glucose (61 mg/dL) and protein (35 mg/dL). The oligoclonal immunoglobulin G (IgG) band was absent. PCR for herpes simplex virus and varicella zoster virus deoxyribonucleic acid (DNA) in CSF were negative. A variety of tests were performed on serum samples, including those for antinuclear antibodies, anti-ds-DNA, SS-A, SS-B, anti-GM1 IgG antibody, anti-GQ1b IgG antibody, and paraneoplastic antibodies (anti-amphiphysin, anti-CV2, anti-Ma2/Ta, anti-Ri, anti-Yo, anti-Hu, anti-revoverin, anti-SOX1, anti-titin, anti-zic4, anti-GAD65, and anti-Tr antibodies); all yielded negative results. On day 27, a brain MRI showed hyperintensity in the cerebellum on diffusion-weighted imaging (DWI) (Fig. 1). The T2/fluid-attenuated inversion recovery (FLAIR) showed edematous changes with slightly increased signals compared with the adjacent tissue. A whole-body CT scan showed no abnormalities, eliminating the possibility of malignancy.
Fig. 1
MRI findings of the patient. Axial DWI (left), axial T2-weighted image (middle left), and coronal FLAIR images (middle right and right) are shown. The hyperintensity in the cerebellum (arrows in DWI and FLAIR image) and edematous changes (circles in FLAIR image) was resolved after methylprednisolone treatments
Subsequently, two courses of treatment with intravenous methylprednisolone (1 g/day) for 3 days were administered. After the second course, the patient’s cerebellar symptoms gradually improved, and the brain MRI abnormalities resolved (Fig. 1). On day 50, she was transferred to a specialized rehabilitation facility. Subsequent tests performed on the CSF (collected on day 22) yielded positive results for autoantibodies to GluRs (Table 1). Thus, we arrived at a diagnosis of AC associated with autoantibodies to GluRs.
Table 1 Optical density of antibody to GluR
留言 (0)